4637
Improving pseudo-continuous arterial spin labelling at ultra-high field using a VERSE-guided parallel transmission strategy1Wellcome Centre for Integrative Neuroimaging, FMRIB Division, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
Synopsis
Implementing ASL at ultra-high field is challenging due to increased specific absorption rate (SAR), along with B1+ and B0 inhomogeneity. Parallel transmission (pTx) provides additional degrees of freedom to mitigate B1+ inhomogeneity. Among various pTx strategies, RF shimming is a simple formulation that modulates the complex weights of each RF channel. In this study, we explored the possibility of using VERSE to further improve PCASL at 7T, and VERSE-guided RF shimming was shown to achieve improved SNR in perfusion-weighted images over power-matched Circularly-Polarised (CP) mode and RF-shimmed Gaussian labelling schemes.
Introduction
Arterial spin labelling (ASL) is a commonly used non-invasive perfusion imaging technique. Among various labelling approaches, pseudo-continuous ASL (PCASL) was recommended by the ASL consensus paper1. Yet its implementation at ultra-high field (UHF) is not trivial. The specific absorption rate (SAR) scales quadratically with B0, limiting the permitted labelling pulse train duration and amplitude2. Additionally, increased B1+ and B0 inhomogeneity at UHF leads to further decreases in labelling efficiency, diminishing the perfusion signal2.
