4607
Novel use of the MAVRIC metal artifact reduction technique in MRI of the brain1Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
While multiacquisition variable-resonance image combination (MAVRIC) is a recognized technique for metal artifact reduction in muskuloskeletal MRI, it is not widely described for MRI of the central nervous system. We investigate the value of this technique for MRI of the brain in patients with MR conditional metal implants and find that MAVRIC-T1 is superior to conventional FSE T1 in both qualitative and quantitative metrics.
Introduction
MR imaging of patients with metal hardware is challenging due to metal susceptibility artifact, which degrades signal in adjacent tissue. This is particularly problematic in imaging of oncology patients wherein small lesions may be obscured. Commercially available metal artifact reduction sequences, such as multiacquisition variable-resonance image combination (MAVRIC), are designed to minimize the region of artifact created by metal devices.1 While the utility of MAVRIC has been evaluated in muskuloskeletal MRI 2-4, this technique has not been widely described for use in MR imaging of the central nervous system. In this study, we assess the utility of the MAVRIC-T1 sequence for metal artifact reduction in MRI of the brain.Methods
Brain MRIs including MAVRIC performed for oncologic treatment evaluation were retrospectively reviewed. Ten consecutive patients imaged with non-removable, MR conditional metal hardware in or near the field of view (dental hardware = 7, ventriculoperitoneal shunt = 2, Ommaya reservoir = 1) will be presented. All studies were performed without and with intravenous gadolinium-based contrast and included both conventional