4603
Comparison of Accelerated MAVRIC-SL with Robust-PCA and Conventional MAVRIC-SL in Evaluation of Symptomatic Total Hip Arthroplasties1Stanford University, Stanford, CA, United States
Synopsis
The substantial reduction of off-resonance artifacts near metal by multi-spectral imaging sequences facilitates the postoperative use of MRI to evaluate total hip arthroplasty patients, but its long scan time can be difficult for patients to tolerate. A novel MAVRIC-SL method using robust principal component analysis (RPCA) recently showed 2.6-fold reduced scan time with comparable artifact suppression. In this study we compare a conventional MAVRIC-SL method with the RPCA-accelerated MAVRIC-SL method in 36 total hip arthroplasty cases. Our data demonstrate nearly equivalent clinical sensitivity of the RPCA MAVRIC-SL method to the conventional method with a mild loss of spatial resolution.
Introduction
In the past several years, a number of novel MRI sequences, including MAVRIC-SEMAC hybrid (MAVRIC-SL)1, have demonstrated substantial suppression of severe off-resonance artifacts near metallic implants1-4, facilitating the use of MRI for the postoperative evaluation of symptomatic total hip arthroplasties. However, the additional slice-encoding process adopted in these techniques results in a long scan time, which can be difficult for patients to tolerate and in turn may introduce motion. Recently, a robust principal component analysis (RPCA) approach was introduced to accelerate MAVRIC-SL by exploiting the redundancy of the spectral bins and sparsity of off-resonance signals. It demonstrated the feasibility of implementing acceleration factors previously unachievable5. In this study, RPCA MAVRIC-SL was compared to conventional MAVRIC-SL in the radiologic evaluation of painful total hip arthroplasties.Methods
After IRB approval, proton-density-weighted coronal MAVRIC-SL and RPCA MAVRIC-SL images were obtained on a GE Discovery MR750 3T scanner (GE Healthcare, Waukesha, WI) in 25 patients (aged 52-82 years) with 36 total hip replacements (18 right, 18 left) using a 32-channel body coil. The scan parameters were as follows: TR/TE 4s/6.6ms, FOV 36x36x9.6cm, matrix 384x256x24, ETL 20, 2x2 parallel imaging for the conventional MAVRIC-SL (6 minute scan time), complementary Poisson-disc sampling for the RPCA MAVRIC-SL (2.3 minute scan time). Each sequence was independently reviewed by two experienced musculoskeletal radiologists and scored on a 5-point scale for overall image quality, geometric distortion, and visualization of the femur and acetabulum using a 5 point scale (5 = excellent, 1 = poor). The total extent of metallic artifact was quantitatively measured using an ROI drawn on the slice where susceptibility artifact was maximal. Clinical pathology was evaluated using a 4 point scale (1=definitely no pathology, 2=probably no pathology, 3=probable pathology, 4=definite pathology). The Wilcoxon signed-rank test was used to determine the statistical difference between the scores. The maximum margin that still accepts the null hypothesis that the conventional MAVRIC-SL score is larger than “RPCA MAVRIC-SL score + margin” is estimated as the statistically significant margin between the scores of the two methods. Interobserver agreement was determined by calculating the weighted Cohen’s kappa coefficient.Results
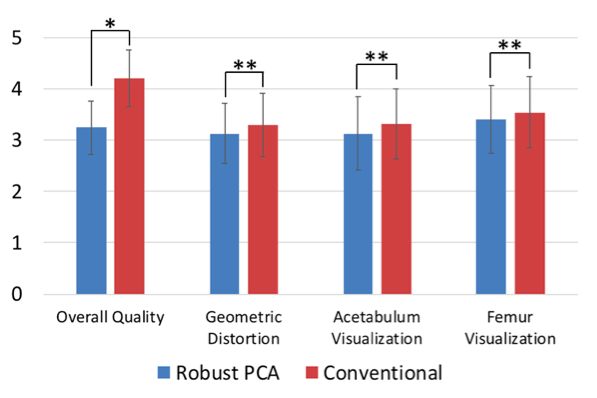
