4566
Dual Contrast Weighting and Simultaneous T2 and T2* Mapping with Radially Sampled RARE-EPI1Berlin Ultrahigh Field Facility (B.U.F.F.), Max Delbrueck Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany
Synopsis
MRI examinations commonly involve a series of multiple imaging contrasts and MR-metrics. Dual or even more contrast techniques offer substantial scan time reduction and eliminate the propensity to slice co-registration errors induced by bulk and physiological motion. Recognizing this opportunity this work presents a dual contrast RARE-EPI hybrid, that provides T2 (RARE module) and T2* (EPI module) contrast and facilitates simultaneous T2 and T2* mapping in a single radially (under)sampled scan (2-in-1 RARE-EPI). The applicability of 2-in-1 RARE-EPI is demonstrated in phantom and in in vivo studies and benchmarked versus conventional T2 and T2* weighted/mapping techniques.
Introduction:
For reasons of speed and clinical utility it is conceptually appealing to pursue MRI techniques that are sensitive to multiple contrast mechanisms and support simultaneous generation of two or more contrasts [1]. Generating two or even more contrasts simultaneously within one acquisition, offers substantial reduction of measurement time. This is of benefit in a clinical scenario, but also in preclinical studies where multiple parameters are assessed using imaging protocols with tight spatio-temporal resolution constraints. Moreover, simultaneous acquisition of multiple contrasts obviates the need for slice co-registration when combining multiple series of images with different contrast, which would be advantageous for applications dealing with bulk or physiological motion such as cardiac or ophthalmic MRI. Realizing this opportunity this abstract proposes a dual contrast RARE-EPI hybrid [2], that provides T2 (RARE module) and T2* (EPI module) contrast and facilitates simultaneous T2 and T2* mapping in a single radially (under)sampled scan, which will be referred to 2-in-1 RARE-EPI for reasons of brevity. The applicability of 2-in-1 RARE-EPI is carefully examined in phantom and in in vivo studies and benchmarked versus conventional T2 and T2* weighted/mapping techniques.Methods:
