4589
Single Breath-Hold Diffusion MRI utilizing a Spiral TSE with Variable Flip Angle Refocusing1Center for Magnetic Resonance Research, Department of Radiology, University of Minnesota, Minneapolis, MN, United States
Synopsis
A single breath-hold diffusion MRI sequence utilizing turbo spin echo (TSE) with variable flip angle refocusing and spiral readout is introduced. Flip angles of the refocus RF pulses were determined with the prospective extended phase graph method to minimize the impact of fluctuating refocusing echo signals in TSE. Spiral k-space sampling made the sequence tolerant to motion. The feasibility of the proposed sequence was tested in in vivo brain and thoracic imaging. The proposed single breath-hold diffusion sequence achieved diffusion-weighted imaging of the thoracic region without clear cardiac motion artifacts.
Purpose
Diffusion-weighted imaging (DWI) with echo-planar imaging (EPI) readout is a widely used imaging method in the neuroscience and oncology fields. Single-shot EPI is a fast imaging technique tolerant to motion, but it is well known to be highly sensitive to magnetic susceptibility and off-resonance effects. Therefore, DWI of strong susceptibility tissues such as the thoracic region is very challenging with EPI-based techniques. In this study, we introduce a single breath-hold diffusion MRI sequence utilizing turbo spin echo (TSE) with spiral readout. The TSE acquisition can minimize image distortion and signal loss due to strong susceptibility effects. In addition, repeated sampling around k-space center in spiral sampling makes it tolerant to motion.
Methods
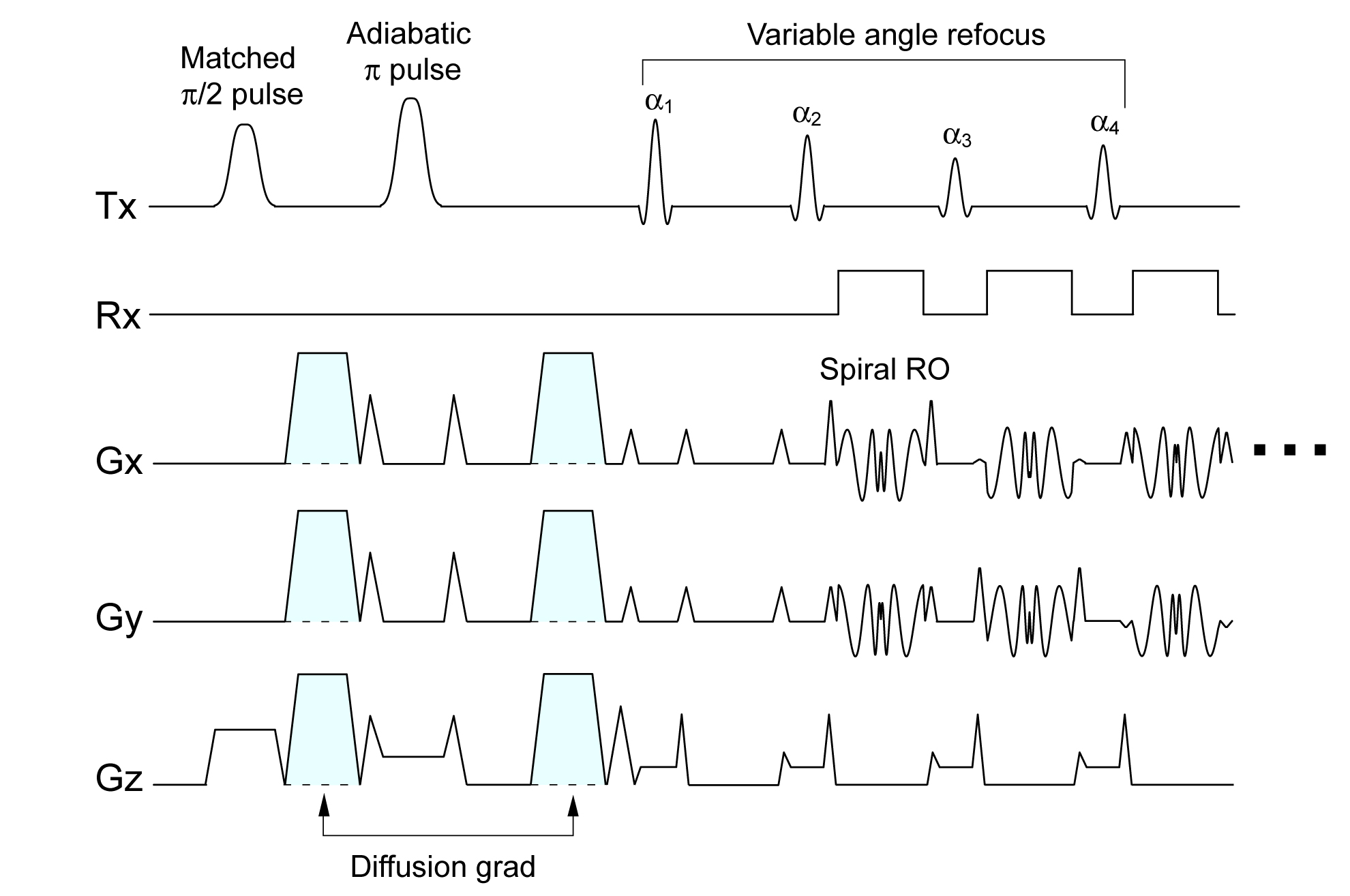
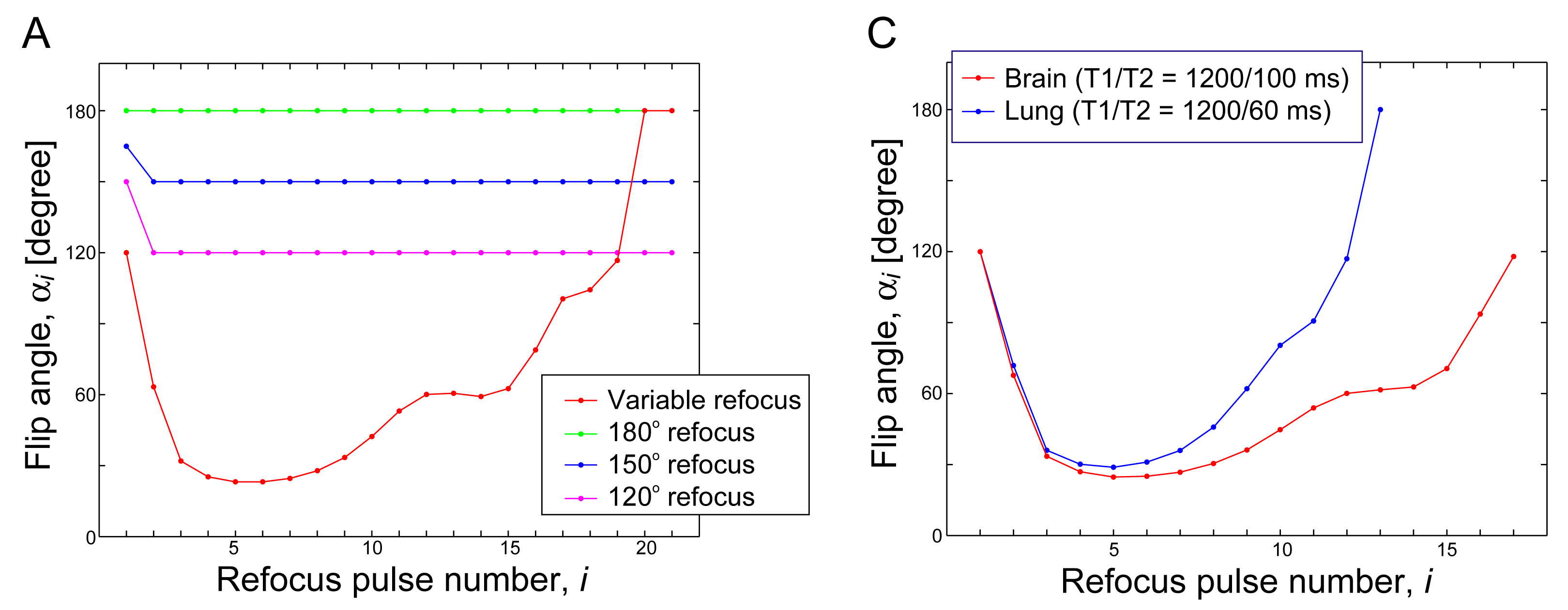
