4483
Deformable slice-to-volume registration for respiratory motion correction in abdominal and in-utero MRI1King's College London, London, United Kingdom
Synopsis
This work introduces deformable slice-to-volume registration (DSVR) integrated into super-resolution reconstruction framework for correction of respiratory motion MRI. Using the initial estimation of respiratory motion as an input this method allows reconstruction of high-resolution volumes for specific respiratory positions using all slices. Based on diffeomorphic free-form deformation model, DSVR provides robust registration of deformable objects as well as out-of-plane motion correction. The feasibility of the method was successfully evaluated on a ‘motion-corrupted’ phantom and a free-breathing in-utero MRI scan. The results also indicated that the accuracy of spatial features in reconstructed volume is directly defined by the initial motion estimation.
Introduction
The recent advances in respiratory motion estimation provide robust solution for reconstructing anatomically consistent 3D+T abdominal MRI1. However, the impact of such factors as inter-cycle and correspondence model variations and exclusion of slices reduces spatial resolution and data efficiency. This is generally addressed by registration of sequential slices or volumes2,3. Slice to volume registration (SVR) in conjunction with super-resolution (SR) reconstruction has proven to be a robust strategy for motion correction for MRI of rigidly moving objects such as fetal brain4,5. Incorporation of deformable registration into SVR would allow reconstruction of abdominal MRI using slices from different respiratory positions to obtain high-resolution volumes. Another advantage of SVR is that it allows correction of out-of-plane motion. In this work, we propose a deformable SVR reconstruction (DSVR) framework for respiratory motion correction in MRI. The feasibility of the method was evaluated on a ‘motion-corrupted’ phantom and a free-breathing in-utero MRI scanMethods
The proposed approach combines the following steps: (1) SR reconstruction of a blurred template with global features from a group of slices corresponding to a specific respiratory position; (2) deformable registration of all slices to the template volume; (3) SR reconstruction of high-resolution volume. Implemented in MIRTK6, the pipeline is based on the well-established algorithm for rigid SVR reconstruction for fetal brain MRI3 extended with diffeomorphic free-form deformation (FFD) model parametrized by stationary velocity field7. The SR reconstruction is performed under the assumption of 3D Gaussian PSF and employs robust statistics scheme for outlier rejection. For the purpose of this study, in order to eliminate the impact of possible error propagation from motion estimation methods, the slice selection for inhale, exhale and resting states was performed manually.
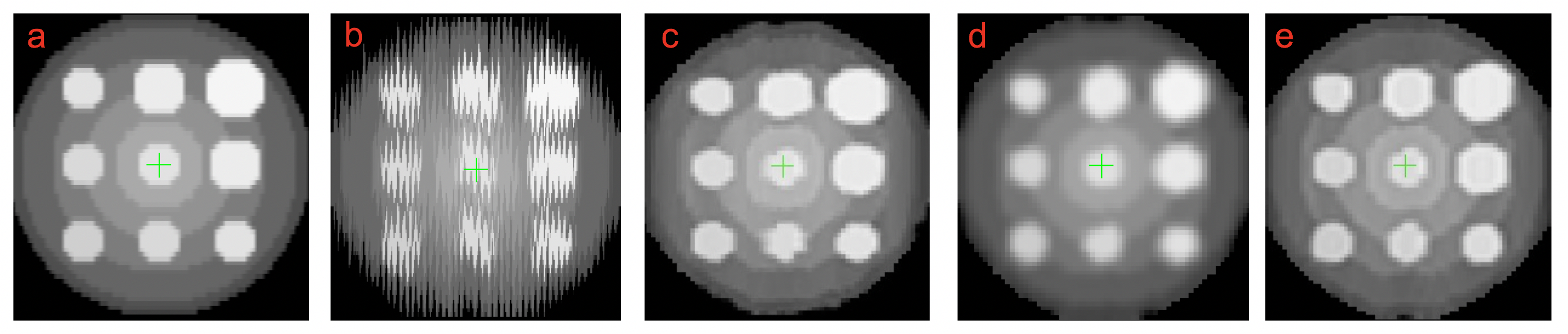
a) Phantom experiment: Simulated datasets were generated by application of FFD transformations replicating breathing motion (extracted from abdominal MRI) to each slice of a 3D ‘stationary’ phantom (Figure 1.a). The method’s efficiency was evaluated in terms of normalized root mean square error (NRMSE) between the ‘stationary’ ground truth volume and the motion corrected reconstructed volume.
b) In-vivo experiment: The feasibility of the DSVR method was evaluated on one in-utero MRI scan of a healthy volunteer acquired with a modified 2D bSSFP sequence that sweeps continuously across a 3D volume by shifting the frequency offset for each excitation pulse8. Only one stack of slices (resolution 1.3x1.3x4mm, slice spacing 0.2mm) was available for this case. The reconstruction quality was assessed visually and by calculating normalized cross-correlation (NCC) between consecutive slices for a specific ROI.
