4514
MRI quality data assessment in the Italian IRCCS advanced neuroimaging network using ACR phantoms1Neuroradiology Unit, Brain MRI 3T Research Center, IRCCS Mondino Foundation, Pavia, Italy, 2Neuroradiology, Fondazione I.R.C.C.S. Istituto Neurologico Carlo Besta, Milan, Italy, 3IRCCS Fondazione Don Carlo Gnocchi, Milano, Italy, 4IRCCS Fondazione Stella Maris, Pisa, Italy, 5Queen Square MS Centre, Department of Neuroinflammation, UCL Queen Square Institute of Neurology, Faculty of Brain Sciences, University College London, London, United Kingdom, 6Department of Brain and Behavioural Sciences, University of Pavia, Pavia, Italy, 7Brain MRI 3T Research Center, IRCCS Mondino Foundation, Pavia, Italy, 8The Italian IRCCS advanced neuroimaging network, Milan, Italy
Synopsis
Generating big-data is becoming imperative with the advent of machine learning. Neuroimaging networks respond to this need. Italian Research Neurological Institutes have formed an advanced neuroimaging network to develop protocols for multisite studies. The present work reports on ACR phantom data across sites and evaluates accuracy and longitudinal reproducibility of: uniformity and ghosting, geometric accuracy, slice thickness, high-contrast and low-contrast object detectability. Our findings show that uniformity, geometric accuracy, low-contrast object detectability are measures that failed at some sites. We intervened to correct these issues improving protocol quality and scanner stability, establishing levels of precision relevant for future multicentre studies in quantitative imaging.
Introduction
Big data is the new frontier of innovation. The need of analyzing large amount of data is becoming fundamental in many fields to improve efficiency, quality and prediction of results. An important example is the healthcare domain. Indeed, in the last years, several neuroimaging networks comprising numerous centers all over the world have been formed to collect, put together and share big amount of data (1,2). In this context, the Italian IRCCS advanced neuroimaging network* was born with the support of the Italian Ministry of Health (RRC-2016-2361095; RRC-2017-2364915) to