MR imaging in this study was performed with a 3T Siemens Prisma MRI scanner. The proposed spiral diffusion sequence is composed of monopolar diffusion preparation with an adiabatic refocusing pulse and variable flip angle TSE acquisition (Fig.1). With adiabatic refocusing, the probability of producing unwanted spin- and stimulated-echoes is minimized. To eliminate the quadratic phase from the adiabatic refocusing pulse, a matched π/2 pulse was employed for excitation (1). In the TSE acquisition, the SPLICE technique is used to split the CPMG and non-CPMG components in the refocusing echoes, which reduces intensity fluctuations due to motion and eddy current related phase variation in diffusion MRI (2). Each refocusing echo was acquired with a spiral-in and -out k-space trajectory. Because spiral acquisition samples the center of k-space in every readout, fluctuation of the refocusing echo signals results in trajectory-related artifacts (3). To minimize the fluctuation of the refocusing signals, variable flip angle refocusing is used; flip angles of the refocusing pulses were determined with the prospective extended phase graph method (Fig.2) (4). To test the impact from the fluctuating echoes, a phantom measurement was conducted with the variable flip angle refocusing and constant flip angle refocusing. Sequence parameters in the phantom measurement were: TR = 2 sec, TEeff = 182 ms, echo spacing (esp) = 14.3 ms, echo train length (etl) = 20, 1.3 mm in-plane resolution, slice thickness = 5 mm, averages=4 and TA=10 sec. TEeff was given by an average of TEs of the acquired echoes. Each of the 4 average datasets was reconstructed separately and then combined by calculating the root sum of squares.