fast spin echo (FSE) T1 and MAVRIC-T1 post-contrast sequences. Both the FSE and MAVRIC-T1 sequences were obtained using 1.5-T scanners (Signa 450w, GE Healthcare, Milwaukee, WI) with the patient in the supine position. The MAVRIC protocol was a 3D fast spin echo acquisition (TR/TE: 527/7 ms; slice thickness: 3-5 mm; gap: 0.8 mm; field of view: 240 mm; 30 slices; matrix: 256x192; flip angle: 110 degrees; bandwidth 976 Hz).
Corresponding images from each sequence were qualitatively and quantitatively compared. For qualitative evaluation, 2 neuroradiologists reviewed blinded representative images of the two comparison sequences, grading on 3 criteria: visualization of the metal-tissue interface, image blurring, and overall image quality/preferability. A 5-point scale (from -2 to +2) as described by Gutierrez et al.5 was used for grading. Briefly, +2 indicates that MAVRIC was significantly better and +1 indicates that MAVRIC was somewhat better than the FSE sequence; likewise a negative score indicates that the FSE sequence was superior. Quantitative analysis entailed measurement of the maximum cross-sectional area of peri-hardware artifact and was conducted using TeraRecon iNtuition software (TeraRecon, Foster City, CA). The region of metal artifact was defined as the area of signal loss or geographic distortion adjacent to the metal device. Statistical comparison of the artifact areas was performed using the Wilcoxon test.
Results
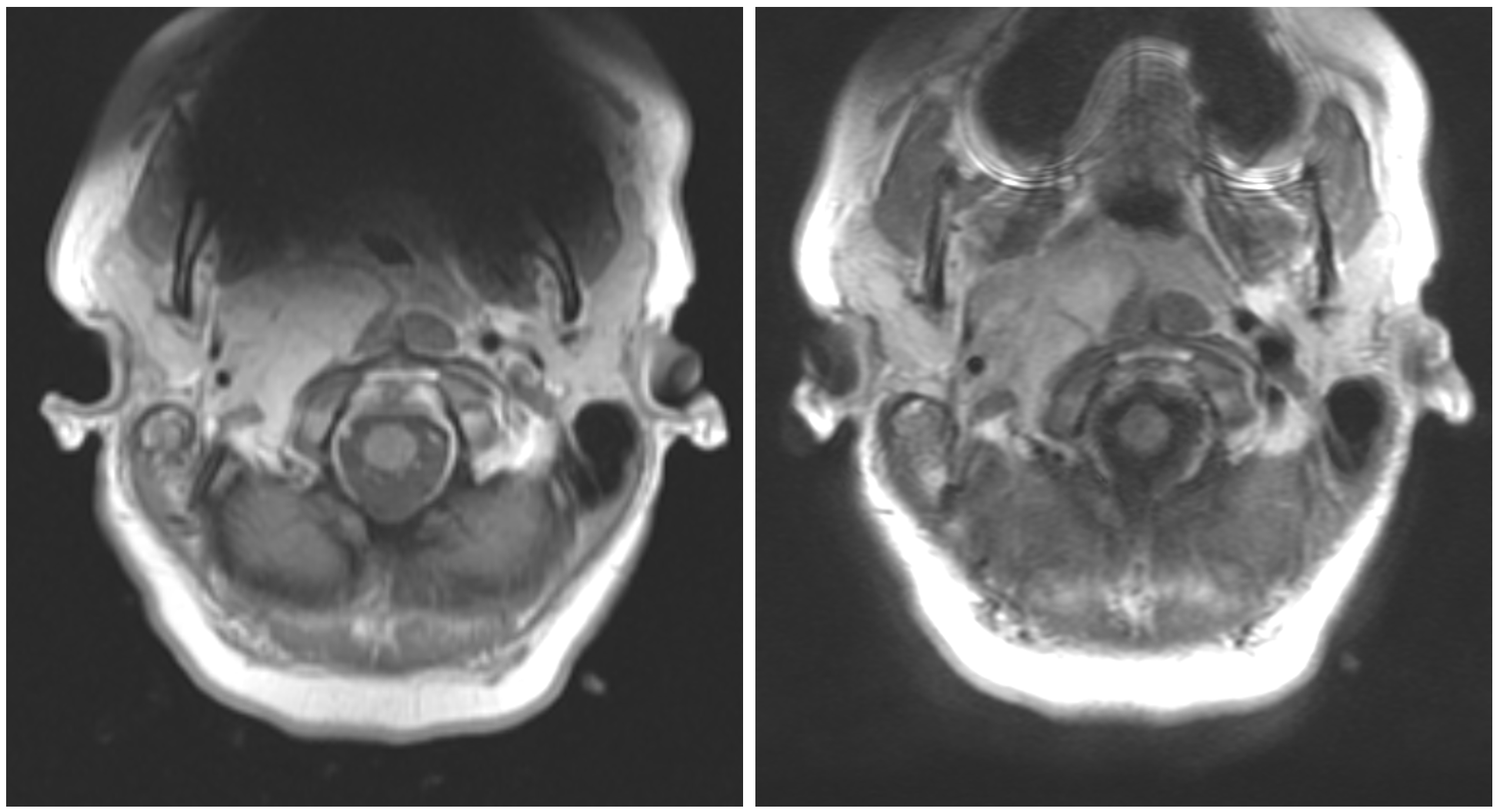
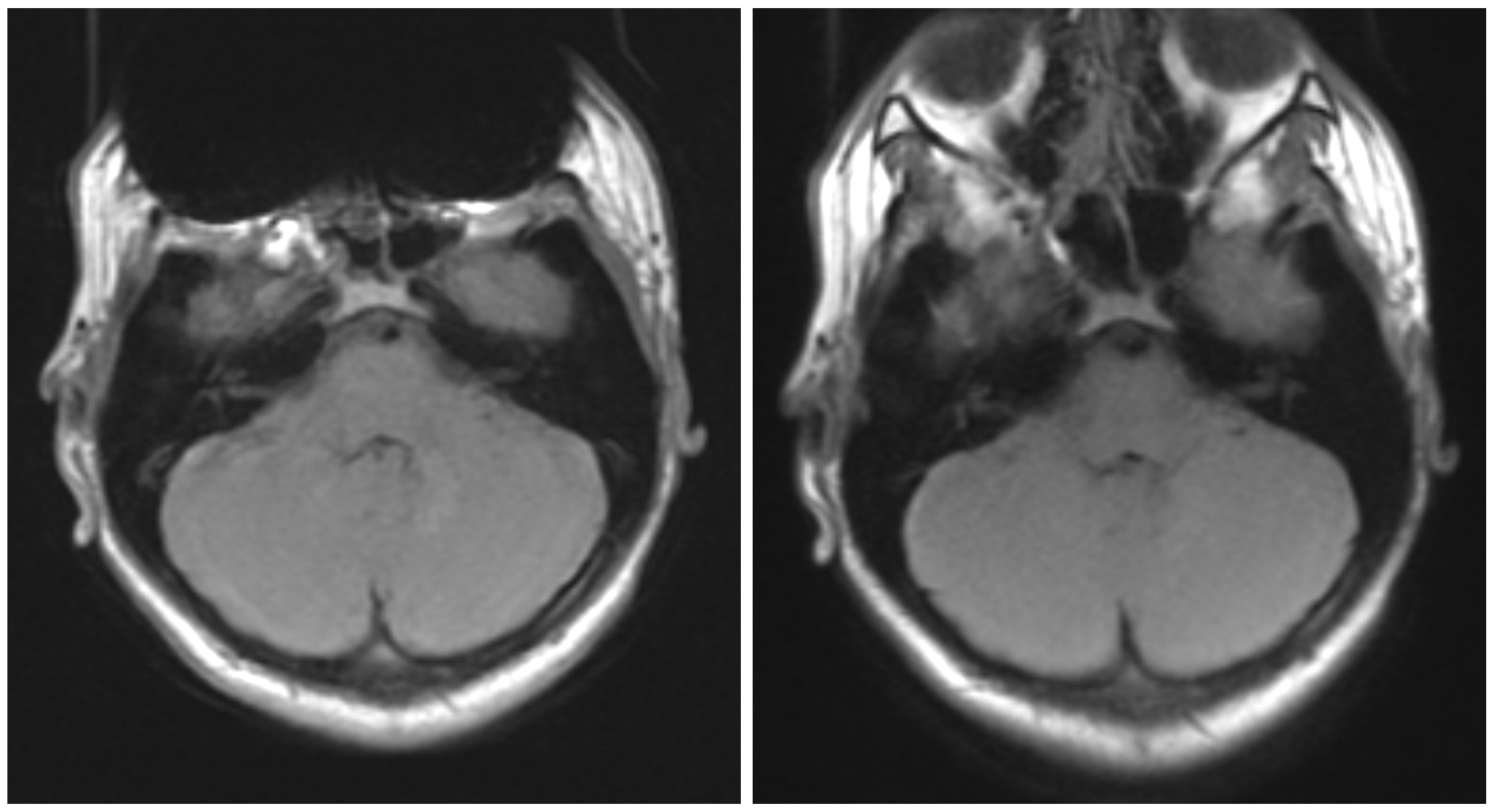