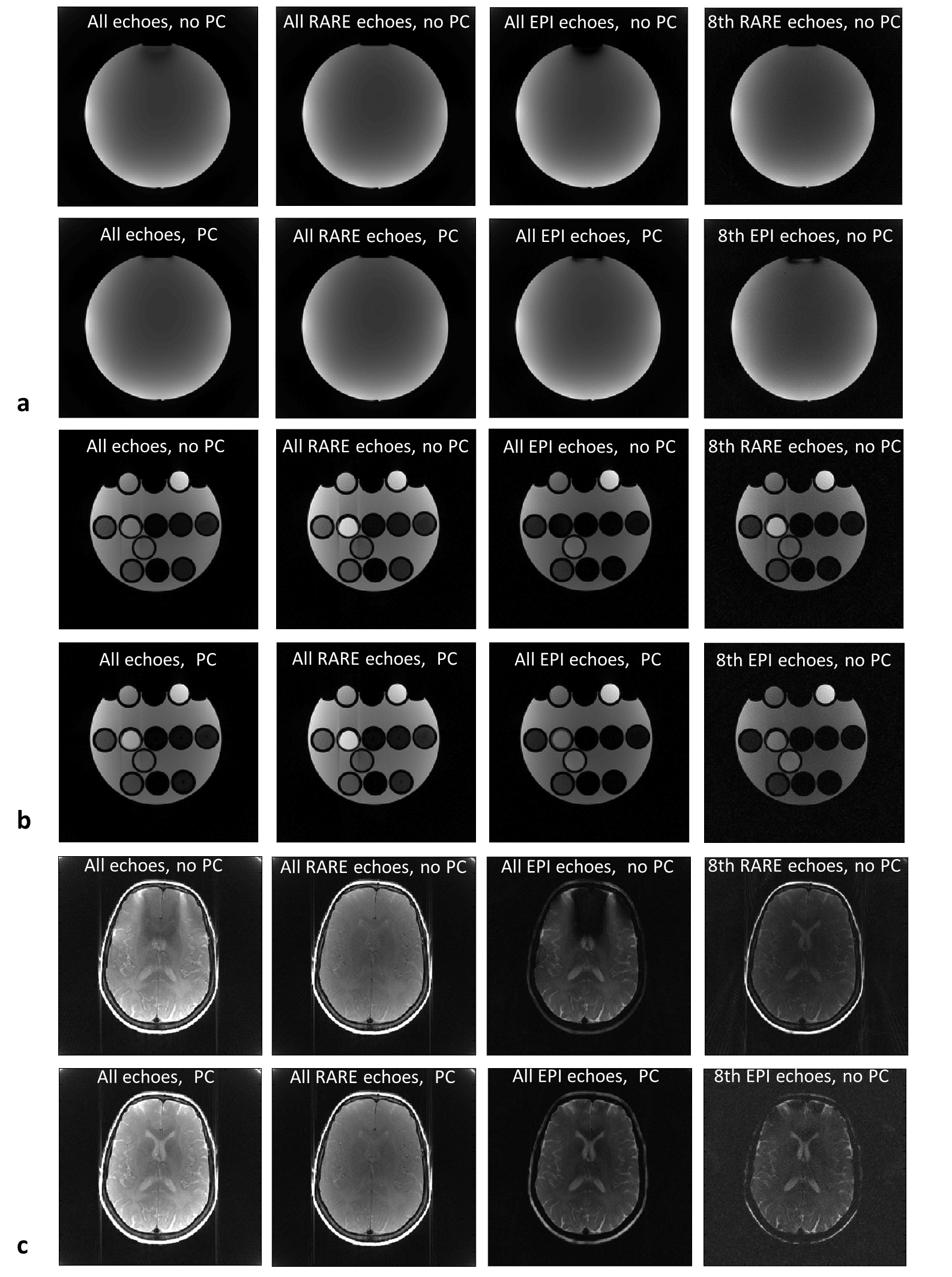
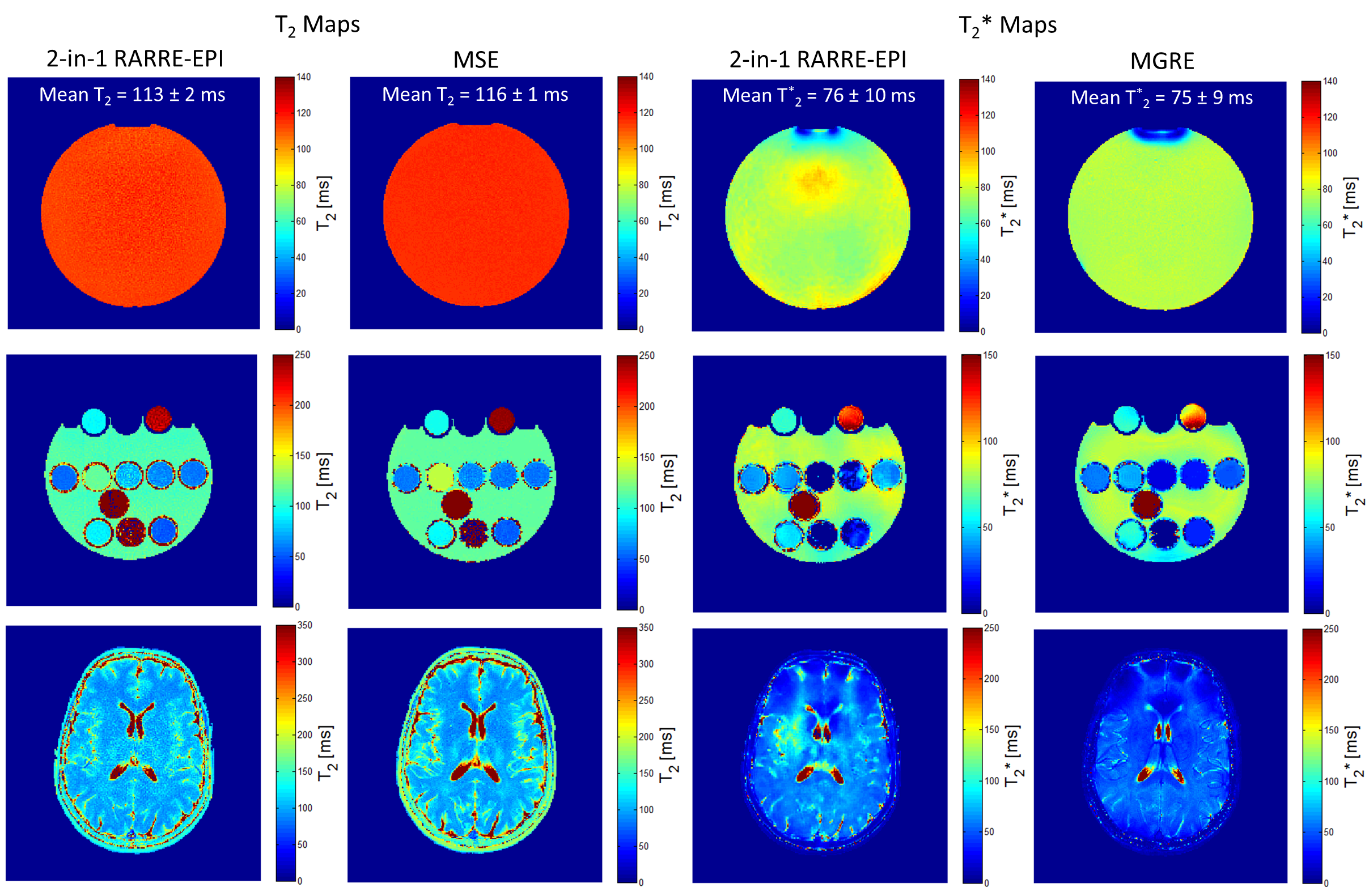
In the RARE-EPI hybrid [3] the first echoes in the echotrain are acquired with a RARE module whereas the later echoes are acquired with an EPI module (Figure 1, left). The combined-acquisition-technique (CAT) factor λ (λ=0.5 in this work) determines the fraction of RARE echoes in the echotrain. In this work, RARE and EPI echoes are acquired in an interleaved manner with respect to the angular position in radially sampled k-space (Figure 1, right). For the view ordering of the RARE echoes we used the bit-reverse scheme [4] to reduce T2-decay induced streaking artefacts, but without distributing echoes in one TR over the full angular range. For the EPI module sequential view ordering was applied to ensure short echo spacing. The method proposed by Block et al. [5] was used to correct for gradient delay artefacts. Images from radial k-space data were reconstructed using regridding with linear density compensation and a magnitude sum-of-squares channel combination. To reconstruct images including all EPI echoes a phase correction (PC) [6] was used, since magnetic field inhomogeneities lead to phase inconsistencies between EPI spokes. Reference T2 and T2* maps were acquired with conventional multi-spin-echo (MSE) and multi-gradient-echo (MGRE) techniques (see caption of Figure 2 for sequence parameters). T2 and T2* maps were calculated with a linear least-square-fit of the logarithmic signal magnitude. For T2* mapping a spatial-adaptive-non-local-means filter was applied to the images prior to the fitting to improve the fit quality [7]. Images were acquired at 3.0T (Siemens Magnetom Verio, Erlangen, Germany) using a 32-channel receive-only head coil (Siemens, Erlangen, Germany). Two phantoms were used: A spherical homogeneous phantom (diameter=15cm), filled with Dimethylpolysiloxan-oil (T2=106ms and T1=452ms), and cylindrical agarose tube phantom (outer diameter=12.5cm, tube diameter=1cm). In vivo images of the brain were acquired from a healthy subject.Results:
Figure 2 shows MR images of the two phantoms and the brain of a healthy subject acquired with 2-in-1 RARE-EPI. The images reconstructed from all echoes, from RARE echoes only (T2 weighted) and from EPI echoes (T2* weighted) exhibit different contrasts. The phase correction (PC) [6] reduces the signal voids which occur if all EPI echoes are combined for image reconstruction. Figure 3 demonstrates, that the T2 map (RARE module, mean T2=113±2ms) of the uniform Dimethylpolysiloxan-oil phantom accords with the reference T2 map (mean T2=116±1ms). The T2* map (mean T2*=76±10ms) obtained from the EPI module is in good agreement with the MGRE reference (mean T2*=75±9ms). The T2 and T2* maps obtained for the tube phantom and for the brain demonstrate agreement between the data derived from 2-in-1 RARE-EPI and MSE and MGRE reference scans (Figure 3). The T2 and T2* maps obtained for the tube phantom and for the brain demonstrate agreement between the data derived from the 2-in-1 RARE-EPI and he MSE and MGRE reference scans (Figure 3).Discussion and Conclusions:
This work demonstrates the feasibility of radially sampled 2-in-1 RARE-EPI which facilities recording of dual contrast weighted images (T2 and T2*) and simultaneous acquisition of T2 and T2* maps. The proposed 2-in-1 RARE-EPI hybrid technique decreases acquisition time for T2 and T2* mapping. To conclude, the proposed 2-in-1 RARE-EPI hybrid is not limited to brain imaging, shown in this work. Dual contrast RARE-EPI also holds the promise to meet the needs of applications dealing with bulk or physiological motion such as cardiac imaging including T2 imaging/mapping of myocardial edema and myocardial T2* mapping [8], as well as MRI of the eye, abdomen and liver.Acknowledgements
The authors would like to thank Antje Els for providing assistance with the in vivo measurements.References
1. K. Fuchs et al., Magn Reson Med, 72(6): p. 1590, 2014
2. C. Hillenbrand et al., MAGMA, 10(3): p. 183, 2000
3. K. Paul et al., NMR Biomed, 31(3): p. e3872, 2018
4. R.J. Theilmann et al., Magn Reson Med, 51(4): p. 768, 2004
5. K.T. Block et al., Proc Int Soc Magn Reson Med Sci Meet Exhib 19, 2816, 2011
6. H. Bhat et al., Magn Reson Med, 66(1): p. 82, 2011
7. J.V. Manjón et al., J Magn Reson Imaging, 31(1): p. 192, 2010
8. T. Huelnhagen et al., Front Phys, 5: p. 22, 2017
Figures