share common MRI protocols and evaluate the performances of each MRI scanner that is part of the network for future multisite and multivendor studies. The network is composed of twenty-two sites distributed all around Italy. Each one has been involved in multiple tasks, ranging from technical to clinical skills. The aims of this work were: 1) to implement and optimize the standardized American College of Radiology (ACR) protocol (3); 2) to evaluate the accuracy and reproducibility of different geometrical and contrast measures using ACR phantoms across sites and vendors; 3) to evaluate the longitudinal reproducibility of these phantom measures.Methods
Phantom: After a benchmarking of different available phantoms, two were selected: ACR large and ACR small, selected according to the dimension of the head-coil used at each site.
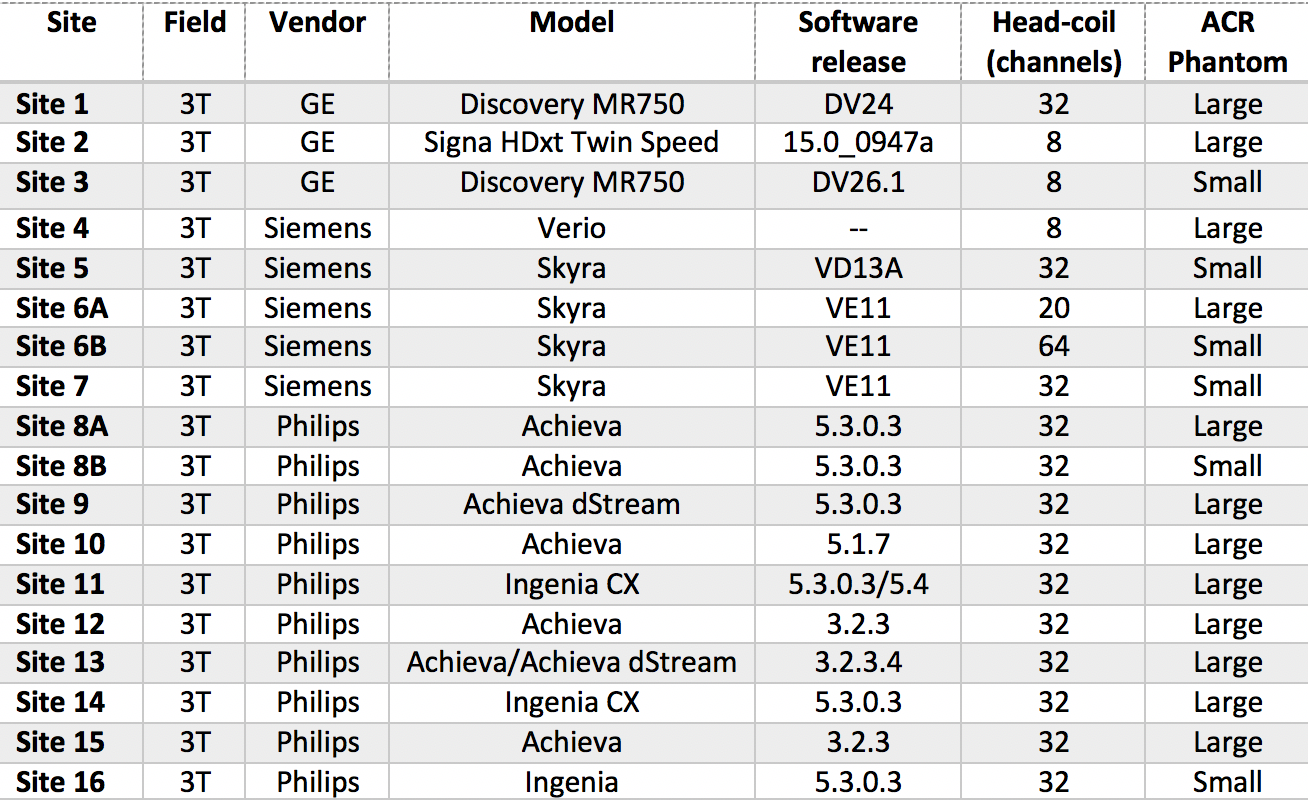
IRCCS sites: Sixteen of the twenty-two sites have a 3T scanner; for the longitudinal analysis, fourteen sites that acquired at least 4 time points were included. The scanner vendors included General Electric, Philips, and Siemens. Details of the scanner and head-coil used at each site are reported in Table1.
Acquisition protocol: Starting from the standardized ACR protocol (3) that includes T1w/T2w images, sequence parameters were adapted as follow: acquisition matrix was modified to obtain an in-plane isotropic voxel (ACR small), post-processing filters were disabled and receiving bandwidth was set at 250±20Hz/px. The protocol was implemented at three sites, one for each vendor, and distributed to the remaining centers.
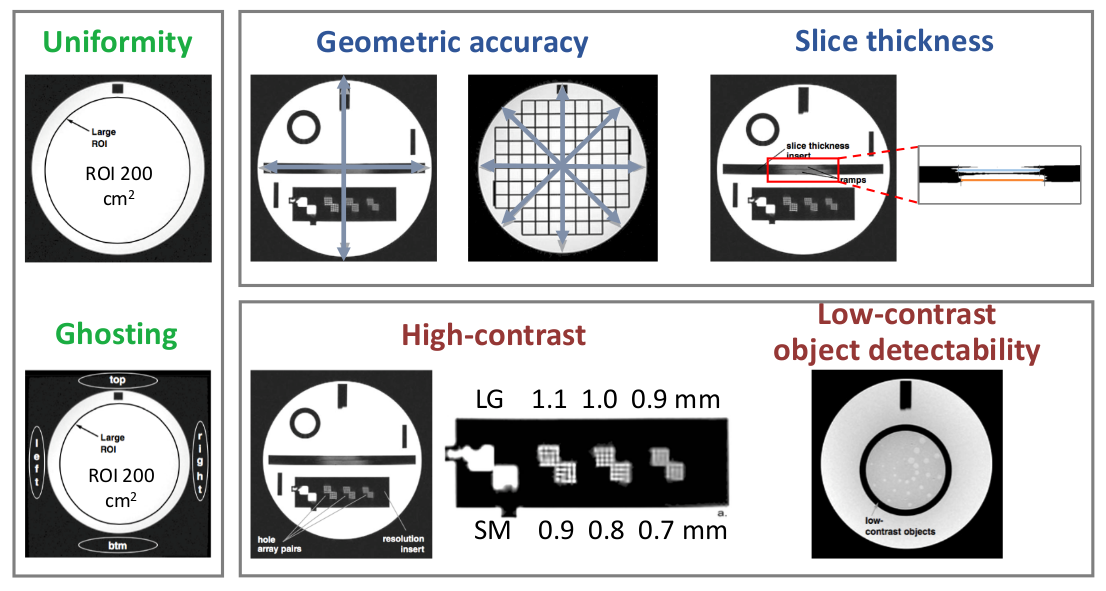
ACR analysis: Two different software were tested for data analyses: a commercial software, Radia (https://radimage.com/products/rit-family-of-products/diagnostic), and a semi-automatic quality assurance (SAQA) Matlab script (http://jidisun.wixsite.com/osaqa-project/resources). The following tests were performed and standard ACR tolerance range was considered: analysis of uniformity and ghosting, geometric accuracy, slice thickness, high-contrast and low-contrast object detectability (Fig1).