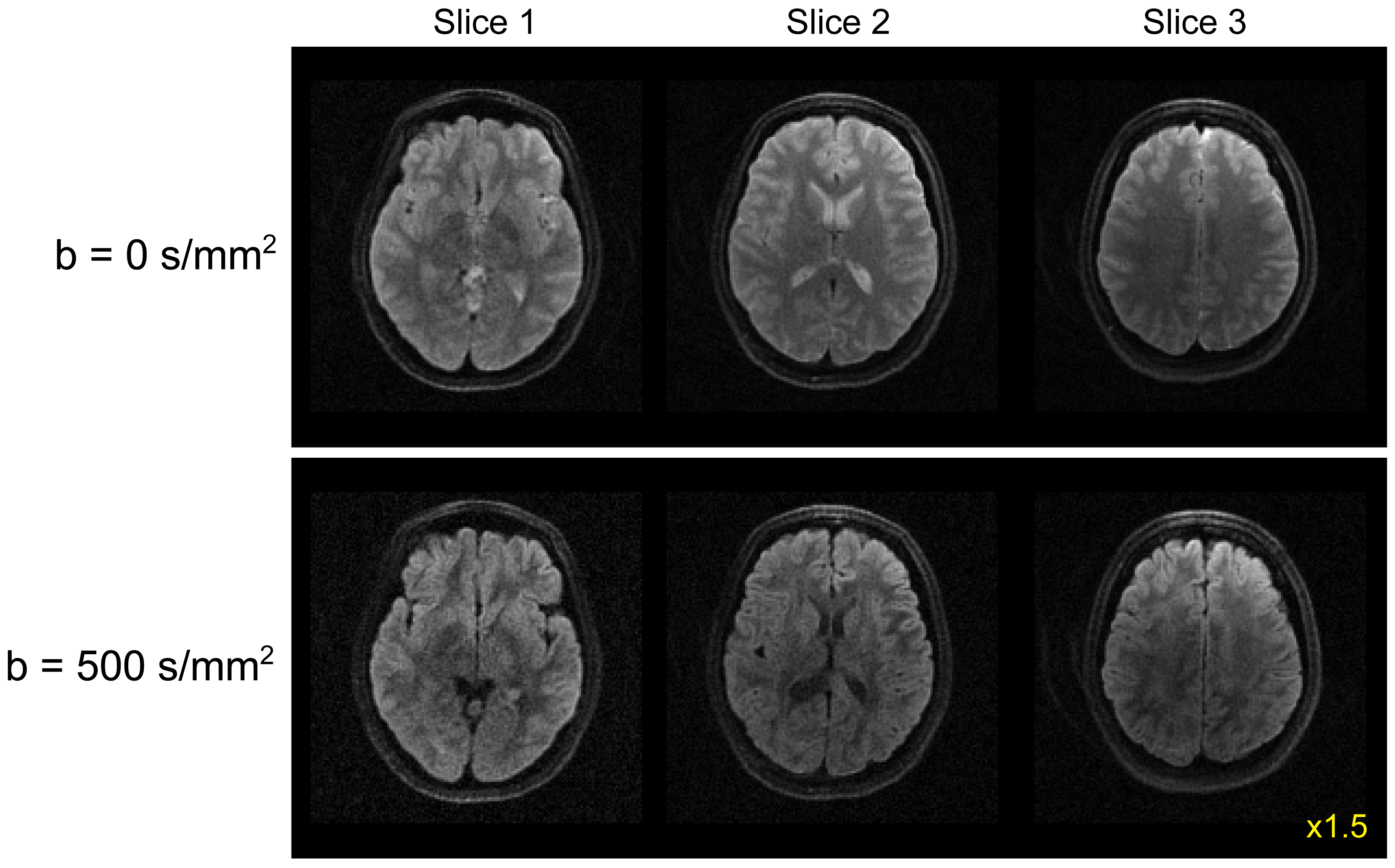
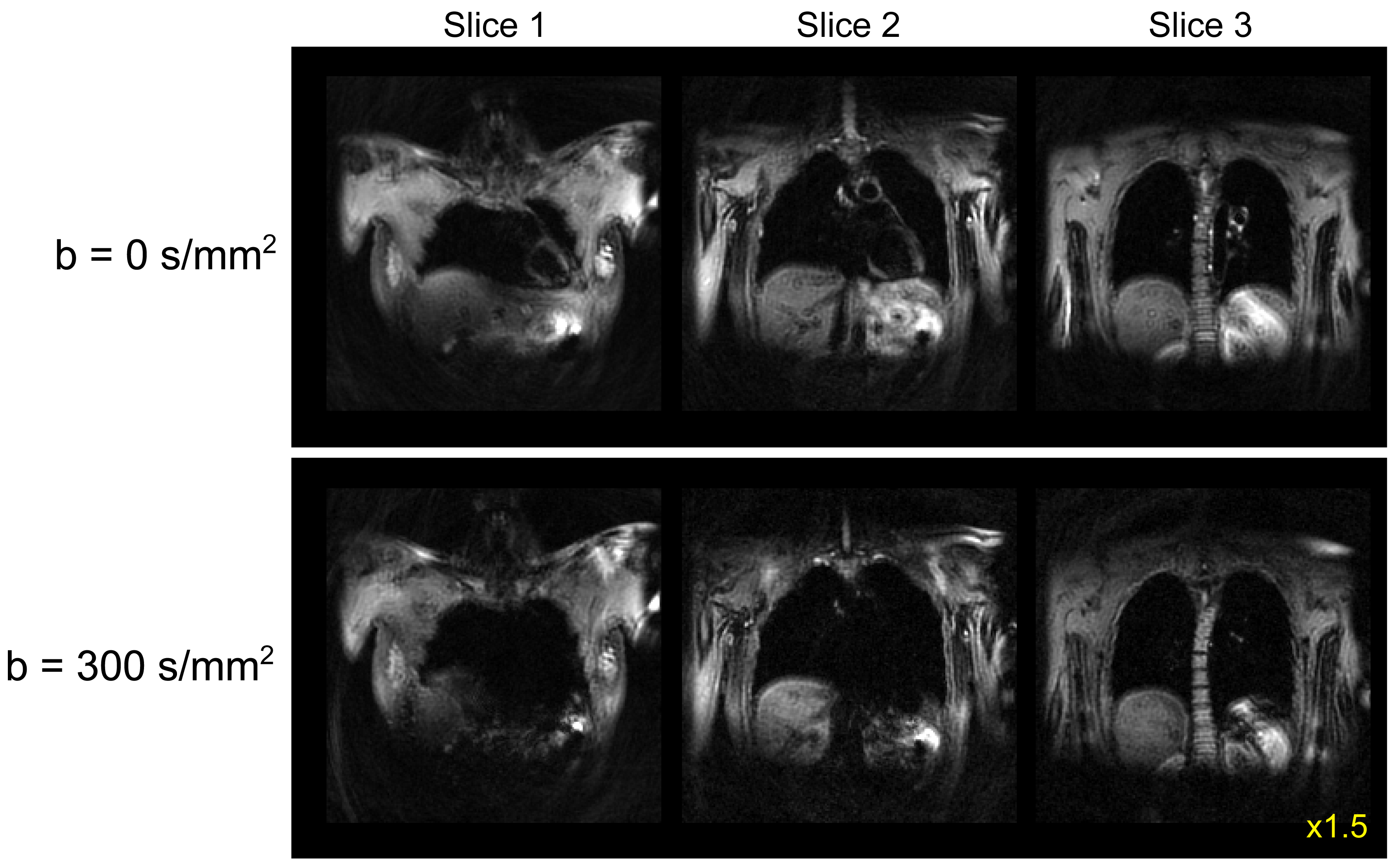
Normal volunteer scans were performed under an IRB approved protocol. In brain imaging, diffusion-weighted images were acquired with b = 0 and 500 s/mm2. Sequence parameters for brain scans were: TR = 2 sec, TEeff = 153 ms, esp = 13.5 ms, etl = 17, 1.3 mm in-plane resolution, slice thickness = 5 mm, averages=4 and TA=18 sec. In thoracic imaging, diffusion-weighted images of b = 0 and 300 s/mm2 were acquired during a single breath holding. Sequence parameters for thoracic imaging were: TR = 2 sec, TEeff = 113 ms, esp = 12.3 ms, etl = 13, 2.9 mm in-plane resolution, slice thickness = 10 mm, averages=4 and TA=18 sec. Image reconstruction in this study was performed offline using an image reconstruction routine written with C++.