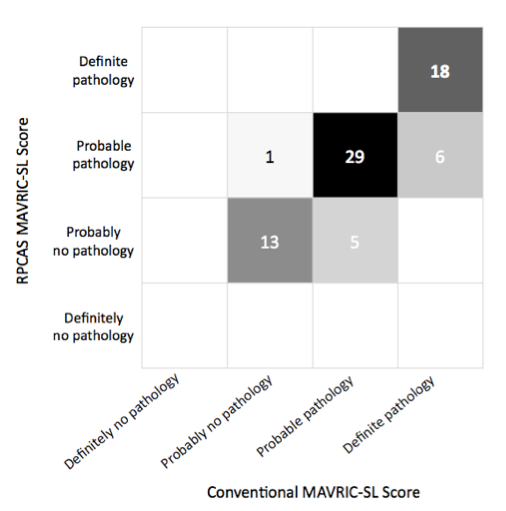
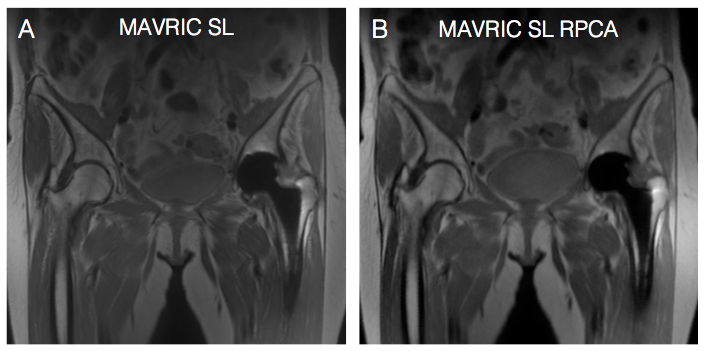
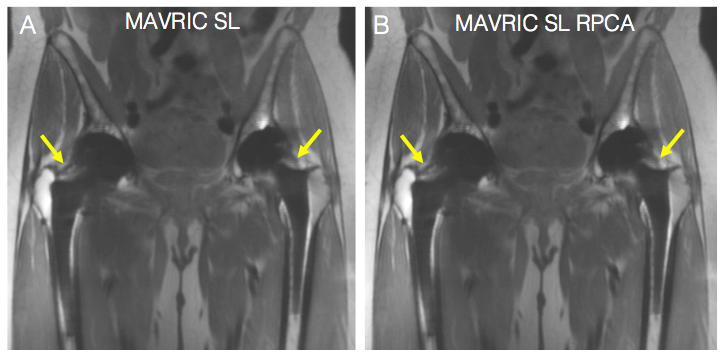
Mean scores for conventional MAVRIC-SL were higher compared to RPCA MAVRIC-SL for all qualitative parameters with a p-value of <0.05 (Figure 1). However, non-inferiority testing demonstrated that the mean score difference was < 1 for overall quality and <0.1 for the other tested parameters (Figure 1). Interobserver agreement ranged from 0.6-0.91. The extent of artifact measured using an ROI was not found to be statistically different between the two methods (p = 0.07). For visualization of pathology, each individual observer gave identical scores for conventional MAVRIC-SL vs RPCA MAVRIC-SL in 27 out of the total 36 cases (Figure 2). In 4 out of 36 cases, at least one observer gave slightly differing pathology scores between the conventional MAVRIC-SL and RPCA MAVRIC-SL of 2 (probably no pathology) and 3 (probably pathology). Figures 3-5 show examples of the two MRI imaging techniques shown side by side with corresponding scores.Discussion
Our results show that there is a mild reduction in spatial resolution with RPCA MAVRIC-SL compared to conventional MAVRIC-SL. Subjective geometric distortion from metallic artifact is minimally greater with the RPCA technique, although differences are almost negligible. In the majority of cases, clinical pathology was equally visible using both techniques. In the remaining cases, small joint effusions were seen with a slightly higher degree of confidence in the conventional technique, although this remains a relatively subjective diagnosis. Compared to conventional MAVRIC-SL, the RPCA approach allows for 2.6-fold faster scanning time, reducing discomfort for patients who experience pain during the scan. Given how frequently patients are unable to complete a full MRI exam or are unable to lay still without introducing motion artifact, this new accelerated technique can also make the difference in whether a full set of diagnostic images is acquired, as well as potentially increasing patient throughput.Conclusion
We compared the recently developed RPCA MAVRIC-SL method which allows for accelerated scan time with the conventional MAVRIC-SL technique in patients with metal hip implants. We conclude that while spatial resolution is mildly reduced, the new technique allows for significantly reduced scan time while maintaining nearly equivalent clinical sensitivity.Acknowledgements
GE Healthcare and NIH R01 EB017739References
1. Koch KM, Brau AC, Chen W, Gold GE, Hargreaves BA, Koff M, McKinnon GC, Potter HG, King KF. Imaging near metal with a MAVRIC-SEMAC hybrid. Magn Reson Med 2011;65(1):71-82.
2. Koch KM, Lorbiecki JE, Hinks RS, King KF. A multispectral three-dimensional acquisition technique for imaging near metal implants. Magn Reson Med 2009;61(2):381-390.
3. Lu W, Pauly KB, Gold GE, Pauly JM, Hargreaves BA. SEMAC: Slice Encoding for Metal Artifact Correction in MRI. Magn Reson Med 2009;62(1):66-76.
4. Hargreaves BA, Chen W, Lu W, Alley MT, Gold GE, Brau AC, Pauly JM, Pauly KB. Accelerated slice encoding for metal artifact correction. J Magn Reson Imaging 2010;31(4):987-996.
5. Levine E, Stevens K, Beaulieu C, Hargreaves B. Accelerated three-dimensional multispectral MRI with robust principal component analysis for separation of on- and off-resonance signals. Magn Reson Med 2018;79(3):1495-1505.
Figures