4497
Self-Gated Pulmonary Embolism Imaging with Multi-Slice Golden-Angle Radial bSSFP1Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden, 2Department of Clinical Physiology, Karolinska University Hospital, Stockholm, Sweden, 3Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden, 4Department of Radiology, Karolinska University Hospital, Stockholm, Sweden, 5Department of Thoracic Radiology, Karolinska University Hospital, Stockholm, Sweden
Synopsis
Free-breathing, non-contrast bSSFP MRI has shown great potential for imaging of pulmonary embolisms in patients with contraindication for contrast-enhanced computed tomography angiography. While the free-breathing approach is convenient, it limits the possibility for multiplanar reformatting which otherwise could aid in visualizing the pulmonary vasculature. In this work, we propose a methodology for deriving a motion signal from the free-breathing data and we incorporate this signal in the reconstruction pipeline to obtain a slice-aligned image stack from which multiplanar reformatting can be performed.
Purpose
Recently, a new methodology has been proposed for imaging pulmonary embolism with MRI (1,2). Instead of using contrast-enhanced computed tomography angiography (CTA), which comes with the risks associated with exposure to ionizing radiation and the risk of adverse reaction to iodinated contrast agents, the proposed methodology relies on non-contrast enhanced, free breathing, balanced steady state free precession MR imaging with a golden-angle radial trajectory (2). Radial spokes are continuously acquired in each slice position over a few seconds, to capture different phases of the cardiac- and respiratory cycle. This enables good visualization of the pulmonary vasculature on a slice-by-slice basis from sliding window reconstructions. However, the difference in respiratory position between slices may complicate the visual tracking of vessels and may preclude multiplanar reformatting (MPR). The purpose of this study was to develop and evaluate whether using the self-gating capability of the golden-angle trajectory to divide images into motion states would enable motion synchronized slice stacks and MPR reconstructions.Method
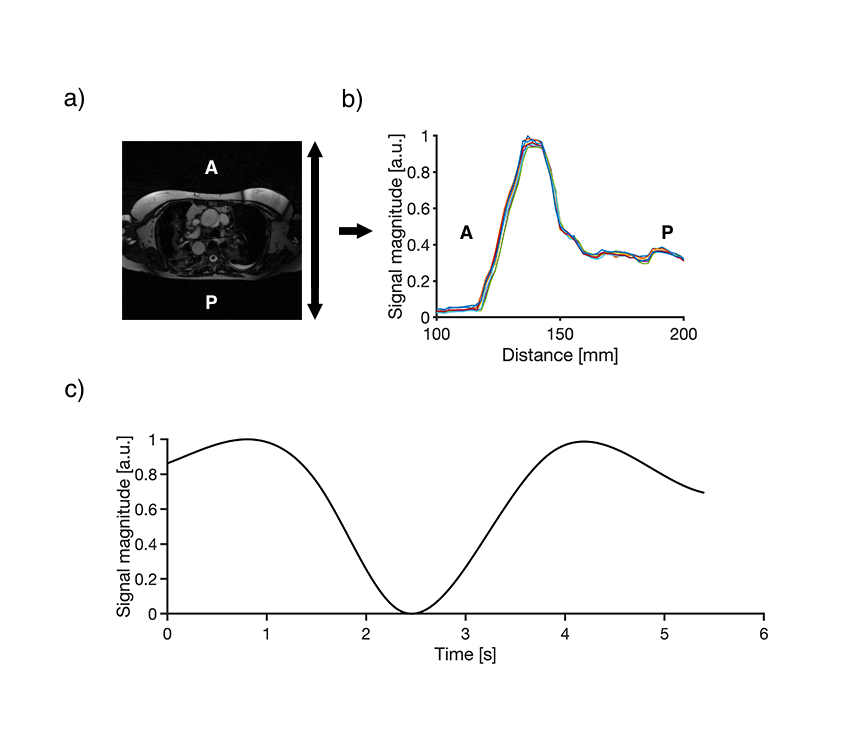
Two patients underwent MRI at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) using a prototype radial bSSFP pulse sequence with golden-angle ordering under free breathing. Both subjects gave written informed consent and the study was approved by the regional ethics board. Relevant sequence parameters were as follows; TE/TR: 1.8/3.6 ms, flip angle, 60°; field-of-view, 380×380 mm; matrix size, 240×240; slice thickness, 3 mm, 60 slices in the transversal plane, 1500 radial spokes per slice. Image reconstruction was performed using the XD-GRASP framework (3) in MATLAB. The motion signal was estimated from a sliding window reconstruction where each of the timeframes was collapsed along the left-right (LR) direction to form an image projection along the anterior-posterior (AP) direction, see Figure 1. The anterior chest wall was automatically tracked by fitting a sigmoid function over the signal profile and finding the mid-point of the fitted function (4). The estimated motion signal was then interpolated to full temporal resolution using spline interpolation. The efficacy of the self-gating method was evaluated by visual assessment of the slice registration using MPR, vessel sharpness measured as the image gradient at the border of the main pulmonary arteries and blood-to-blood clot contrast. which was evaluated as
$$C_{blood,clot} = \frac{S_{blood}-S_{clot}}{S_{blood}+S_{clot}}$$
Results
As evident from the MPR reconstruction, see Figure 2, the slice mismatch is significantly reduced in the self-gated reconstruction. The vessel sharpness did not differ (n = 48, 0.44±0.3 vs. 0.43±0.3, P = 0.96). The blood-to-blood-clot contrast did not differ (n = 16, 0.56±0.1 vs. 0.52±0.1, P = 0.43 for the free-breathing and the self-gated acquisitions respectively. Visual inspection of the free-breathing MPR’s revealed that each slice moved independently from each other, while in the self-gated MPR’s the slices were synchronized over the respiratory cycle, see Figure 2.Conclusion
The self-navigation capability of the golden-angle radial imaging shows potential for slice alignment in multi-slice 2D pulmonary imaging. Although residual misregistration remains due to imperfect detection of the respiratory motion, the slice aligned image stacks exhibited coherent motion compared to the free-breathing reconstruction in which each slice moved independently. Image-based self-navigation has the potential to be robust to erratic breathing, as often seen in the targeted patient group. Further work will show if the self-navigation can be further improved to reduce residual slice misregistration.Acknowledgements
No acknowledgement found.References
1. Nyren S, Nordgren Rogberg A, Vargas Paris R, Bengtsson B, Westerlund E, Lindholm P. Detection of pulmonary embolism using repeated MRI acquisitions without respiratory gating: a preliminary study. Acta radiol. 2017;58:272–278.2. Fyrdahl A, Vargas Paris R, Nyrén S, Holst K, Ugander M, Lindholm P, Sigfridsson A. Pulmonary artery imaging under free‐breathing using golden‐angle radial bSSFP MRI: a proof of concept. Magn. Reson. Med. 2018;80:1847–1856.
3. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn. Reson. Med. 2015;75:775–788.
4. Hui CK, Wen Z, Stemkens B, Tijssen RHN, Van Den Berg CAT, Hwang KP, Beddar S. 4D MR imaging using robust internal respiratory signal. Phys. Med. Biol. 2016;61:3472–3487.
Figures