4490
Effects of Image Registration in Dynamic Contrast-Enhanced MRI of the TMJ1Dept. of Physics and Technology, University of Bergen, Bergen, Norway, 2Mohn Medical Imaging and Visualization Centre, Haukeland University Hospital, Bergen, Norway, 3Dept. of Clinical Engineering, Haukeland University Hospital, Bergen, Norway, 4Institute of Scientific Instruments, Czech Academy of Sciences, Brno, Czech Republic, 5Dept. of Radiology and Nuclear Medicine, St. Olav hospital HF, Trondheim, Norway, 6Dept. of Circulation and Medical Imaging, Norwegian university of Science and Technology, Trondheim, Norway, 7Dept. of Radiology, University Hospital of North Norway, Tromsø, Norway, 8Norse, Bergen, Norway, 9Dept. of Radiology, Haukeland University Hospital, Bergen, Norway, 10Dept. of Clinical Sciences, University of Bergen, Bergen, Norway
Synopsis
The effect of elastic and affine motion correction in dynamic contrast enhanced MRI ofthe temporomandibular joints in children is investigated. Imaging in children is particularly difficultdue to motion. This hampers DCE-MRI and pharmacokinetic estimations for their potentialdiagnostic value in these children with Juvenile Idiopathic Arthritis with possible TMJ involvement.The relative enhancement curves obtained with different motion correction approaches arecompared with the curves calculated with the Gamma Capillary Transit Time model. It is found thatwhen image registration is applied, a greater number of participants can be analysed. The elasticmotion correction approach outperforms the affine approach.
Purpose:
To investigate the effect of elastic and affine motion correction in dynamic contrast-enhanced MRI (DCE-MRI) of the temporomandibular joints (TMJs) in children. Imaging in children is particularly difficult due to motion. This hampers DCE-MRI and pharmacokinetic estimations1, which are currently being investigated for their potential diagnostic value in children with Juvenile Idiopathic Arthritis with possible TMJ involvement.Methods:
The DCE-MRI data from the TMJ of 48 children with JIA are included, aged 6-15 years. The data is part of a larger set of data from a still ongoing study. It is part of an extensive imaging protocol acquired at three centres using Siemens Skyra 3T and a 64-channel head coil. A 3D-FLASHsequence was used (TR/TE/FA = 4ms/1ms/9°, image matrix 160x160x16, at 60 points in time with a temporal resolution of about 4s). Using a power injector, the contrast agent Gd-DOTA (Dotarem®) was injected 10s after acquisition start (injection speed 5 mL/s). Regions-of-interest (ROIs), i.e. masks of the left and right TMJ, were manually selected in consensus by three expert paediatric radiologists allowing the extraction of relative enhancement curves from the DCE-MRI data.
Parmacokinetic parameters were estimated in the right and left TMJ in each participant comparing three different pre-processing schemes: i) no motion correction,(non-registered), ii) affine motion correction of the whole image volume using the Elastix software 2,3 (affine), iii) elastic registration over the TMJs using an inhouse developed implementation of elastic registration originally developed for DCE-MRI of the kidneys 4 (elastic). The pharmacokinetic parameters blood plasma flow (Fp ), initial extraction fraction(E), volume of extravascular extracellular space (ve), capillary mean transit time (Tc), width of transit time distribution (α-1 ) and bolus arrival time (BAT) were computed using the Gamma Capillary Transit Time (GCTT) model.5
Results:
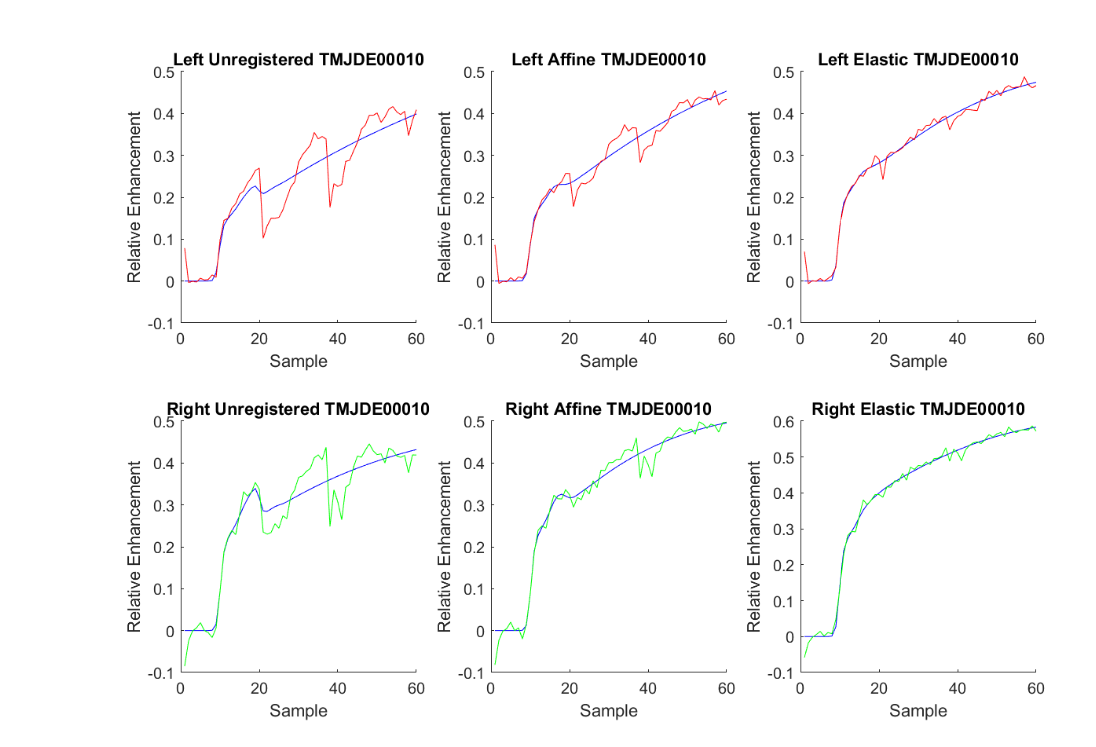
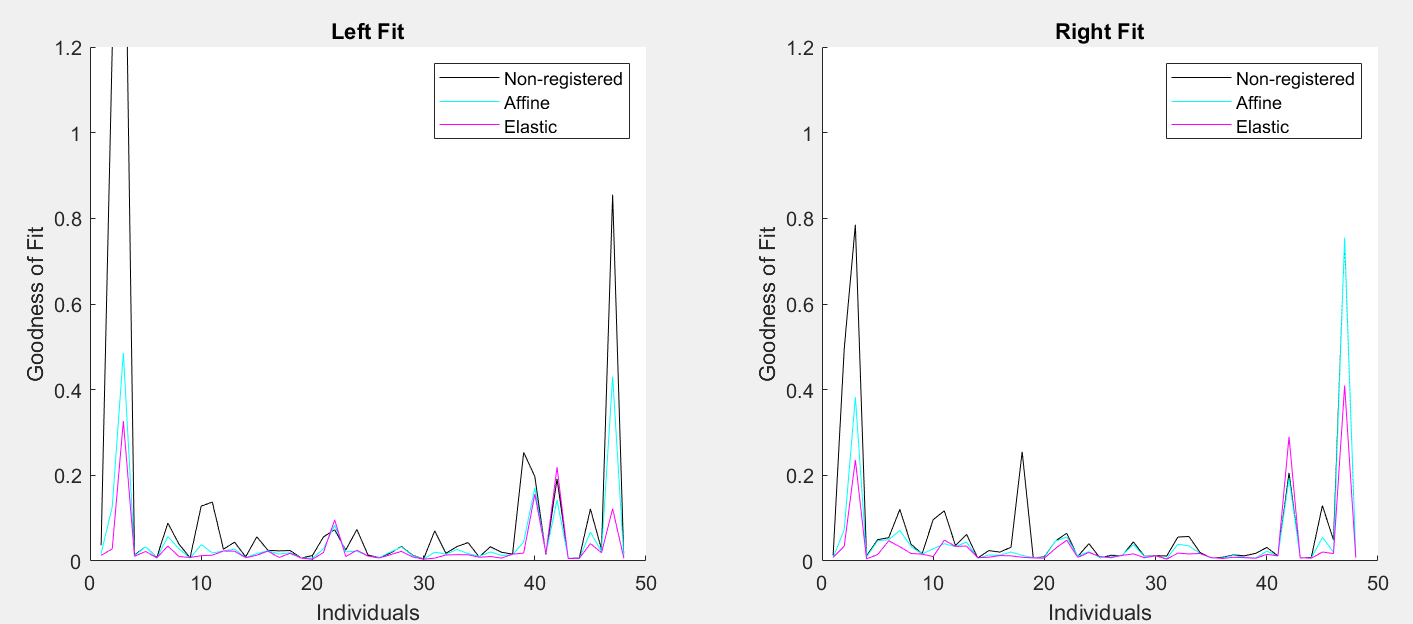
Visual inspection of the effect of various level motion correction were promising, cfr. the randomly selected case in Fig. 1, where model estimations (GCTT) are overlaid. The goodness of fit,Fig. 2, of the three approaches (non-registered, affine and elastic correction) shows that the model best describes the underlying measured data for elastic transformations which outperforms the affine transformation and non-registered, cfr. Tab.1 for sum-of-squares for each model across participants. The estimated parameters from the GCTT modelling show that there are fewer outlier data for the elastic registration, particularly for Fp, E, Tc and BAT potentially indicating that erroneous estimations are reduced, Fig. 3.Discussion:
The results show that image registration, and specifically the elastic ROI approach to image registration, results in a better fit of the GCTT model. A greater variation in parameter values is expected when moving patients are included in the non-registered data, and registration in the current data is reducing outliers of the estimated parameters. However, to further investigate if the registration influences the diagnostic value of disease affection in TMJ in these children more information on clinical data and multimodal data (structural MRI, ultrasound, CT) is required to better classify the patients into active disease versus chronic affection.Conclusion:
Image registration is of importance in the evaluation of DCE-MRI in the TMJ in children, as seen by the increased smoothness of the time curves post registration and by the better model fit of the model to the data. Elastic registration of the TMJs, outperformed affine registration in that its fit to the GCTT model is better. Image registration will facilitate DCE-MRI analysis also in participants where analysis otherwise is not possible due to large motion artefacts and hence increase the potential diagnostic value of DCE-MRI in Juvenile Idiopathic Arthritis affecting the TMJs.
Acknowledgements
The work was supported by European Regional Development Fund-Project "Modernization and support of research activities of the national infrastructure for biological and medical imaging Czech-BioImaging" (No. CZ.02.1.01/0.0/0.0/16_013/0001775) and by the MEYS CR (LO1212).References
1. Macíček O. Andersen E, Angenete O, Augdal T, Rosendal K, Jiřík R, Grüner R, ISMRM 2018, Paris.
2. S. Klein, M. Staring, K. Murphy, M.A. Viergever, J.P.W. Pluim, " elastix: a toolbox for intensity based medical image registration," IEEE Transactions on Medical Imaging 2010; 29: 196 - 205.
3. D.P. Shamonin, E.E. Bron, B.P.F. Lelieveldt, M. Smits, S. Klein and M. Staring, & quot; Fast Parallel Image Registration on CPU and GPU for Diagnostic Classification of Alzheimer’s Disease & quot;, Frontiers in Neuroinformatics 2014; 50: 1-15.
4. Hodneland E. et al. Normalized gradient fields for nonlinear motion correction of DCE-MRI time series. Computerized Medical Imaging and Graphics 2014; 38: 202-210.
5. Schabel M. C. A unified impulse response model for DCE-MRI. Magnetic Resonance in Medicine 2012; 68:1632–1646.
Figures