4719
Automated femoro-tibial cartilage segmentation of OA patients with and without bone abnormality1Centre for Biomedical Engineering, Indian Institute of Technology, New Delhi, India, 2Biomedical Engineering, ASET, Amity University Haryana, Gurgaon, India, 3Mahajan Imaging Centre, New Delhi, India, 4Department of Biomedical Engineering, All India Institute of Medical Sciences, New Delhi, India, 5National Institute of Technology, Kurukshetra, India
Synopsis
The study of knee cartilage under subchondral abnormality is important in osteoarthritis (OA) progression studies. However, cartilage segmentation for patients with Bone-Marrow-Edema (BME) lesion, particularly using radial-search based approach, is erroneous. In this study, a framework for automatic segmentation of femoro-tibial cartilage of OA patients with and without bone abnormality, based on modified radial-search approach and T2-map values is developed. A 2D projected view of T2-map and thickness values of cartilage was generated. Proposed method was successfully applied on 23 MRI patient data. Dice-coefficient for cartilage segmentation was ~82% for OA patients with and without BME lesions.
INTRODUCTION
Accurate knee cartilage segmentation is helpful for quantitative analysis and 2D or 3D visualization of cartilage. In general, manual segmentation is performed, which is quite cumbersome and subjective to errors1. Popular automatic segmentation techniques such as thresholding2, clustering3, active contour4 performs poorly in case of femoro-tibial cartilage segmentation due to the poor contrast with nearby tissues, smaller size and curved shape. Radial-search based approach5, 6 is a semiautomatic approach which provide improved segmentation of cartilage. However, this approach is inefficient in case of patients with Bone-Marrow-Edema(BME) lesion. BME lesion is a common subchondral abnormality present in OA and underneath