Parallel transmission (pTx) provides more degrees of freedom that allow for constructive and destructive interference of different radio-frequency (RF) waveforms to mitigate B1+ inhomogeneity. RF shimming, or “static pTx”, is a simple formulation that modulates the complex weights of each RF channel, and has been shown to improve PCASL at 7 T3. To address the SAR problem, Variable-Rate Selective Excitation (VERSE) can also be employed during the labelling period. VERSE is a technique that reduces SAR without compromising the slice profile4,5. In this study, we present a VERSE-guided RF shimming strategy to further improve PCASL at UHF.
Methods
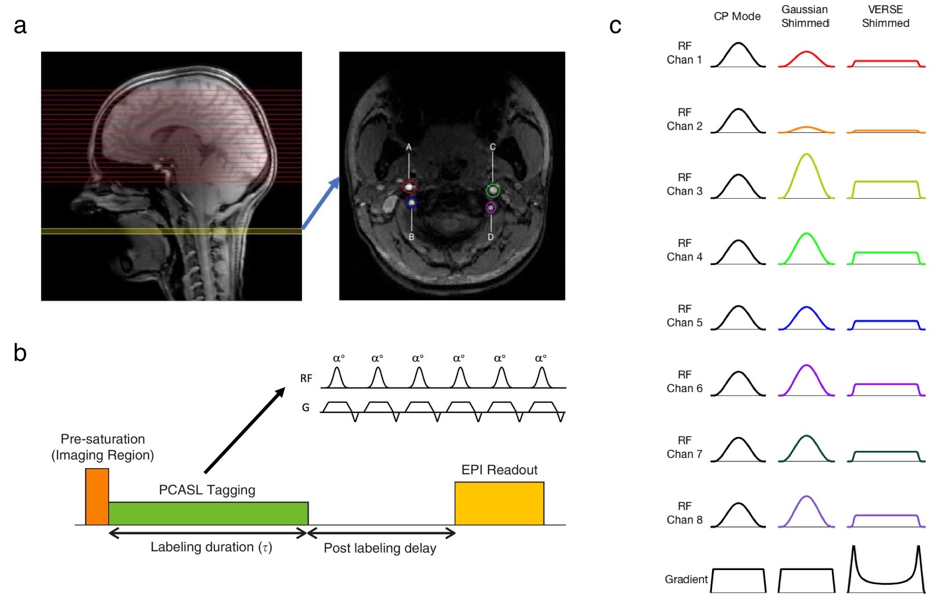
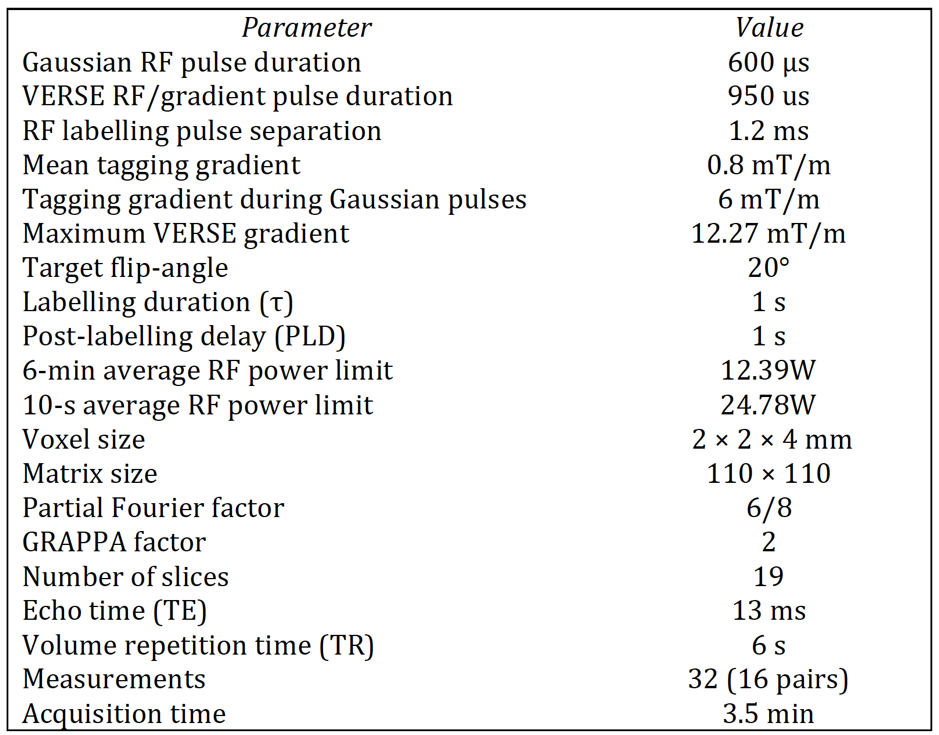
The PCASL sequence consisted of a train of 833 pulses, separated by 1.2 ms, to give an overall PCASL labelling duration of 1.0 second (see Fig. 1). After a post-label delay of 1.0 second an EPI readout was used to acquire the labelled and control data. To minimise SAR no background suppression pulses were used. Additionally, an M0 image with no labelling was acquired for perfusion quantification.
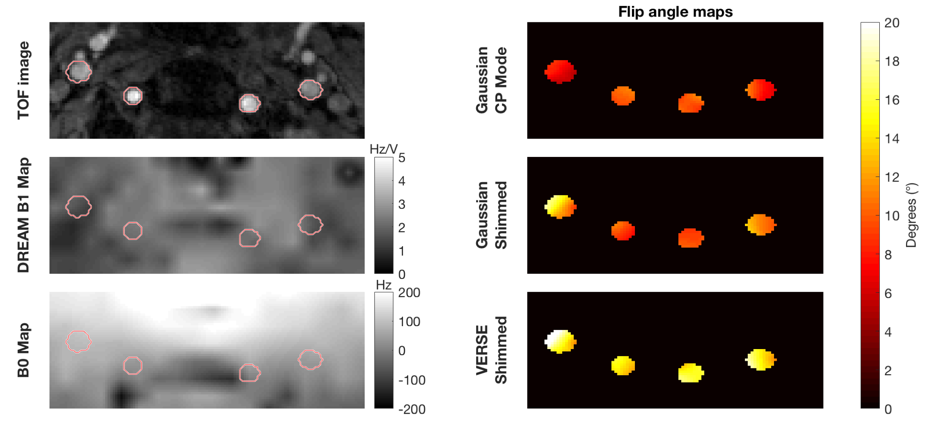
Perfusion-weighted images were acquired from six subjects (1F, age: 32.3±10.1) on a Siemens (Erlangen, Germany) Magnetom 7 T scanner equipped with an 8 channel pTx system, and a Nova Medical Inc. (Wilmington MA, USA) 8Tx32Rx head coil. B1+ maps were acquired using a 2D “STE first” phase-cycled DREAM sequence6,7. B0 maps were acquired using a dual-echo gradient-echo sequence. A time-of-flight (TOF) sequence was used to identify the four principal arteries that feed the brain in the labelling plane, and four elliptic regions of interest (ROIs) were manually selected around the vessels as the RF shimming regions (see Fig. 2). Sequence parameters are provided in Table 1.
