4682
Improvement of 3D-STIR for TRANCE non-contrast MR angiography at 3T using stretched adiabatic inversion pulseKosuke Morita1, Masami Yoneyama2, Masanobu Nakamura2, Takeshi Nakaura3, Seitaro Oda3, Masahiro Hatemura1, and Yasuyuki Yamashita3
1Radiology, Kumamoto University, Kumamoto-shi, Japan, 2Philips Japan, Tokyo, Japan, 3Diagnostic Radiology, Kumamoto University, Kumamoto-shi, Japan
Synopsis
The purpose of our study was to improve 3D-STIR for TRANCE non-contrast MR angiography in clinical 3.0T MR system using modified hyperbolic secant (HS4) pulses. the higher field strength poses additional challenges to 3D STIR, including wider offset frequency between water and fat combined with larger B0 and B1 inhomogeneities, which reduce the reliability of fat suppression. 3D STIR (TRANCE) with HS4 pulse has clearly improved fat suppression due to B0/B1 inhomogeneous compared with conventional HS pulse in clinical.
INTRODUCTION
ECG-Triggered Non-Contrast-Enhanced MR Angiography (TRANCE1) typically applies 3D short tau inversion recovery (STIR) sequence to effectively suppress background fat signals. 3D STIR basically applies nonselective adiabatic IR pulses such as hyperbolic secant (HS). In fact, the higher field strength poses additional challenges to 3D STIR, including wider offset frequency between water and fat combined with larger B0 and B1 inhomogeneities, which reduce the reliability of fat suppression. The crucial factors of an adiabatic IR pulse to achieve robust fat suppression in 3D TSE-STIR are a broader bandwidth for B0 insensitivity and a lower adiabatic threshold for B1 insensitivity, which are challenging to achieve simultaneously with the HS pulse2 [Fig.1]. To improve the reliability of HS pulse, several alternatives including a derivative of the HS pulse, called a stretched HS pulse, have been proposed for T1rho studies3,4. Furthermore, broadband STIR pulse with increased robustness to B0 and B1 inhomogeneities at 3T for brachial plexus imaging has also been demonstrated recently2. Therefore, we attempt to use stretched HS pulse for 3D STIR on 3.0T. The purpose of our study was to improve fat suppression in TRANCE on clinical 3.0T MR using stretched HS pulses.MATERIALS AND METHODS
