4459
T1 mapping with golden-angle radial sampling: A comparison of direct and indirect reconstruction1Leeds Institute of Biomedical and Clinical Sciences, University of Leeds, Leeds, United Kingdom, 2Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom
Synopsis
The purpose of the study is to compare a direct model-based reconstruction with an indirect compress sensing reconstruction for the estimation of T1-map, from simulated radial sampled datasets. Comparisons are performed for the binning strategy that is optimal in each case as measured by T1-errors.
The direct reconstruction solves the nonlinear-least-squares optimization problem with a gradient-based L-BFGS algorithm without regularization, while for the indirect method the images are reconstructed using the iGRASP technique.
The accuracy for both methods is similar, however the computational time of the model-based reconstruction is a limiting factor for clinical applications.
Introduction
Direct model-based reconstruction for golden-angle radial sampling schemes is an attractive option for quantitative MRI1-3 as it allows for a perfect temporal fidelity in the presence of evolving magnetisation and is well-determined without regularisation – producing a purely data-driven reconstruction. Indirect compressed-sensing reconstruction is significantly faster but requires binning of radial k-space lines into frames, which either impacts temporal fidelity (if many k-space lines are binned) or requires heavy regularisation that reduces data dependence (if very few k-space lines are binned). The aim of this study is to compare the two approaches using digital phantoms, and for the special case of saturation-recovery T1-mapping. Comparisons are performed for the binning strategy that is optimal in each case as measured by T1-errors.Methods
