4499
Correcting breast MRI with a generic B-1(+) template for T-1 map calculation1Center for Image Sciences, UMC Utrecht, Utrecht, Netherlands, 2Biomedical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
In 7T breast MRI, the use of local transmit coils causes an inhomogeneous B1+ field, decaying towards the pectoral muscle. This leads to differences in image contrast throughout the breasts and in dynamic contrast enhanced (DCE) MR images it has a direct influence on the enhancement kinetic curves. Therefore a correction is necessary. We used B1+ simulations to generate a template to correct the images, because the dynamic range of measured B1+ maps is often insufficient. We validated the template on eleven volunteers. T1-maps were calculated using the generic template as a first step of correcting the DCE images.
Introduction
The use of a higher field strength (7T) for dynamic contrast enhanced MRI (DCE-MRI) images leads to an increased signal-to-noise ratio, as well as higher spatial and temporal resolution compared to lower field strengths.1 However, the radiofrequency transmit (B1+) field is often inhomogeneous at 7T due to the reduced wave length of the radiofrequency field and the use of local transmit loops causing in breast MRI a decrease in B1+ towards the pectoral muscle.2 Correcting DCE-MRI is necessary since inhomogeneous B1+ directly influences the shape of enhancement curves. The acquired B1+ maps are not sufficient for a proper correction as the dynamic range in B1+ is often beyond the limits for accurate B1+ mapping protocols.3 Van Rijssel et al. showed that it is possible to use a generic B1+ map to correct images acquired with a unilateral breast coil.2 In this study, we investigated the same technique could be applied for bilateral breast imaging. As a first step in DCE correction, B1+ corrected T1-maps were calculated using a variable flip angle (VFA) series.Methods
Ten healthy subjects for template generation and one control subject, to validate the template, of different ages (mean 30, range 21-80 year) and with different sizes of breasts were scanned on a 7T MRI scanner (Philips, Best, The Netherlands) in prone position using a dual-quadrature double-tuned radiofrequency coil.3 Finite-difference time-domain simulations were performed in Sim4Life (ZMT, Zurich, Switzerland) using personalized