4477
Unraveling the effect of spatial resolution and scan acceleration on 3D image-based navigators for respiratory motion tracking1Electrical Engineering, Stanford University, Stanford, CA, United States
Synopsis
Beat-to-beat 3D image-based navigators (3D iNAVs) enable nonrigid respiratory motion tracking of the heart. In this work, we study the accuracy of motion information extracted from 3D iNAVs with different choices of two parameters: spatial resolution and scan acceleration factor. We demonstrate that high spatial resolution coupled with aggressive scan acceleration results in residual blurring and aliasing following iterative reconstruction, which corrupts the derived motion estimates. Through simulations, we identify the optimal combination of spatial resolution and scan acceleration for acquiring 3D iNAVs. In vivo studies presenting sharp motion correction outcomes demonstrate a capability for monitoring motion with high fidelity.
Introduction
Recently, beat-to-beat 3D image-based navigators (3D iNAVs) have been proposed as a means of monitoring the nonrigid motion of the heart1. To collect a 3D iNAV in a single heartbeat, a non-Cartesian cones trajectory, a variable-density sampling scheme, and a compressed sensing reconstruction approach are helpful2,3,4. In this study, we develop a simulation framework to examine the fidelity of respiratory motion estimates obtained from 3D iNAVs with varying spatial resolutions and degrees of scan acceleration. For navigators beyond certain scan acceleration factors, we identify that the accuracy of motion estimates is compromised due to higher levels of blurring and aliasing.Methods
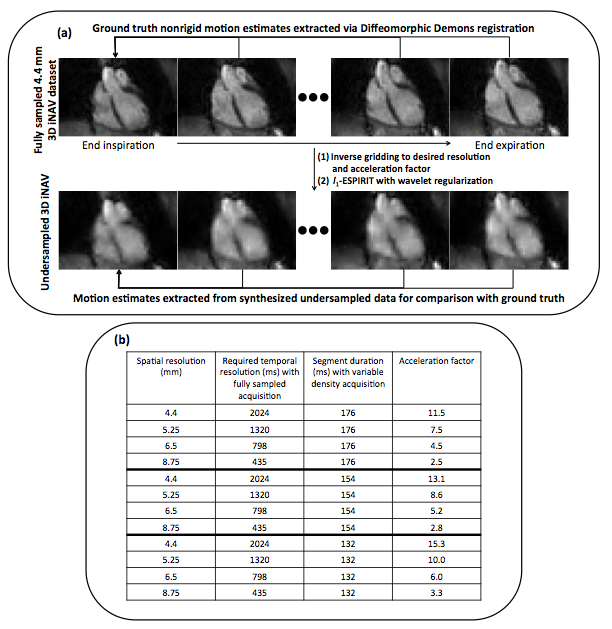
Our study begins with the collection of fully sampled, breath-held, and cardiac-gated 4.4 mm spatial resolution 3D iNAVs at six respiratory phases from end-expiration to end-inspiration with a temporal resolution of 90 ms, corresponding to 18 cone readouts per heartbeat. Because these 3D iNAVs do not exhibit undersampling artifacts, the voxel-by-voxel nonrigid motion estimates derived from them (via Diffeomorphic Demons (DD) registration) with respect to the end-expiration navigator serve as the ground truth (Figure 1(a)).
To analyze the effect of spatial resolution and undersampling, we generate a total of twelve variable-density cones trajectories with a combination four spatial resolutions (4.4 mm, 5.25 mm, 6.5 mm, and 8.75 mm) and three segment durations (176 ms, 154 ms, and 132 ms) (Figure 1(b)). The k-space data corresponding to these trajectories are computed from the fully sampled 4.4 mm 3D iNAV dataset via inverse gridding. l1-wavelet ESPIRiT is applied to reconstruct twelve sets of 3D iNAVs at six different respiratory phases5. Note that the analysis of segment durations does not consider the effect of possible temporal blurring of the heart. We nonetheless incorporate segment duration in our simulation, as a shorter acquisition of 3D iNAVs might, for example, be beneficial in patients with abnormal ventricular function, where significant cardiac motion may occur even during diastole.
Nonrigid motion estimates for each of the twelve navigator configurations are derived using DD image registration. Applying mean absolute error (MAE) as the similarity metric, we compare these motion estimates to the ground truth obtained from the fully sampled 4.4 mm dataset.