Model-based reconstruction of spin density Mo and relaxation time T1-maps, after a saturation recovery (SR) magnetization preparation, solves the nonlinear-least-squares optimization problem
$$(M_0 (\textbf{r}),T_1 (\textbf{r}))=\underset{(M_0 (\textbf{r}),T_1 (\textbf{r}))}{argmin}∑_t‖y(\textbf{k},t)-f(M_0 (\textbf{r}),T_1 (\textbf{r}),t)‖_2^2 \qquad [1] $$
where $$$y(\textbf{k},t)$$$ is the raw data and f is the operator which converts the Mo and T1 maps to ($$$(\textbf{k},t)$$$-space by performing a NU-FFT on the signal after a saturation pulse at time point t:
$$f(M_0,T_1,t)=NUFFT [ S(M_0,T_1,t)] \qquad [2]$$
$$S= (M_0 (1-exp(-t/T1) \qquad [3] $$,
where the mono-exponential relation (eq.3) represents the model for the signal behaviour after the SR magnetization preparation. Optimisation is performed with the gradient-based L-BFGS algorithm4, subject to bound constraints, allowing only positive values. The maximum number of L-BFGS iterations was set to 200. For the indirect method, the signal model (eq.3) is fitted on the images reconstructed by the iGRASP5, by a trust-region-reflective algorithm. All calculations were performed in MATLAB (The MathWorks, MA) on a PC (Intel i5@3.30GHz, 8GB RAM). For the iGRASP reconstruction we used the available online Matlab implementation.
Two digital reference objects were created by simulating the signal evolution after a single saturation pulse assuming free recovery, using a pseudo-continuous sampling interval TS.