cartilage behaviour is important for OA studies7. Radial-search approach can be automatized using recently reported automatic seed point selection procedure8. In the current study, an automatic approach based upon modified radial-search method and T2-map is proposed for segmentation of femoro-tibial cartilage in OA patients, and it has been found to be efficient in patients with and without bone abnormality.MATERIALS AND METHODS
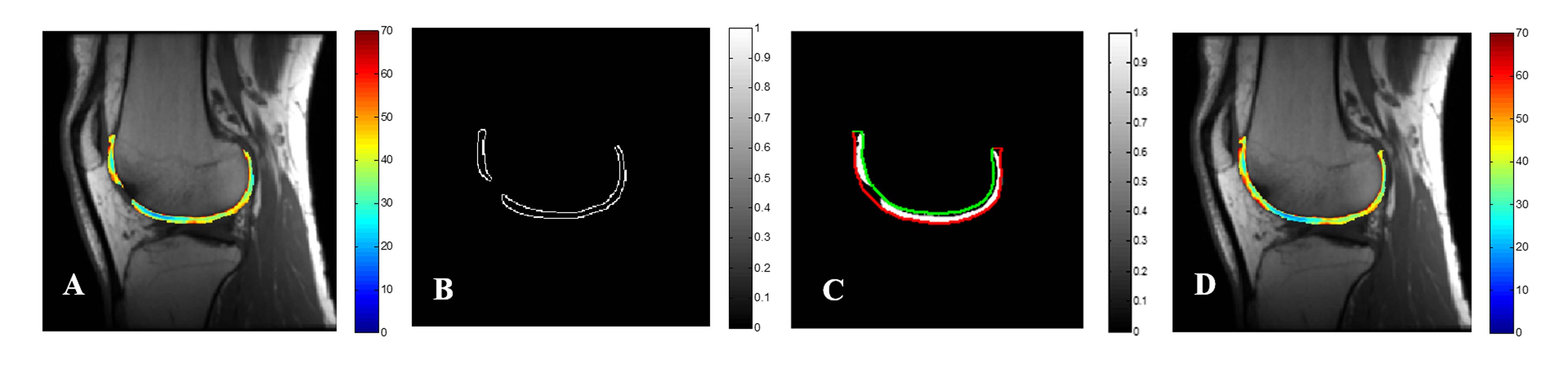
In this study, 23 OA patients data collected retrospectively of which 11 patients had bone abnormalities such as BME like lesions, avascular necrosis, osteophytes etc. Knee joint MRI images were acquired using a 3.0T MRI scanner(GE Healthcare) with eight channel knee transmit-receiver coil. MRI protocol included acquisition of T2-map/CartiGram data: TR=1000ms, TE=6.4, 12.8, 19.2, 25.6, 32, 38.4, 44.8, 51.2ms, Slice-thickness=3mm, Field-of-View(FOV)=140x140mm2, Acquisition-matrix= 256x256. Preprocessing steps such as average filtering, canny edge detection and morphological opening operation were performed as first step on all the datasets. Figure 1 shows the complete segmentation procedure of the proposed method. Inner bone-cartilage boundary points obtained based on inner threshold value(Thresh-1) from the radial outward search, initiated from a seed point placed on the center of both femur and tibial bone. The outer cartilage boundary was obtained based on the same radial approach, that continue from all inner cartilage boundary points using the combination of outer threshold value(Thresh-2) and fixed outer value (determined using maximum possible thickness and resolution). The inner-outer boundary points were connected using cubic spline interpolation and the resultant mask was applied on quantitative T2-map. In T2-map result, T2 value >100ms were thresholded for removing the errors due to chemical shift