Scanners were considered longitudinally not stable if the same test failed at least at two consecutive time points.
Results
Our findings showed that the SAQA script is more flexible (it can be easily modified) and less user-dependent than Radia, thus all analyses were performed using the SAQA script.
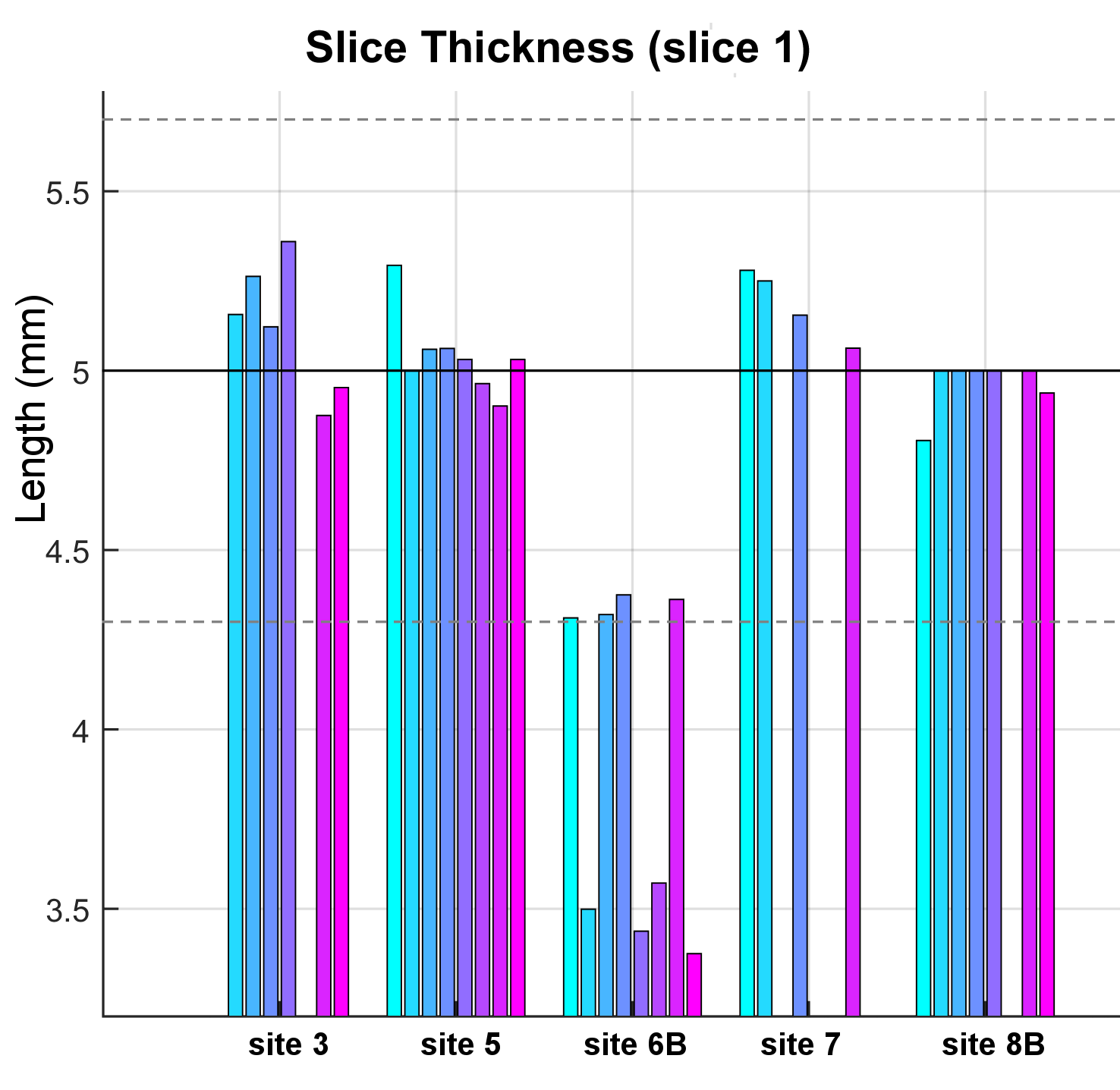
ACR small: all sites passed all tests except site 6B that failed, longitudinally, the slice thickness measure (Fig2).