a) A modified Shepp-Logan phantom (Matrix:256x256;Overall Acquisition Time:1000ms;TS:1ms;Total no. Spokes:1000) with predefined values for Mo and T1 (Fig.1)
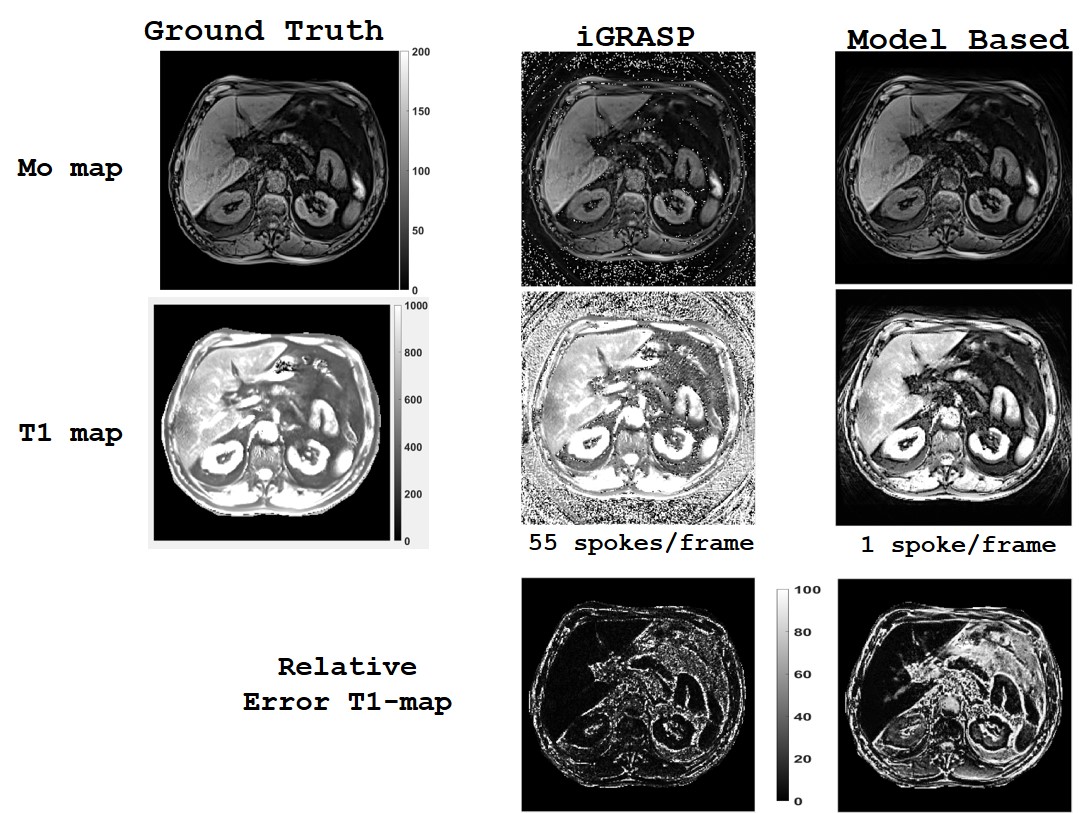
b) An abdomen phantom (Matrix:256x256;Overall Acquisition Time:4000ms;TS:3 ms; Total no. Spokes:1333), with predefined Mo and T1 maps (Fig.5) calculated using the MOLLI6 sequence. The simulated signal images S(r,t) were converted to radial S(k,t)-data where each spoke was acquired for each TS using the NU-FFT and the golden-angle scheme. The data were retrospectively combined into frames S(k, tf) of binning spokes (1-89) leading to sampling rates of TR =1xTS to TR = 89xTS, where tf is defined as the time point of the central spoke in the frame.
ROIs were selected for the estimation of the relative errors(RE=|Rec – Ref|/Ref). The optimum value of spokes per frame is estimated by finding the minimum value of the RE across the sampling rates.
Results
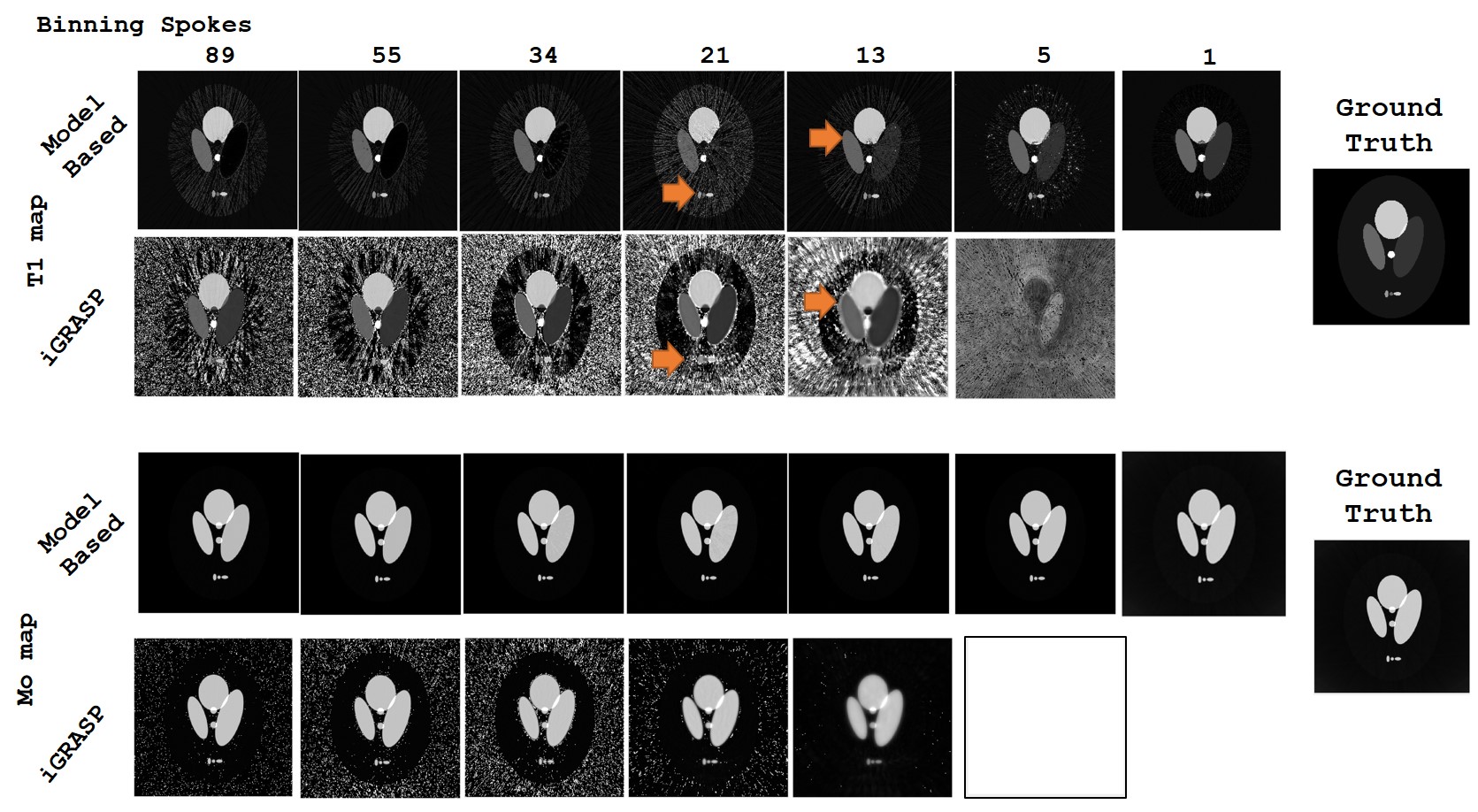
Figure 1 presents the reconstructed maps using the direct and indirect methods. The image quality of the Model-based reconstruction is better for all sampling rates than the indirect method, preserving the features of the T1-map (boundaries, shape) without contamination of excessive noise. The Mo-map is less affected by the number of the binning spokes for both reconstructions.
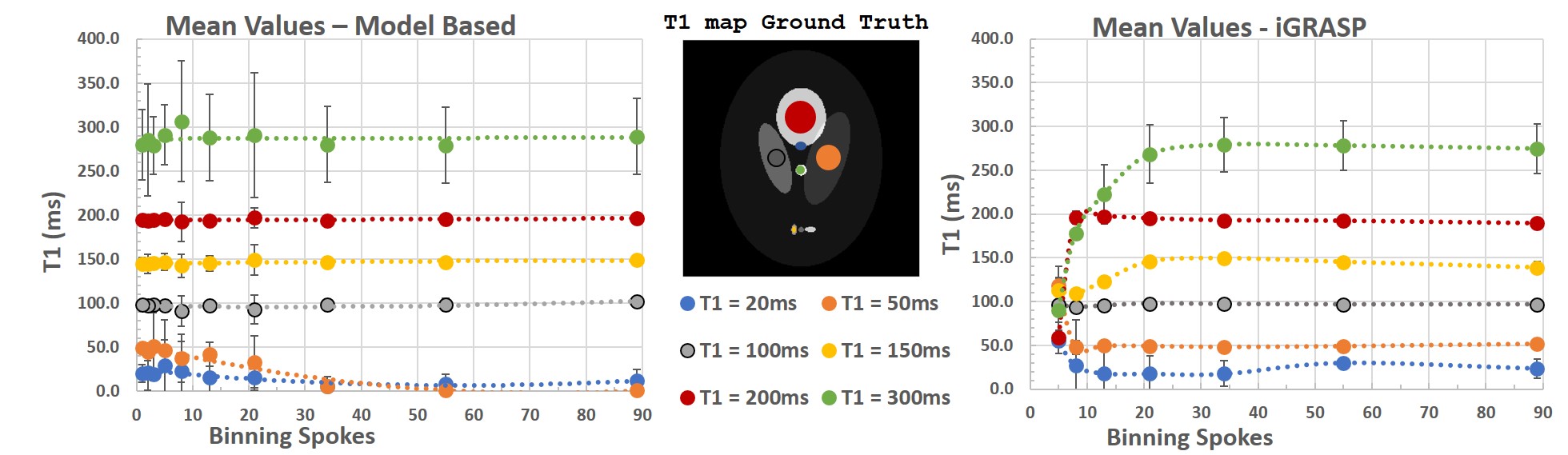
Figure 2 shows the mean values of the ROIs. The Model-based reconstruction fails to estimate the low T1 values for sampling rates over 21ms (21xspokes), while the iGRASP accuracy drops due to the noise induced as the result of binning less than 21 spokes/frame .