On qualitative assessment, MAVRIC-T1 was superior to FSE with respect to visualization of the metal-tissue interface (mean +1.06) and overall image quality/preferability (mean +1.06). MAVRIC was graded as minimally better than FSE in terms of image blurring (mean +0.11). Quantitative analysis demonstrated a marked superiority of MAVRIC over FSE, with the region of metal artifact measuring 7.87 ± 6.09 vs 27.2 ± 24.9 cm2 (p = 0.008). Representative images are included in Figures 1 and 2.Conclusions
These results suggest that MAVRIC-T1 is superior to conventional T1 FSE for MRI of the brain performed on patients with non-removable, MR conditional metal hardware in the head and neck. Further investigation is required to quantify the clinical value of MAVRIC for improved lesion detection in these patients.Acknowledgements
No acknowledgement found.References
- Koch KM, Lorbiecki JE, Hinks RS, King KF. A multispectral three-dimensional acquisition technique for imaging near metal implants. Magn Reson Med. 2009;61(2):381–90. doi: 10.1002/mrm.21856.
- Kretzschmar M, Nardo L, Han MM, Heilmeier U, Sam C, Joseph GB, et al. Metal artefact suppression at 3 T MRI: comparison of MAVRIC-SL with conventional fast spin echo sequences in patients with Hip joint arthroplasty. Eur Radiol. 2015;25(8):2403–11.
- Choi SJ, Koch KM, Hargreaves BA, Stevens KJ, Gold GE. Metal artifact reduction with MAVRIC SL at 3-T MRI in patients with hip arthroplasty. AJR Am J Roentgenol. 2015;204(1):140–7.
- Susa M, Oguro S, Kikuta K, et al. Novel MR imaging method--MAVRIC--for metal artifact suppression after joint replacement in musculoskeletal tumor patients. BMC Musculoskelet Disord. 2015;16:377. doi:10.1186/s12891-015-0838-1
- Gutierrez LB, Do BH, Gold GE, Hargreaves BA, Koch KM, Worters PW, et al. MR imaging near metallic implants using MAVRIC SL: initial clinical experience at 3T. Acad Radiol. 2015;22(3):370–9. doi: 10.1016/j.acra.2014.09.010.
Figures