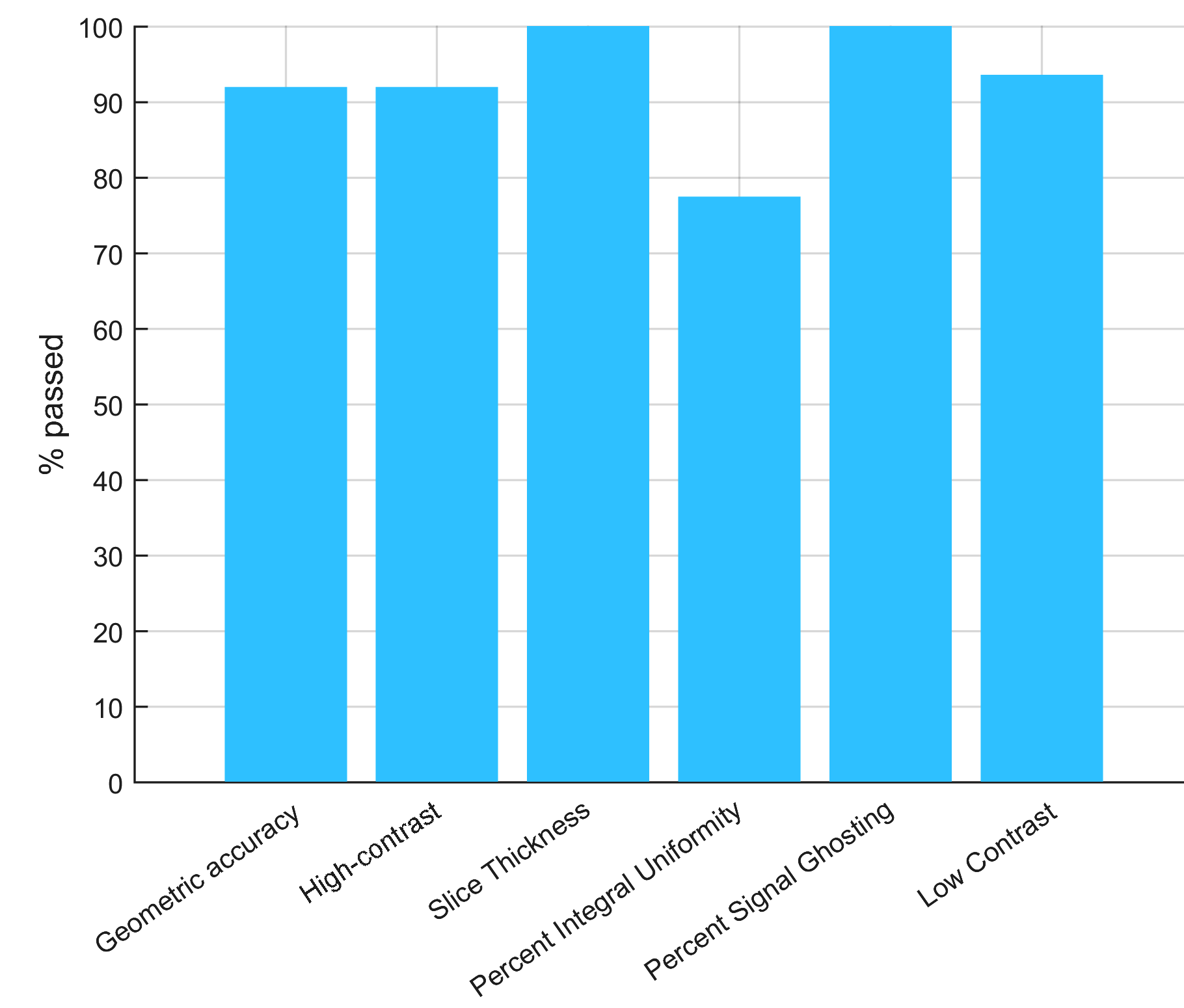
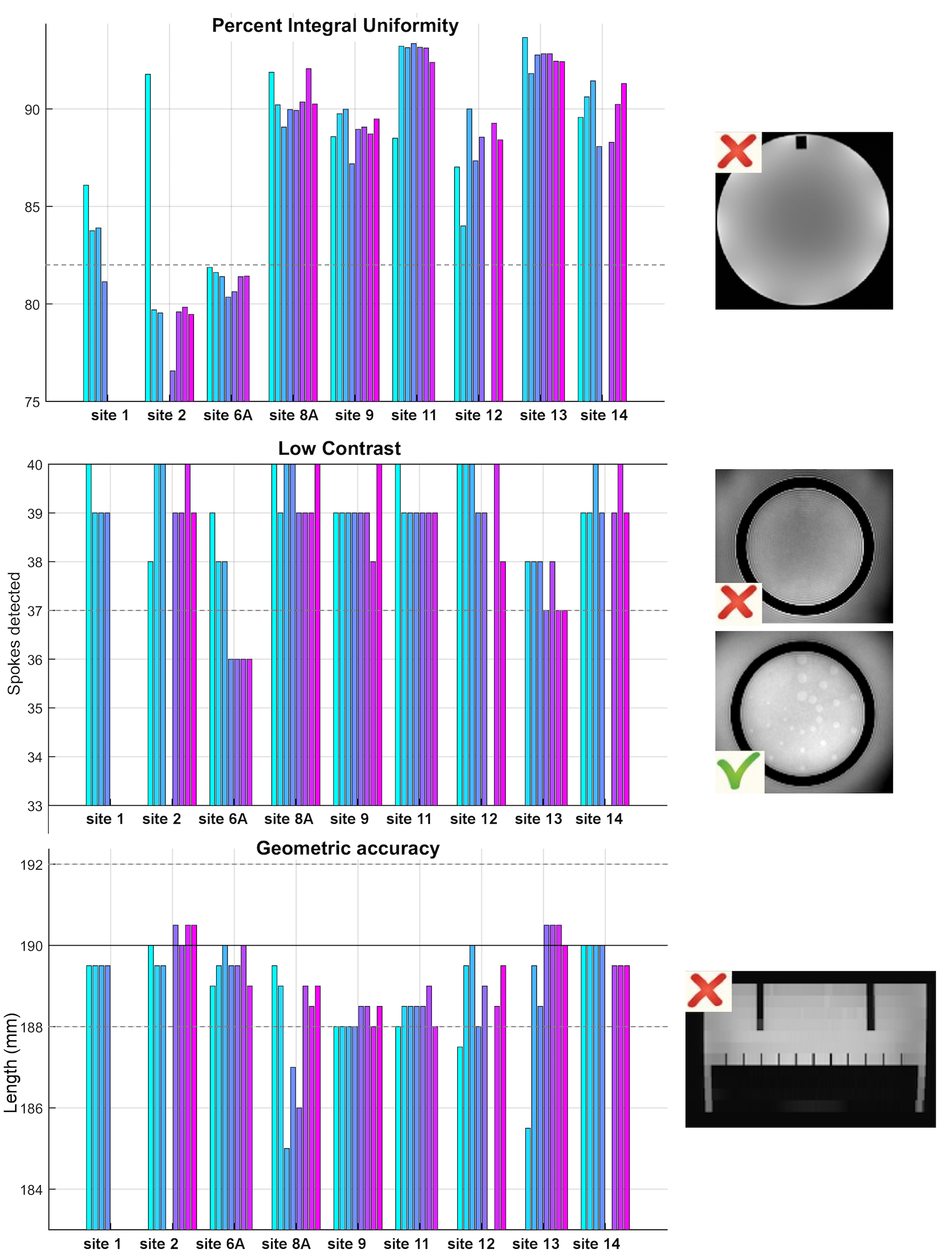
ACR large: all sites passed the ghosting and slice thickness tests, while for the other tests at least one site highlighted some problems in one or more time points (Fig3). In detail, two sites (2 and 6A) failed the uniformity test and one site (6A) failed the low-contrast object detectability test in at least two consecutive time points. Furthermore, two sites (8A in 3 time-points, and 13 in 1 time-point) failed the geometric accuracy test (Fig4).