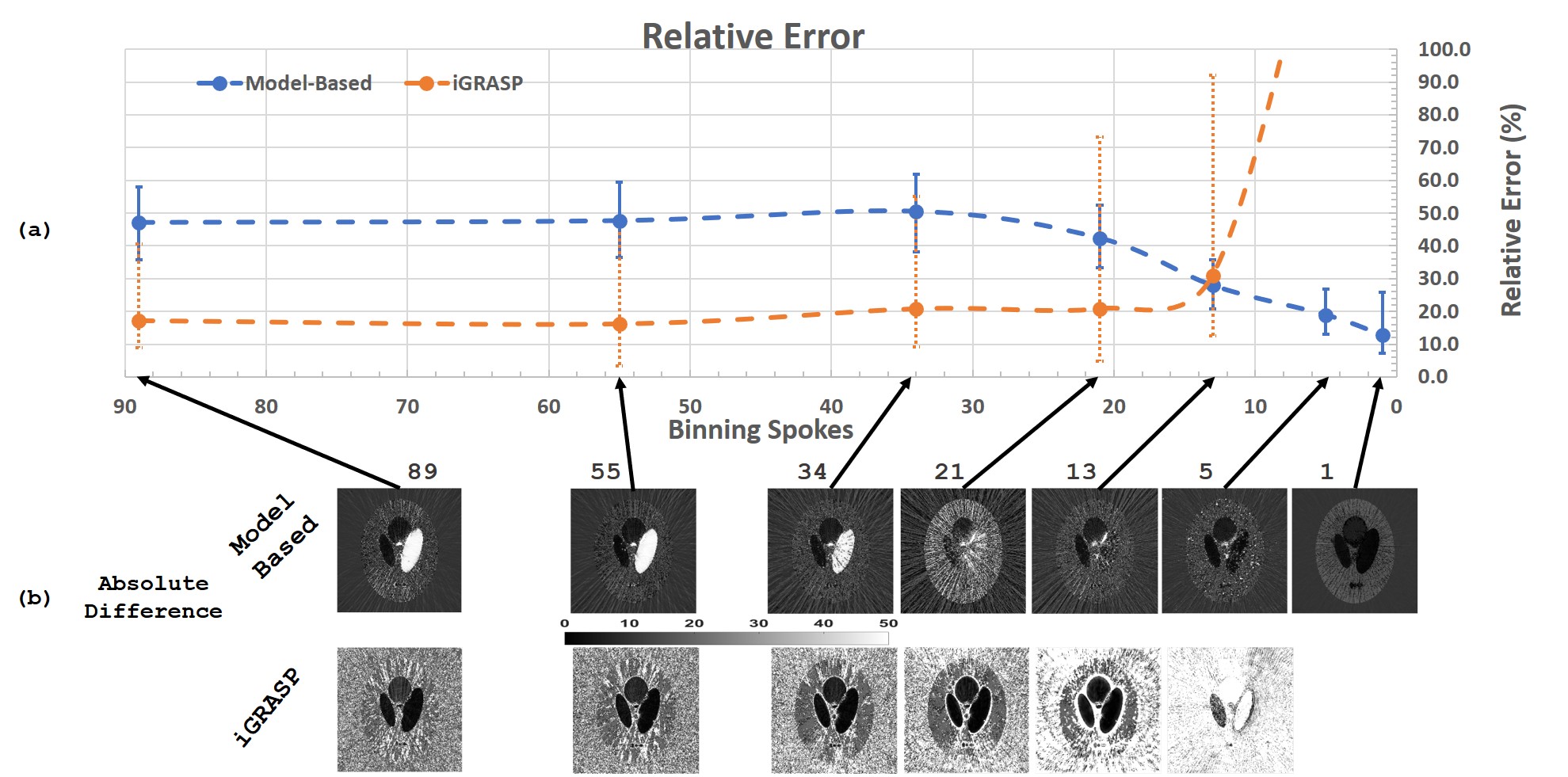
Figure 3, shows that the reduction of the number of binning spokes, increasing the sampling rate, improves the accuracy of the Model-based reconstruction. The optimum number of binning spokes for the model-based reconstruction seems to be one, while for the iGRASP is fifty-five.