breast models for each volunteer based on Ella.4 During simulation, a fixed phase was used to generate the individual B1+ simulations and SAR models.3 To generate a generic B1+ template, the individual simulations were normalized before their weighted average was taken. Simulated B1+ distributions were scaled to real-world values using a linear scale factor. This factor was determined for every subject using the average measured B1+ (AFI, TE=1.981 ms, TR=[40,200] ms, FA=30$$$^\circ$$$) and scaled template values in a manually selected region by minimizing the squared error between them.5-7 The root mean squared error (RMSE) was calculated afterwards to quantify the remaining differences between the scaled template and the measured B1+ map. After generating the template, we were able to test this on patient data from an ongoing study. To calculate T1-maps, the DESPOT1 method was used, extended to include the generic B1+ template for 18 patients, using a VFA series (FFE, TE/TR=2/4 ms, FA=[4,10,13]$$$^\circ$$$).8 The individual linear scale factor could be determined using a modified DESPOT1 approach to fit B1+ to the VFA data, assuming a literature-based longitudinal relaxation time for glandular tissue (1.61s) and the least-squares minimization procedure described above.2,8,9 The mean of the longitudinal relaxation time of the glandular tissue was calculated in the area where the scale factor was determined.Results
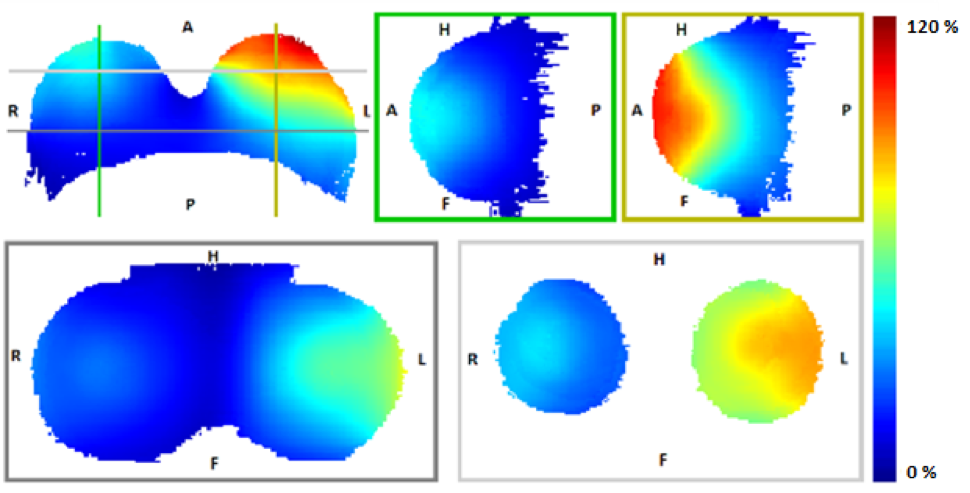
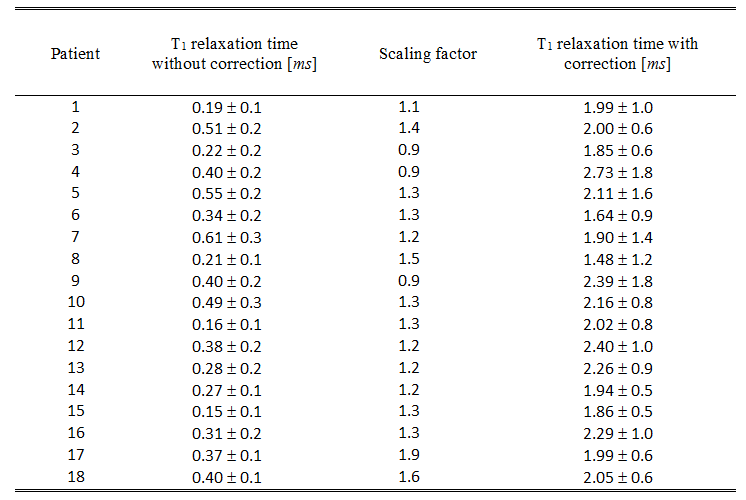
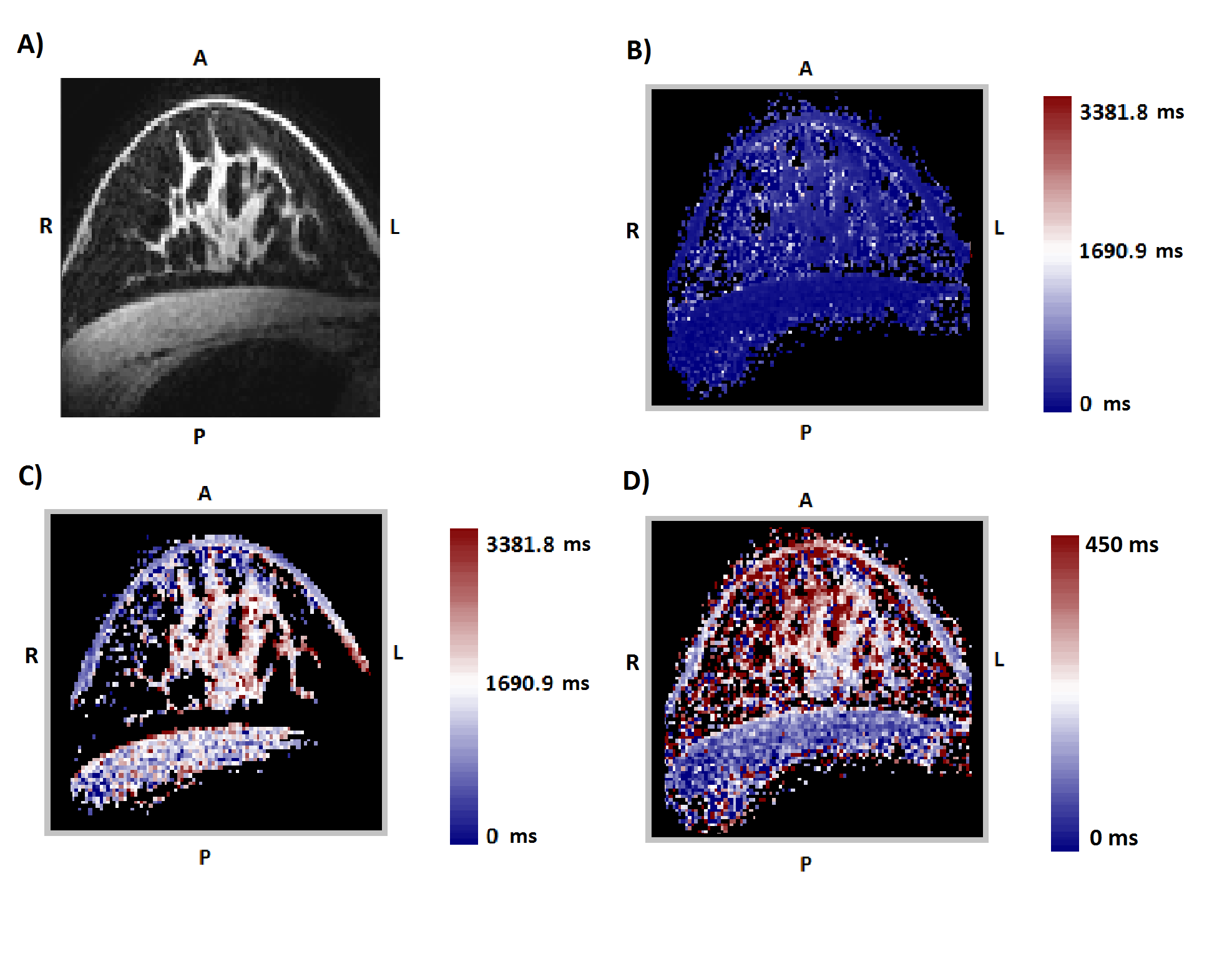
Figure 1 shows the generic B1+ template generated from the individual simulation of ten subjects. The RMSE of the control subject and the ten volunteers was and 4.08% of normal angle respectively, which is in the range of the reproducibility of consecutive B1+ mapping.2 Figure 2 lists the T1 relaxation times of the 18 patients with and without correction. The corrected T1 values are in the same range as values reported in literature.8,9 Figure 3 shows an example of a VFA scan, T1-map without correction, and T1-map with correction of patient number 14. The corrected T1-map (Fig 2C) no longer shows the B1+-induced bias gradient present in the uncorrected T1-map (Fig 2D).Discussion