artefact and to remove synovial fluid presence in segmented cartilage9. Any isolated inner voxels near edge were also removed automatically. In case of OA patient having bone abnormality, the previously proposed algorithm8 fails to segment cartilage next to OA lesions. The proposed method was further modified to automatically take care of this aspect. In such cases, the algorithm automatically connect the neighboring pixels of segmented cartilage using cubic spline for recovering cartilage next to BME lesion. Manual segmentation of the cartilage was performed by an experienced radiologist for validation. Segmentation result were validated statistically by computing Dice-coefficient(DC), Jaccard-coefficient(JC) and Sensitivity measurements. Finally, two separate 2D WearMap5 of T2-map, Thickness map were also generatedRESULTS
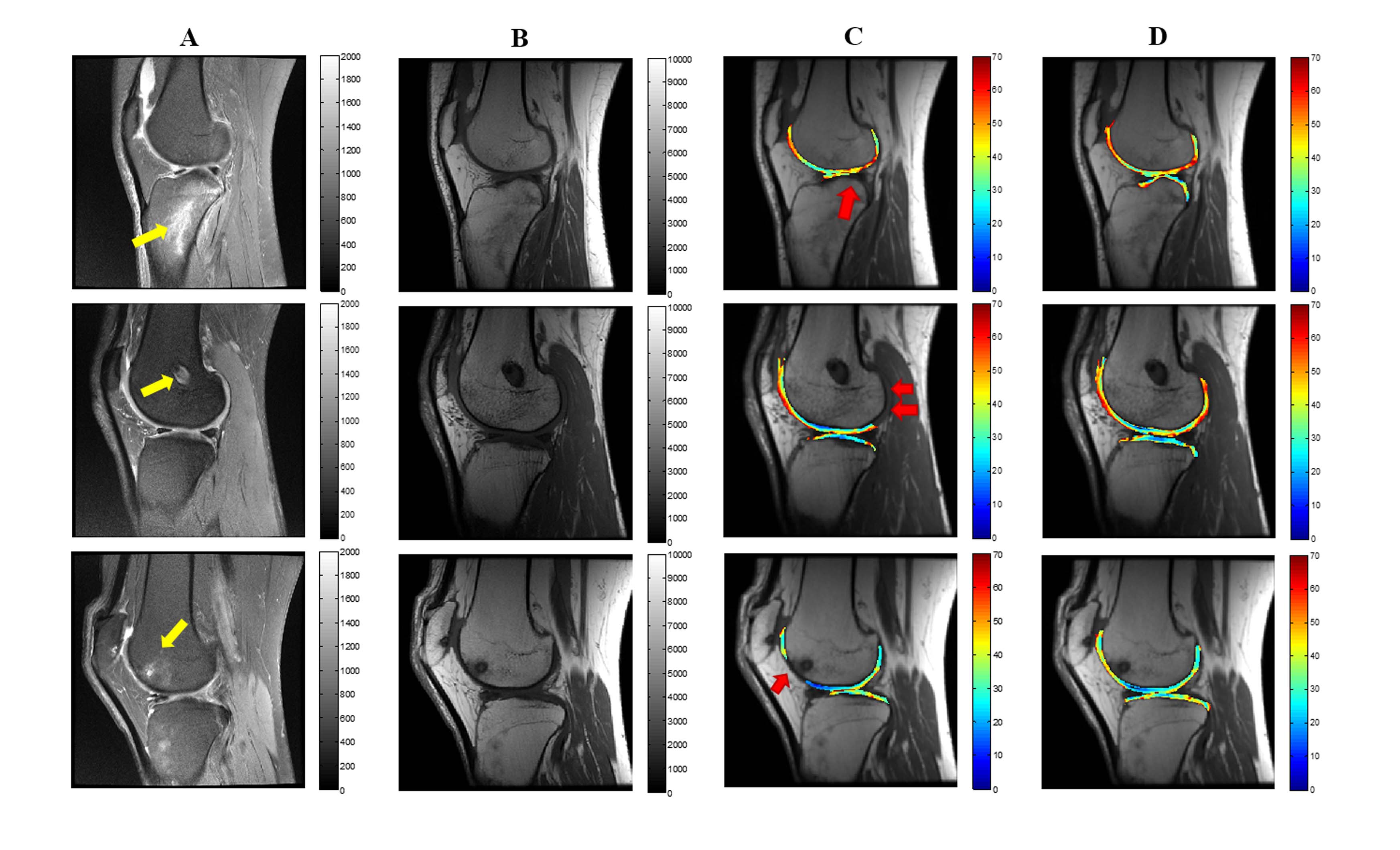
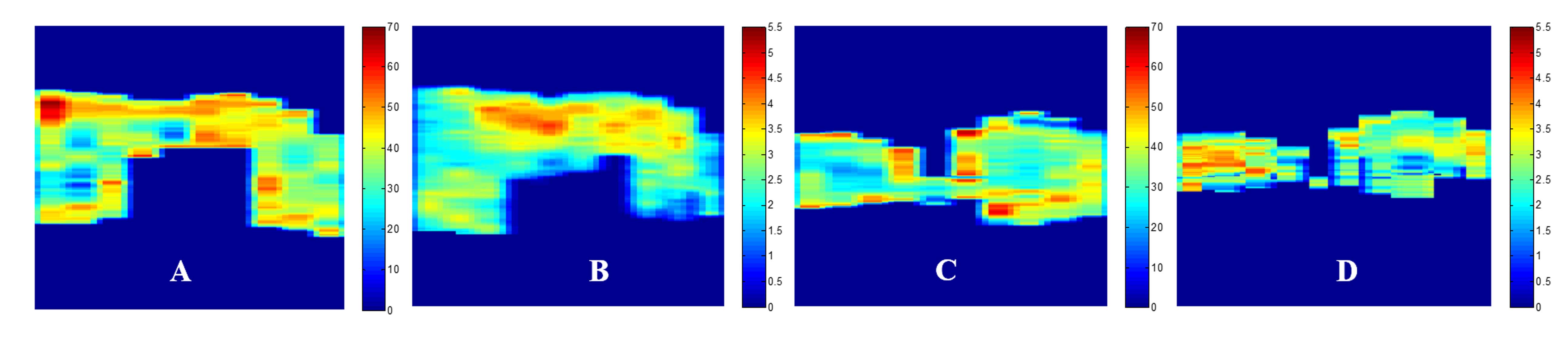
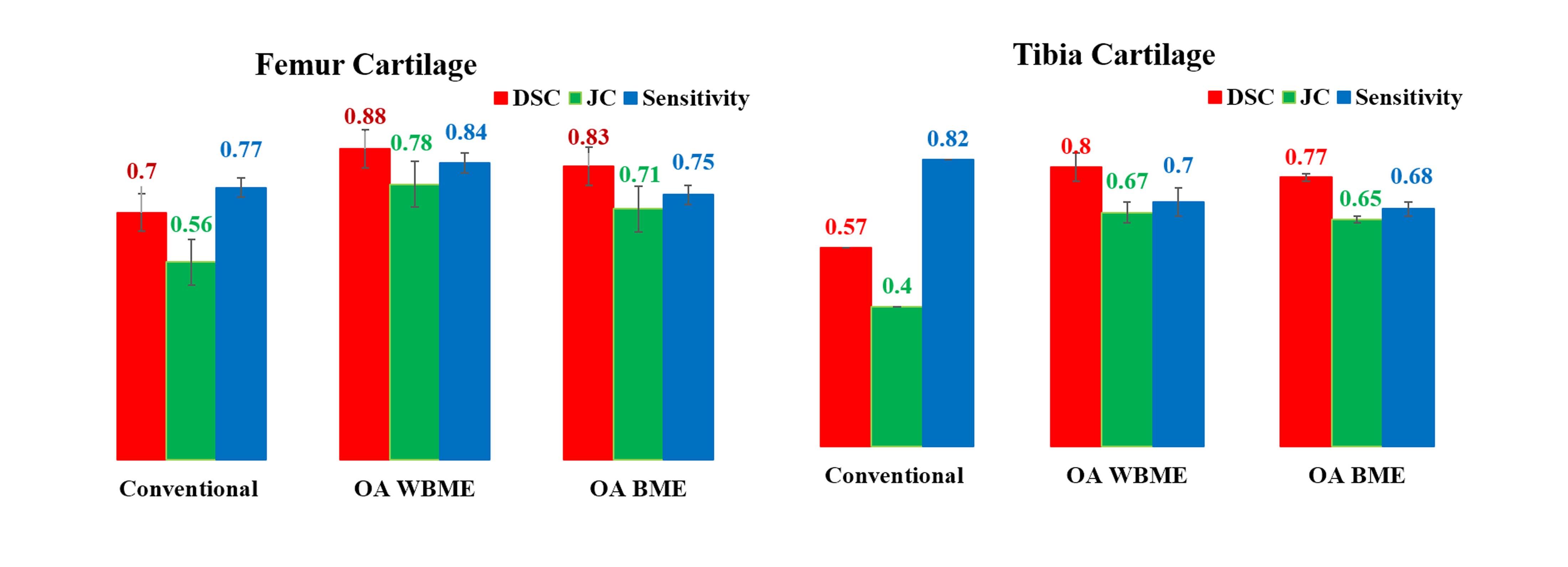
Figure 2 shows the processing steps of automatic detection of missing cartilage in OA patient having severe bone abnormality. In Figure 3, third column represents the poor performance of conventional radial-search method. Figure 4 shows the 2D WearMap results of T2 values and thickness from the femoro-tibial segmentation results using proposed algorithm. Figure 5 shows the statistical evaluation results of femoro-tibial cartilage using conventional radial-search and proposed algorithm. DC for OA patient data without bone abnormality was 88±2% (femur) and 80±4% (tibia). DC for OA patient having bone abnormality was 83±2% (femur) and 77±1% (tibia) respectively.DISCUSSION