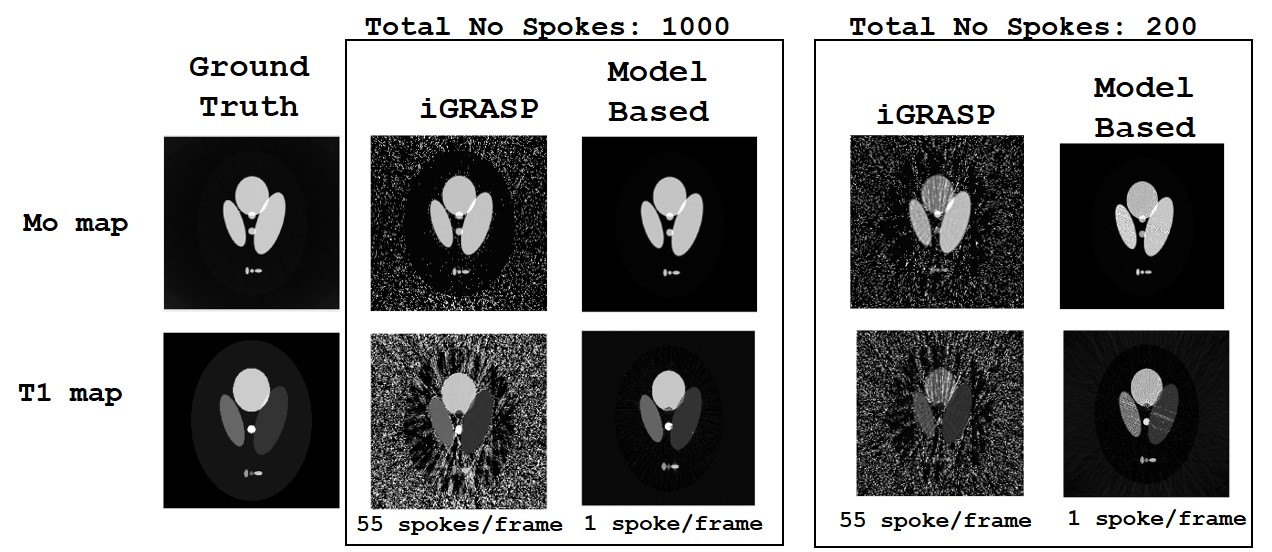
Figure 4, presents the reconstructed maps using the optimum number of binning spokes per dynamic frame. Using one-fifth of the data (acquiring 200 spokes), we notice that the Model-based method is more robust to reduced sampling duration than iGRASP.
Figure 5 displays the reconstructed maps of the simulated abdominal
phantom. The iGRASP reconstruction achieves better results than the Model-based
reconstruction, however this is mainly due to the early termination of the optimization algorithm.
Discussion
Model-based
reconstruction provides accurate maps, exploiting
a perfect temporal fidelity without a regularization term. Furthermore, the accuracy of the model-based reconstruction improves by combining
less radial data, while for the iGRASP the accuracy is
higher within a range of binning spokes. The disadvantage of the present
implementation, is a significantly higher computational requirement.Conclusion
Model based reconstruction seems to produce better results
by a purely data-driven reconstruction, but improvements
are small and considering the calculation times it is not immediately obvious
clear the benefit is there in real data.Acknowledgements
No acknowledgement found.References
1. Wang, X. et al. Model-based T1 mapping with sparsity constraints using single-shot inversion-recovery radial FLASH. Magn Reson Med 79, 730-740, doi:10.1002/mrm.26726 (2018).
2. Tran-Gia, J., Bisdas, S., Kostler, H. & Klose, U. A model-based reconstruction technique for fast dynamic T1 mapping. Magn Reson Imaging 34, 298-307, doi:10.1016/j.mri.2015.10.016 (2016).
3. Roeloffs, V. et al. Model‐based reconstruction for T1 mapping using single‐shot inversion‐recovery radial FLASH. International Journal of Imaging Systems and Technology 26, 254-263 (2016).
4. Schmidt, M. minFunc: unconstrained differentiable multivariate optimization in Matlab, <http://www.cs.ubc.ca/~schmidtm/Software/minFunc.html> (2005).
5. Feng, L. et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 72, 707-717, doi:10.1002/mrm.24980 (2014).
6. Messroghli, D. R. et al. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med 52, 141-146, doi:10.1002/mrm.20110 (2004).
Figures