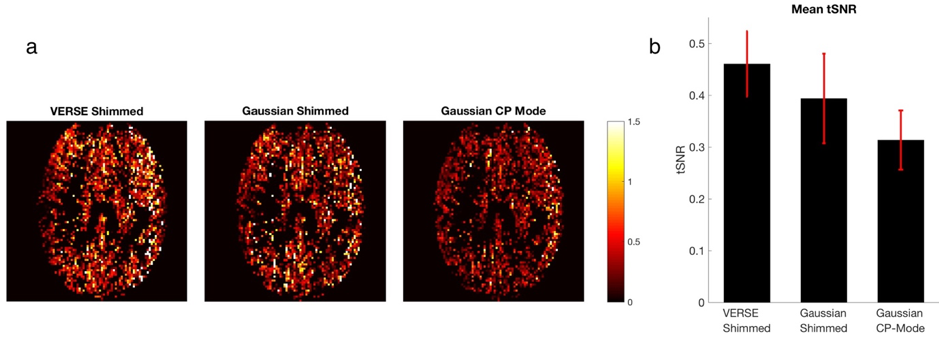
The flip-angle optimisation strategy was identical to that in a similar preliminary study3, which was based on a method by Dupas et al.8 VERSE RF and gradient pulses were obtained using an approach proposed by Hargreaves et al.5 A target power reduction factor of 50% was set, and this required elongation of the RF pulse (600 us to 950 us). Bloch simulation9 was performed to characterise the slice profile produced by VERSE pulses under different B0 off-resonances. Cerebral blood flow (CBF) was calculated using a method by Buxton et al.10 with an assumed 7T arterial blood T1 value of 2587 ms11. Voxel-wise temporal signal-to-noise ratio (tSNR) of the central slice was calculated as the mean divided by the standard deviation of the perfusion signal across measurements.
Results
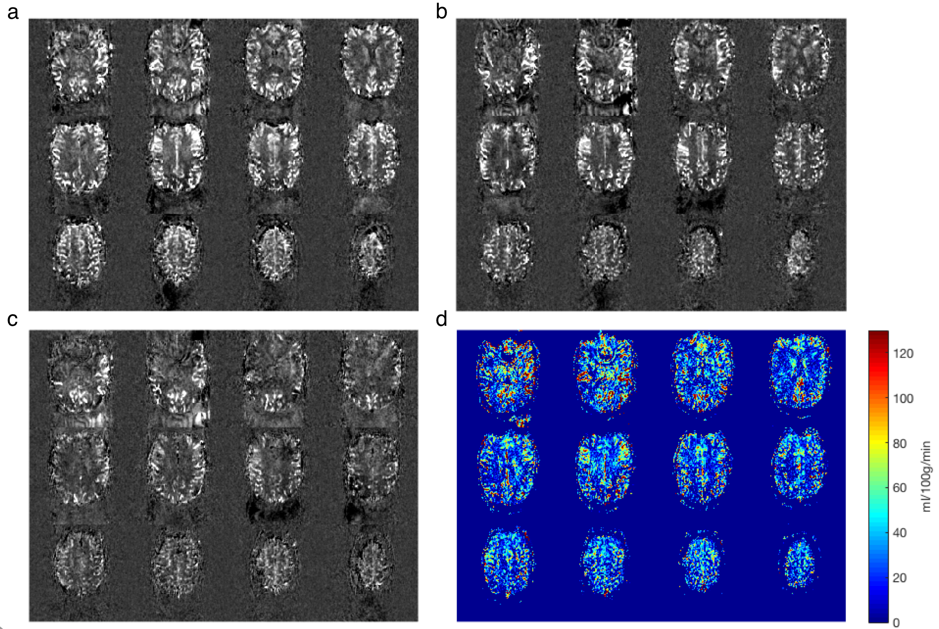
Simulation results showed that there was minimal contamination of VERSE slice profile in the presence of off-resonance. In vivo experiments showed that VERSE shimming produced perfusion-weighted images with higher contrast than Gaussian RF shimming and Gaussian Circularly-Polarised (CP) mode in all subjects except one. CBF measurements calculated from perfusion-weighted images using VERSE shimming were qualitatively comparable to literature values10 (see Fig. 3). Mean tSNR values of all subjects were as follows: VERSE shimming (0.460±0.063), Gaussian shimming (0.394±0.087), and Gaussian CP Mode (0.314±0.056). VERSE shimming achieved a 47% and 17% improvement in tSNR compared to CP mode and Gaussian shimming, respectively (see Fig. 4). VERSE shimming achieved a greater consistency in tSNR compared to Gaussian shimming.Discussion
Unlike dynamic pTx, RF shimming does not involve calculation of a full RF waveform, nor optimisation of the gradient trajectory. Nevertheless, RF shimming provided significantly improved results when utilised in the small ROIs, and with short calculation time. Replacing Gaussian RF pulses and trapezoidal gradients with VERSE RF and gradient waveforms further improved the RF efficiency, allowing for higher-flip-angle labelling pulses to be achieved in the labelling plane under the same RF power limit.