Results
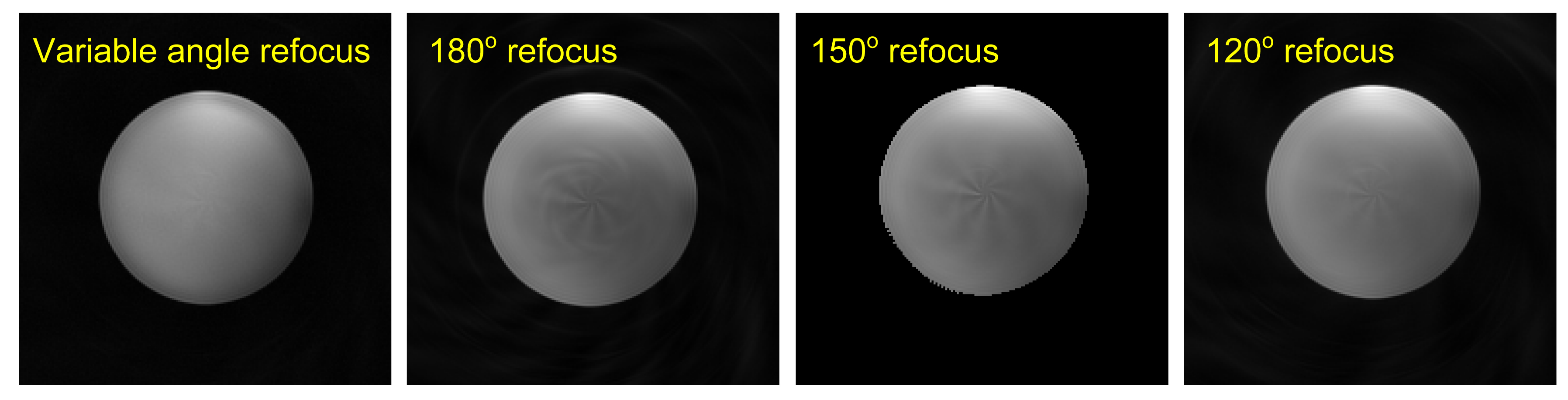
In phantom measurements, variable flip angle refocusing produced a nearly artifact-free image, whereas images from constant flip angle refocusing showed spiral trajectory related artifacts especially with 180° refocusing (Fig.3). In brain imaging, a single 18 sec diffusion scan provided two b-value images (b = 0 and 500 s/mm2) with clear diffusion weighting (Fig.4). In thoracic imaging, there were no clear motion artifacts in the reconstructed images even without cardiac gating (Fig.5).Discussion
The proposed DWI method in this study is technically a single-shot imaging sequence. Therefore, it required relatively long echo train length (i.e. long effective TE) to cover the entire k-space in one TR. Multi-shot acquisition can reduce the effective TE and thus increase SNR. However, it requires correction of the motion-induced phase shot by shot (5), which necessitates additional processing in reconstruction.
The DWI sequence proposed herein should be useful to characterize indeterminate lung nodules. Previous lung cancer MRI studies demonstrated that DWI offers the capability to differentiate benign and malignant lung nodules (6). Clinically relevant lung nodules are typically of a size of 8 mm or greater in diameter. The in-plane resolution achieved in this study (2.9 mm) could be sufficient for assessment of the clinically relevant lung nodules. The accuracy of this technique for characterizing clinically relevant lung nodules needs to be elucidated in future patient studies.
Conclusions
The single breath-hold spiral diffusion TSE with variable flip angle refocusing achieved DWI of the thoracic region without clear cardiac motion artifacts.Acknowledgements
This study was supported by NIH grant P41EB015894 and 1S10OD017974-01.References
1. Balchandani P, Yamada M, Pauly J, Yang P, Spielman D. Self-refocused spatial-spectral pulse for positive contrast imaging of cells labeled with SPIO nanoparticles. Magnetic resonance in medicine. 2009;62(1):183-92.
2. Schick F. SPLICE: sub-second diffusion-sensitive MR imaging using a modified fast spin-echo acquisition mode. Magnetic resonance in medicine. 1997;38(4):638-44.
3. Li Z, Karis JP, Pipe JG. A 2D spiral turbo-spin-echo technique. Magnetic resonance in medicine. 2018;80(5):1989-96.
4. Busse RF, Hariharan H, Vu A, Brittain JH. Fast spin echo sequences with very long echo trains: design of variable refocusing flip angle schedules and generation of clinical T2 contrast. Magnetic resonance in medicine. 2006;55(5):1030-7.
5. Truong TK, Guidon A. High-resolution multishot spiral diffusion tensor imaging with inherent correction of motion-induced phase errors. Magnetic resonance in medicine. 2014;71(2):790-6.
6. Henzler T, Schmid-Bindert G, Schoenberg SO, Fink C. Diffusion and perfusion MRI of the lung and mediastinum. European journal of radiology. 2010;76(3):329-36.
Figures