The good agreement between template and measurement B1+ indicates that this method is feasible for bilateral breast imaging. The calculated mean value of T1 is not identical to the chosen value of 1.61 s, because the calculated B1+ field from the VFA scans is not used directly in the calculation of T1-maps, it is only used to determine the scale factor of the B1+ template.Conclusion
This study presents evidence that individually scaled, generic B1+ templates can be used in a clinical setting to calculate T1 maps and ultimately correct DCE-MRI in the breast at 7T. The correction results in average T1 relaxation times in the range of literature values and compensates for B1+ induced gradient bias.Acknowledgements
We thank the Dutch Cancer Society (Alpe d’Huzes project nr: UU 2013-6302), ZonMw (grant number: 104003019), and the NWO (VENI grant: J.P.Wijnen 016.148.002) for financial support.
References
1. Menezes GLG, Stehouwer BL. Et al. Dynamic contrast-enhanced breast MRI at 7T and 3T: an intra-individual comparison study. Springerplus. 2016;5(1):1-12.
2. van Rijssel MJ, et al. Estimating B1+ in the breast at 7T using a generic template. NMR in Biomedicine. 2018;31(5):1-12.
3. Van der Velden TA, Italiaander M, et al. Radiofrequency Configuration to Facilitate Bilateral Breast 31P MR Spectroscopic Imaging and High-Resolution MRI at 7 Tesla. Magnetic Resonance in Medicine. 2015;74(6):1803-1810.
4. Christ A, Kainz W, Hahn EG, et al. The Virtual Family—development of surface‐based anatomical models of two adults and two children for dosimetric simulations. Phys Med Biol. 2010;55(2):N23‐N38.
5. Yarnykh VL. Actual flip-angle imaging in the pulsed steady state: A method for rapid three-dimensional mapping of the transmitted radiofrequency field. Magnetic Resonance Medicine. 2006;57(1):192-200.
6. Coleman T.F., Y. Li. An Interior. Trust Region Approach for Nonlinear Minimization Subject to Bounds. SIAM Journal on Optimization. 1996;6:418-445.
7. Coleman, T.F., Y. Li. On the Convergence of Reflective Newton Methods for Large-Scale Nonlinear Minimization Subject to Bounds. Mathematical Programming. 1994;67(2):189-224.
8. Haacke E. et al. New Algorithm for Quantifying Vascular Changes in Dynamic Contrast-Enhanced MRI Independent of Absolute T1 Values. Magnetic Resonance in Medicine. 2007;58:463-472.
9. Brown K. et al. Sub-Milimeter Breast Imaging and Relaxivity Characterization at 7T. Proc. Intl. Soc. Mag. Reson. Med. 2011;19:3092.
Figures