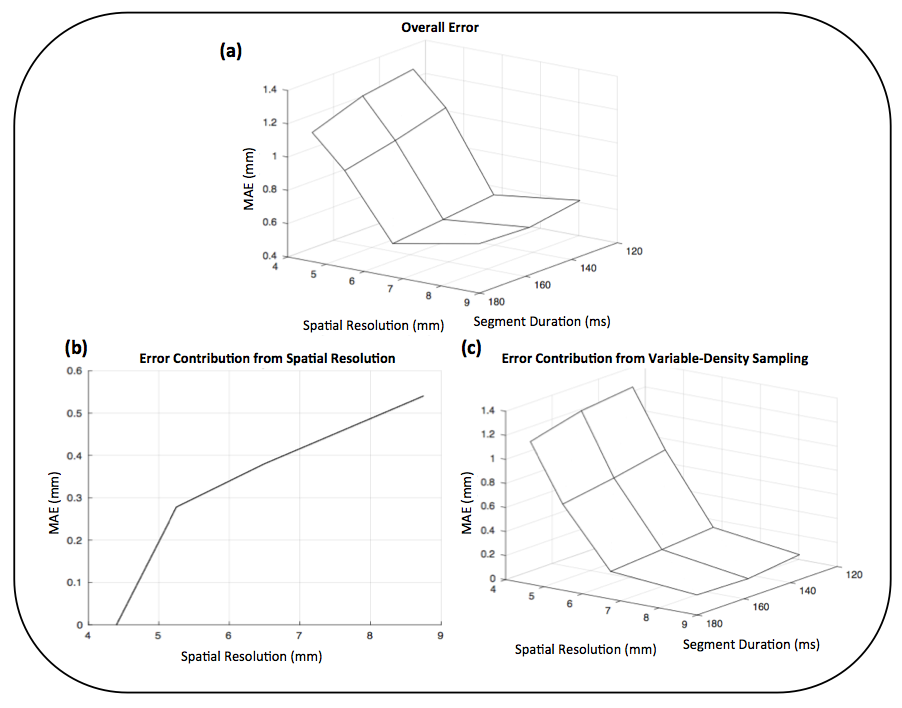
Inaccuracies in motion estimates from the synthesized data can be due to the lower spatial resolution with respect to the ground truth or residual aliasing from the variable-density sampling pattern following iterative reconstruction. To separate these two effects, we create fully sampled 5.25 mm, 6.5 mm, and 8.75 mm datasets by appropriately truncating the k-space data of the fully sampled 4.4 mm 3D iNAVs. DD registration is applied to these generated datasets, and the resulting motion information is compared using MAE to that obtained from fully sampled 4.4 mm 3D iNAVs. By subtracting the error due to spatial resolution calculated here from the total error determined above, we isolate the influence of residual aliasing in the 3D iNAVs on the extracted motion estimates.
Results
When the error from spatial resolution and residual aliasing are combined, a minimum in overall MAE is seen at a spatial resolution of 6.5 mm and segment duration of 176 ms (Figure 2(a, b, c)). With this specific 3D iNAV configuration, the error due to the lower spatial resolution is counteracted by the benefits of reduced aliasing. Note that at a spatial resolution of 6.5 mm, decreasing the acquisition duration to 132 ms from 176 ms increases MAE by approximately 0.1 mm. The advantage from reduced temporal blurring at this shorter acquisition duration might offset this error, but experiments investigating this speculation are beyond the scope of this work.
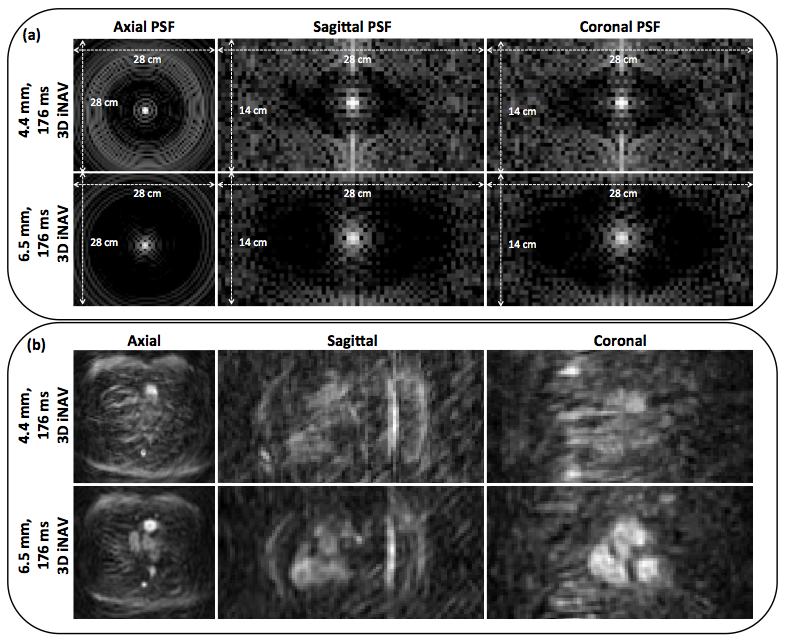
Analysis of point spread functions (PSFs) corroborates the quantitative trends (Figure 3). The PSF of the higher resolution 3D iNAV exhibits aliased signal throughout the FOV. l1-wavelet ESPIRiT does not completely mitigate the effects of such severe aliasing, which diminishes the advantages associated with high spatial resolution motion tracking.