Discussion
The Italian IRCCS neuroimaging network is the first large neuroimaging network in Italy and the present work demonstrates how good synergy between sites can improve scientific impact of each involved center.
The network is composed of many vendors, different software releases and, in some cases, different types of coils. All these variables affect the sequences output and consequently the harmonization pipeline. This exercise also allowed us to enhance the original ACR scanning procedure by limiting additional software and hardware confounding factors that could affect quantitative imaging (3).
For example, our tests showed that the slice thickness measure seemed to be affected by the number of coil channels and suggested a possible intervention to tune their gains. Furthermore, the geometric accuracy test highlighted a significant deformation along the cranio-caudal direction in certain sites, suggesting the necessity to tune the scanner gradients. Moreover, geometric accuracy and low contrast tests gave indications about possible B0 inhomogeneities (e.g. imperfect shim or a gradient miscalibration) and a low SNR (4).
In conclusion, setting up this procedures with the ACR phantoms have identified sites performing below acceptable image quality levels. Thanks to the technical expertise available at network level, each site was supported to correct their specific issues, improving the quality of own protocols and understanding the importance of checking scanner stability over time, essential for quantitative in vivo neurological studies.
Acknowledgements
This study was funding by the Italian Minister of Health (RRC-2016-2361095; RRC-2017-2364915).
* The Italian IRCCS advanced neuroimaging network is constituted by the following centers: IRCCS Istituto Auxologico Italiano (Milan); IRCCS Ospedale pediatrico Bambino Gesù (Rome); Fondazione IRCCS Istituto neurologico “Carlo Besta” (Milan); IRCCS Centro Neurolesi “Bonino Pulejo” (Messina); Centro IRCCS “Santa Maria nascente” - Don Gnocchi (Milan); IRCCS Centro San Giovanni di Dio – Fatebenefratelli (Brescia); IRCCS Ospedale pediatrico “Giannina Gaslini” (Genoa); IRCCS Istituto Clinico Humanitas (Milan); Istituto di Ricerche Farmacologiche “Mario Negri” IRCCS (Milan); Istituti Clinici Scientifici Maugeri, IRCCS (Pavia); IRCCS Eugenio Medea (Bosisio Parini); Fondazione IRCCS Istituto Neurologico “Casimiro Mondino” (Pavia); IRCCS NEUROMED – Istituto Neurologico Mediterraneo (Pozzilli); IRCCS Associazione Oasi Maria SS Onlus – Troina (Enna); Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (Milan); IRCCS Fondazione Ospedale San Camillo (Venice); IRCCS Ospedale San Raffaele (Milan); IRCCS Fondazione Santa Lucia (Rome); IRCCS Istituto di Scienze Neurologiche (Bologna); IRCCS SDN Istituto di ricerca diagnostica e nucleare (Naples); IRCCS Fondazione Stella Maris (Pisa)
References
- Jack CR Jr, Barnes J, Bernstein MA, et al. Magnetic resonance imaging in Alzheimer's Disease Neuroimaging Initiative 2. Alzheimers Dement. 2015 Jul;11(7):740-56.
- UK Biobank data on 500,000 people paves way to precision medicine. Nature. 2018 Oct;562(7726):163-164.
- Phantom Test Guidance for Use of the Large MRI Phantom for the ACR Large. https://www.acraccreditation.org/-/media/ACRAccreditation/Documents/MRI/LargePhantomGuidance.pdf?la=en
- Mulkern RV, Forbes P, Dewey K, et al. Establishment and results of a magnetic resonance quality assurance program for the pediatric brain tumor consortium. Acad Radiol. 2008 Sep;15(9):1099-110.
Figures