The presence of bone abnormalities resulted in inaccurate cartilage segmentation, particularly next to bone abnormality or lesion. In this study, we addressed the challenges of automatic cartilage segmentation in OA patients with bone abnormality using modified radial-search approach and T2-map. The use of same sequence(T2-W and T2-map) in segmentation improved cartilage segmentation and also provided the biochemical information in addition to morphological changes of the tissue. The 2D projected view(2D WearMap) is helpful for easy identification of diseased region and might improve diagnosis. In some subjects, there is chance of cartilage thinning occurs due to the subject life style, hereditary etc. In such cases, the 2D WearMap comparison could be helpful to clinician for taking better decision. That means, the same patient 2D map shows both the high T2 value and low thickness values in a particular area represents more chance of abnormality. One of the limitation of our study is the low resolution of 2D weighted images due to time constraints.CONCLUSION
In this study a modified radial-search approach has been proposed which improved cartilage segmentation, particularly for OA patients with bone abnormalities.Acknowledgements
The authors acknowledge the internal grant support from IRD, IIT Delhi (Project number MI01422). Authors would like to thank Ms. Madhuri Barnwal at Mahajan Imaging Centre for providing the required data.References
1. J. Pang, P. Li et al. J. Digit. Imaging, vol. 28, no. 6, pp. 695–703, 201
2. R. Gonzalez et al. Digital Image Processing, Third Edition, Prentice Hall, pp. 1–976, 2007
3. N. Dhanachandra et al. Procedia Comput. Sci., vol. 54, pp. 764–771, 2015
4. T. F. Chan et al. IEEE Trans. Image Process., vol. 10, no. 2, pp. 266–277, 2001
5. S. Akhtar et al. Osteoarthr. Cartil., vol. 15, no. 9, pp. 1070–1085, 2007
6. M. S. Mallikarjuna Swamy et al. IJBB, Volume (7): Issue (1): 2013
7. Yasuhito Kaneko et al. J Magn Reson Imaging. 2015 December ; 42(6): 1507–1516
8. J A Carrino et al. Osteoarthritis and Cartilage (2006) 14, 1081-1085
9. Sandeep Panwar Jogi et al, Proc. Intl. Soc. Mag. Reson. Med. 26 (2018), 8155
Figures