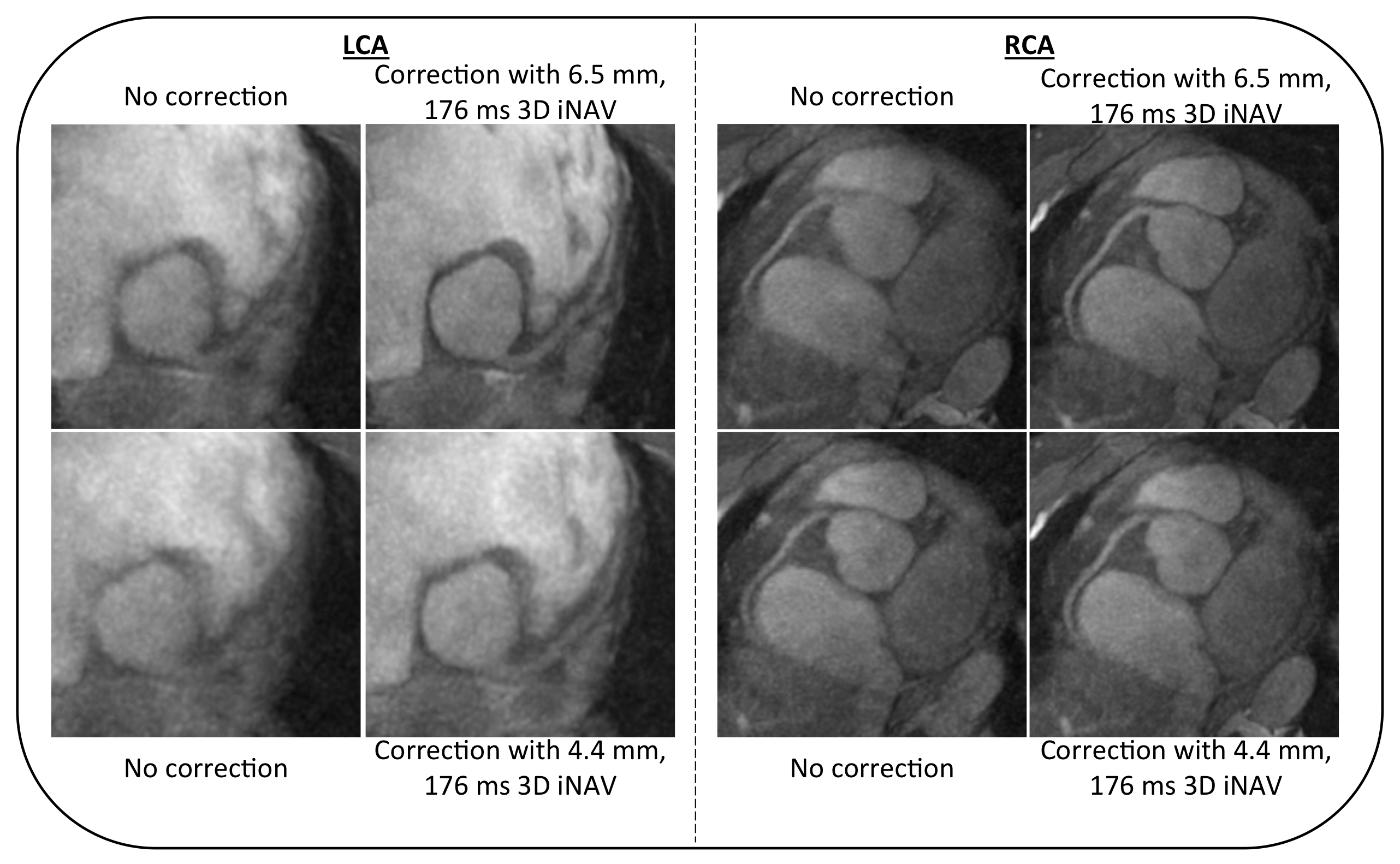
Videos of beat-to-beat 3D iNAVs acquired in 176 ms with the optimal 6.5 mm spatial resolution demonstrate enhanced motion tracking capability with sharp structures and minimal aliasing artifacts (Figure 4). Improvements in motion correction outcomes for in vivo subject studies are observed when integrating the 6.5 mm 3D iNAVs into a generalized matrix description framework (Figure 5).
Discussion and Conclusion
We have analyzed the effect of spatial resolution and scan acceleration on the fidelity of motion tracking for cardiac imaging. A higher spatial resolution 3D iNAV, if fully sampled, results in better motion estimates. But, with undersampling, the advantages associated with high spatial resolution motion tracking are offset by the presence of residual aliasing following iterative reconstruction.Acknowledgements
We gratefully acknowledge the support of NIH grants R01HL127039, T32HL007846, and T32EB009653. This work was also supported by the Hsi-Fong Ho Stanford Graduate Fellowship, the Ruth L. Kirschstein National Research Award, and the National Science Foundation Graduate Research Fellowship under Grant No. DGE-114747.References
[1] Addy et al. Magnetic Resonance in Medicine 77.5 (2017): 1874-1883.
[2] Lustig et al. Magnetic Resonance in Medicine 58.6 (2007): 1182-1195.
[3] Tsai et al. Magnetic Resonance in Medicine 43.3 (2000): 452-458.
[4] Gurney et al. Magnetic Resonance in Medicine 55.3 (2006): 575-582.
[5] Uecker et al. Magnetic Resonance in Medicine 71.3 (2014): 990-1001.
Figures