Since B1+ maps were collected, we could predict flip-angles in all vessels, which allows for more accurate CBF quantification. However, even though perfusion signal could be enhanced by adopting VERSE, homogenous excitation at the target flip-angle of 20° was not achieved in subjects with low B1+ at the labelling plane. Local SAR monitoring using virtual observation points (VOPs) would allow for less stringent RF power limits, and thus higher and more uniform flip-angles in the labelling vessels.
Conclusion
We have demonstrated the feasibility of improving PCASL using VERSE-guided RF shimming at 7 T.Acknowledgements
This study was supported by China Oxford Scholarship Fund, Medical Research Council (MRC), the Royal Academy of Engineering, Dunhill Medical Trust, and the NIHR Oxford Health Biomedical Research Centre. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).References
1. Alsop, D.C., et al., Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med, 2015. 73(1): p. 102-16.
2. Teeuwisse, W.M., A.G. Webb, and M.J.P. van Osch, Arterial spin labeling at ultra-high field: All that glitters is not gold. International Journal of Imaging Systems and Technology, 2010. 20(1): p. 62-70.
3. Tong, Y., et al. Improving arterial spin labeling at ultra-high field using parallel transmission: a simulation study. in Proceedings of the 27th Scientific Meeting, ISMRM. 2018. Paris.
4. Conolly, S., et al., Variable-Rate Selective Excitation. Journal of Magnetic Resonance, 1988. 78(3): p. 440-458.
5. Hargreaves, B.A., et al., Variable-rate selective excitation for rapid MRI sequences. Magn Reson Med, 2004. 52(3): p. 590-7.
6. Nehrke, K. and P. Bornert, DREAM--a novel approach for robust, ultrafast, multislice B(1) mapping. Magn Reson Med, 2012. 68(5): p. 1517-26.
7. Tse, D.H., et al., Encoding methods for B1(+) mapping in parallel transmit systems at ultra high field. J Magn Reson, 2014. 245: p. 125-32.
8. Dupas, L., et al., Two-spoke placement optimization under explicit specific absorption rate and power constraints in parallel transmission at ultra-high field. Journal of Magnetic Resonance, 2015. 255: p. 59-67.
9. Bloch, F., Nuclear Induction. Physical Review, 1946. 70(7-8): p. 460-474.
10. Buxton, R.B., et al., A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med, 1998. 40(3): p. 383-96.
11. Rooney, W.D., et al., Magnetic field and tissue dependencies of human brain longitudinal 1H2O relaxation in vivo. Magn Reson Med, 2007. 57(2): p. 308-18.
Figures