Experimental data was collected from 5 healthy volunteers. Written informed consent was obtained from each volunteer and the protocol was approved by the ethics committee. All studies were performed with clinical 3.0T MR scanner (Philips, Ingenia 3.0T CX) and 32-channel dS-torso coil. Scan parameters of 3D STIR using HS pulses were as follows: TR / TE / TI = 2000 / 100 / 220 ms, slices thickness = 2.0 mm, number of slices = 50, field-of-view = 40 × 40 cm2, acquisition matrix = 320 × 320 (reconstruction matrix = 512× 512), NSA = 1, TSE factor = 30, echo space = 5.4 ms, Compressed Sense (CS) factor = 8.0, Acquisition time = 4:40, Coronal plane acquisition. Mean measured values were measured in the regions of interest (ROI) on 3D STIR images with default IR pulse (conventional HS) and stretched HS pulse (broadband HS). We determined the HSn pulse using Eq.(1). The amplitude and orientation are time dependent and these in turn are functions of the amplitude modulations and frequency modulations used for the pulse. One way to alter the modulations is to change the stretching factor, n. Accordingly, the amplitude modulation function of the HSn pulse becomes flatter as the factor n increases as given by ω1(t) = ω1maxsec h(βτn) … (1) where ω1max is the maximum pulse amplitude in rad per sec and β is a constant. When n=1, the pulse is the original hyperbolic secant pulse5, whereas when n > 1, a stretched version of the pulse is produced6. In the experiments performed here, HSn pulse parameters was held constant except for the stretching factor (n =4). Fig.2 shows actual RF perfomance for conventional HS and broadband HS4 pulse.RESULTS
Figure 3 shows the representative images for upper extremity and lower extremity. Fat suppression failure due to B1 inhomogeneous appeared on conventional HS images (arrows). In contrast, broadband HS4 uniformly suppressed background fat sugnals. Figure 4 shows clinical case for elbow soft tissue tumor. TRANCE MIP image demonstrated more detailed blood vessel information around the tumor with clear fat suppression.CONCLUSION
3D STIR (TRANCE) with HS4 pulse has clearly improved fat suppression due to B0/B1 inhomogeneous compared with conventional HS pulse on 3.0T MR system. It may facilitate the detection of small vessel lesion existing in the extremities even with B0/B1 inhomogeneity.Acknowledgements
No acknowledgement found.References
[1] Gutzeit a, et al. Eur Radiol 21:1979–1987, 2011. [2] Wang X, et al. J Magn Reson Imaging 48:1104-1111, 2018. [3] Jokivarsi KT, et al., Journal of Cerebral Blood Flow & Metabolism 29:206-216; 2009. [4] Okuaki T et al., Proc. Intl. Soc. Mag. Reson. Med. 21:4093, 2013. [5] Silver MS, et al. Magn Reson Med 29:688-691; 1993. [6] Tannus A et al. J Magn Reson A 120:133-137; 1996.Figures
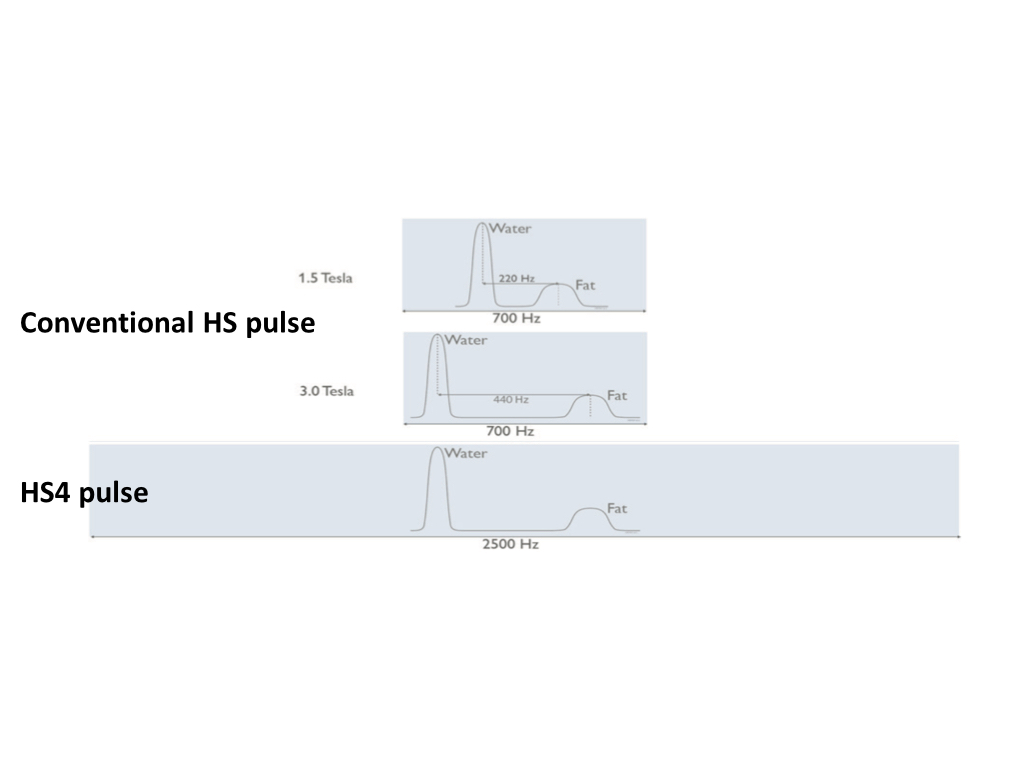
Figure 1. Performance of Conventional HS pulse and HS4
pulse.