Results
Figure 1 shows the reconstruction results for a motion corrupted phantom (NRMSE > 0.15) (b) with the classical SVR (c) and proposed DSVR (e) methods. Although the classical rigid SVR with outlier rejection removes a significant amount of motion artefacts (c), it also results in blurring and inconsistencies in structural features due to the impact of deformable motion transformations (NRMSE = 0.083). Using only selected slices (25-35%) corresponding to the ‘resting state’ for the template (d) preserves spatial information, but lowers spatial resolution. Application of DSVR of all slices to the template improved the image quality (e) with NRMSE = 0.050 and the majority of features being preserved (Figure 2).
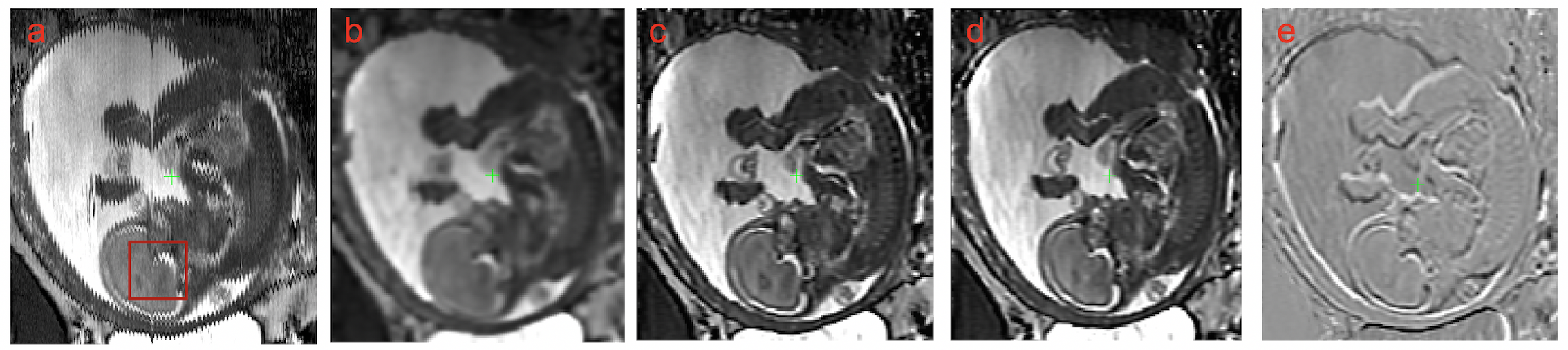
Figure 3 shows the results of DSVR reconstruction for one of the in-vivo cases: the original volume (a), the template example (b), results of DSVR for exhale (c) and inhale (d) positions and their difference (e). In summary, the method successfully reconstructed the volume in different respiratory positions using all slices and low-resolution templates. The average sequential slice NCC for the selected region of interest (a) was 0.89 before and 0.96 ± 0.01 after reconstruction.
Conclusion
This work introduced DSVR reconstruction method for respiratory motion correction in MRI. The results demonstrated that integration of deformable SVR into the standard SR reconstruction provides a robust solution for correction of motion artefacts and increases spatial resolution. The current limitation of the proposed method is that the accuracy of spatial features in reconstructed volume is directly defined by the initially selected respiratory position. The challenge of irregular motion should be addressed by using several orthogonal stacks for reconstruction along with advanced motion estimation methods. Further work will focus on optimization of DSVR parameters for topology preservation and integration of motion estimation into the reconstruction loop.Acknowledgements
This work was supported by by the NIH Human Placenta Project grant [1U01HD087202-01], the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z) and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Baumgartner, C.F., Kolbitsch, C., McClelland, J.R., Rueckert, D., King, A.P., 2017. Autoadaptive motion modelling for MR-based respiratory motion estimation. Med. Image Anal. 35, 83–100.
2. Hamy, V., Dikaios, N., Punwani, S., Melbourne, A., Latifoltojar, A., Makanyanga, J., Chouhan, M., Helbren, E., Menys, A., Taylor, S., Atkinson, D., 2014. Respiratory motion correction in dynamic MRI using robust data decomposition registration - Application to DCE-MRI. Med. Image Anal. 18, 301–313.
3. Kuklisova-Murgasova, M., Quaghebeur, G., Rutherford, M.A., Hajnal, J. V., Schnabel, J.A., 2012. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med. Image Anal. 16, 1550–1564.
4. Gholipour, A., Afacan, O., Aganj, I., Scherrer, B., Prabhu, S.P., Sahin, M., Warfield, S.K., 2015. Super-resolution reconstruction in frequency, image, and wavelet domains to reduce through-plane partial voluming in MRI. Med. Phys. 42, 6919–6932.
5. The Medical Image Registration ToolKit (MIRTK) [WWW], 2018. URL https://biomedia.doc.ic.ac.uk/software/mirtk/
6. Schuh, A., Murgasova, M., Makropoulos, A., Ledig, C., Counsell, C. J., Hajnal, J. V., Aljabar, P., Rueckert, D., 2014. Construction of a 4D brain atlas and growth model using diffeomorphic registration. In: MICCAI, LNCS, 8682, pp. 27-37.
7. Jackson, L. H., Price, A. N., Hutter, J., Cordero-grande, L., Ho, A., Slator, P, J., Dos Santo, A., Van Amerom, J. F. P., Murgasova, M., Mccabe, L., Rutherford, M. A., V Hajnal, J.V., 2018. Respiration resolved imaging using continuous steady state multiband excitation with linear frequency sweeps. In: ISMRM, pp. 5–7.
Figures