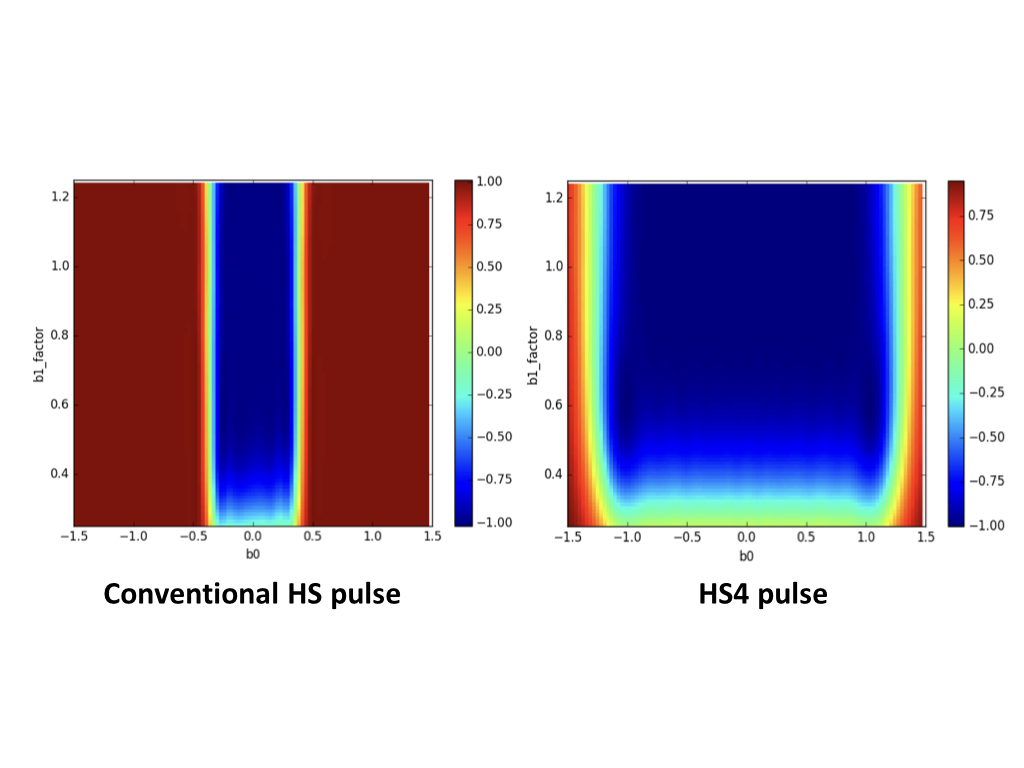
Figure 2. Simulation of B1 and B0
fields for conventional HS pulse and HS4 pulse.
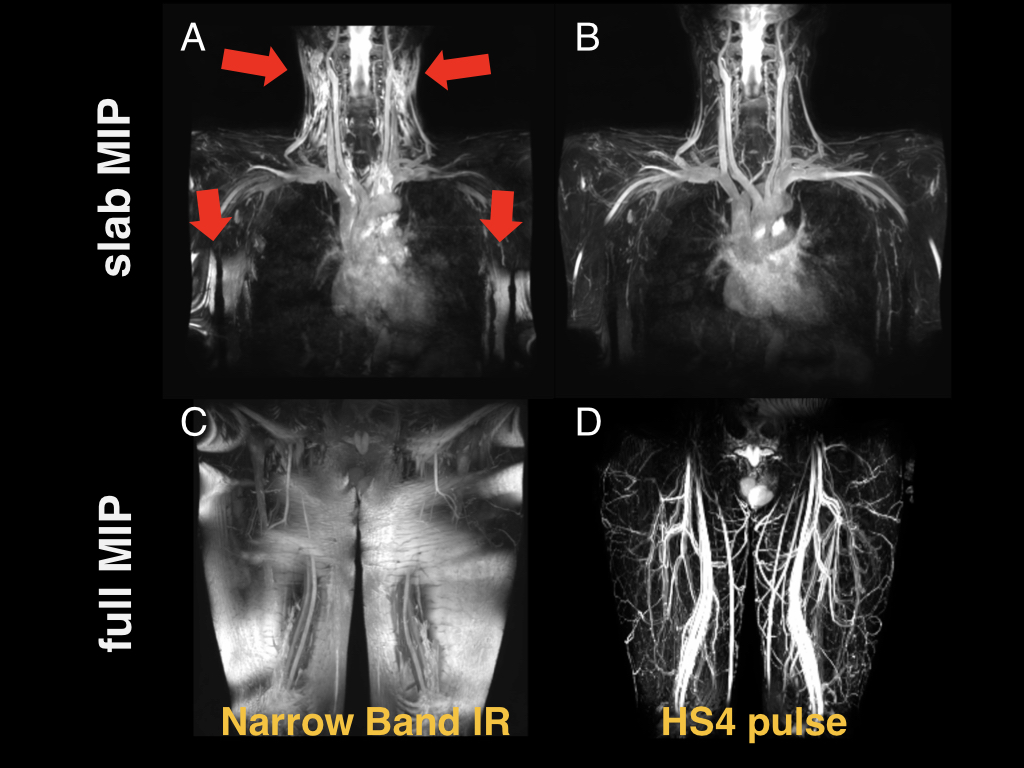
Figure 3. Volunteer
images. Slab MIP (A,B) and full MIP (C,D) show upper extremity (above) and
lower extremity (below). Red arrows show
B1 inhomogeneity area.
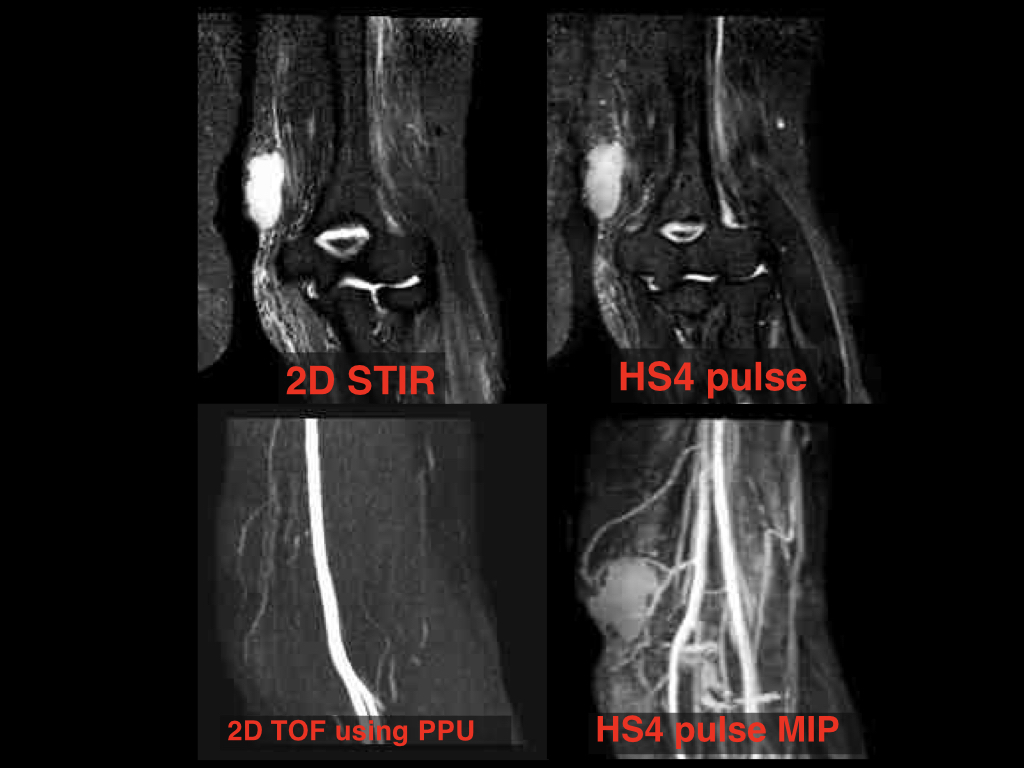
Figure. 4 Elbow
with soft tissue tumor patient.