4433
Markerless real-time motion correction for 2D RARE: reducing artefacts in clinical T2 and FLAIR MRI1Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States, 2Department of Radiology, Harvard Medical School, Boston, MA, United States, 3Department of Radiology, Boston Children's Hospital, Harvard Medical School, Boston, MA, United States, 4Fetal-Neonatal Neuroimaging and Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 5Radiology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, United States
Synopsis
This study investigates high-frequency prospective motion correction (PMC) using markerless face tracking for artefact reduction in clinical T2 and FLAIR MRI. The FOV pose was corrected before the acquisition of each slice in PMC sequences and five subjects were scanned with 1:16 min T2, 4:55 min T2, and 1:50 min FLAIR protocols. The multi-slice segmented RARE sequences showed high sensitivity to changes in head position but use of PMC scans consistently recovered good image quality with higher image sharpness as measured by the Tenengrad metric.
Target Audience
Researchers and clinicians interested in using markerless external motion tracking systems to correct artefacts caused by head motion during clinical T2 and FLAIR MRI.Introduction
Motion is a major problem in clinical MRI leading to degraded image quality and wasted scan time1. In extreme cases, sedation is required, which has associated risks and use with children is cautioned in a recent FDA warning. Prospective motion correction (PMC) using markerless optical tracking of the face has been shown to reduce motion artefacts in 3D-encoded sequences2-5. Multi-slice segmented sequences that encode each slice for over 1 min can also have high sensitivity to motion. In this study, markerless PMC was applied to RARE sequences6 used routinely in clinical MRI. In vivo motion experiments were performed with short and long duration T2 protocols, and a FLAIR scan.Methods
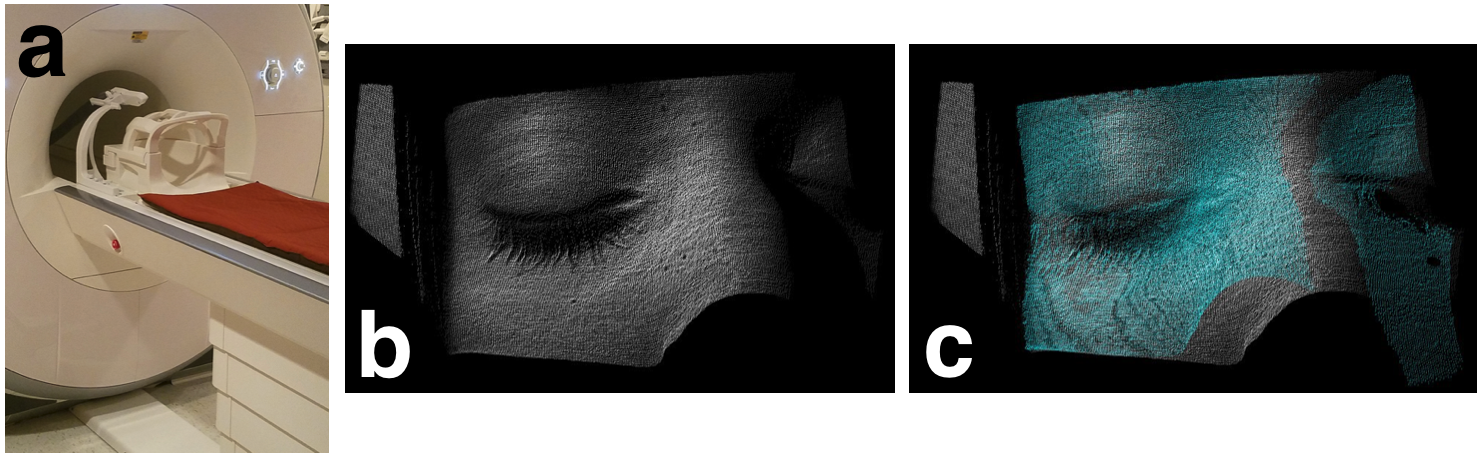
The “Tracoline” TCL3.01 markerless motion tracker with software version 3.0 (TracInnovations, Ballerup, Denmark) was used to estimate head motion2-4. The Tracoline system uses a structured infra-red light source and an optical camera attached to the scanner table (Fig. 1a) to reconstruct a 3D “point cloud” model of the subject’s face, specifically around the nose and the eyes. These point clouds are registered to an initial reference point cloud (Fig. 1b-c) to provide up to 30 motion estimates per second. The cross-calibration between camera and scanner coordinates was found with a pre-calibration using a ginger vegetable phantom. The cross-calibration matrix was corrected for table position after the subjects were positioned.
T2 and FLAIR RARE sequences were modified to apply transformations to the imaging FOV using motion information from the markerless tracking system. The FOV was updated before the start of each slice and the sequence instructions were written 20ms in advance of their execution. Data were acquired on a 3T Siemens Prisma scanner with a 64-channel head coil.
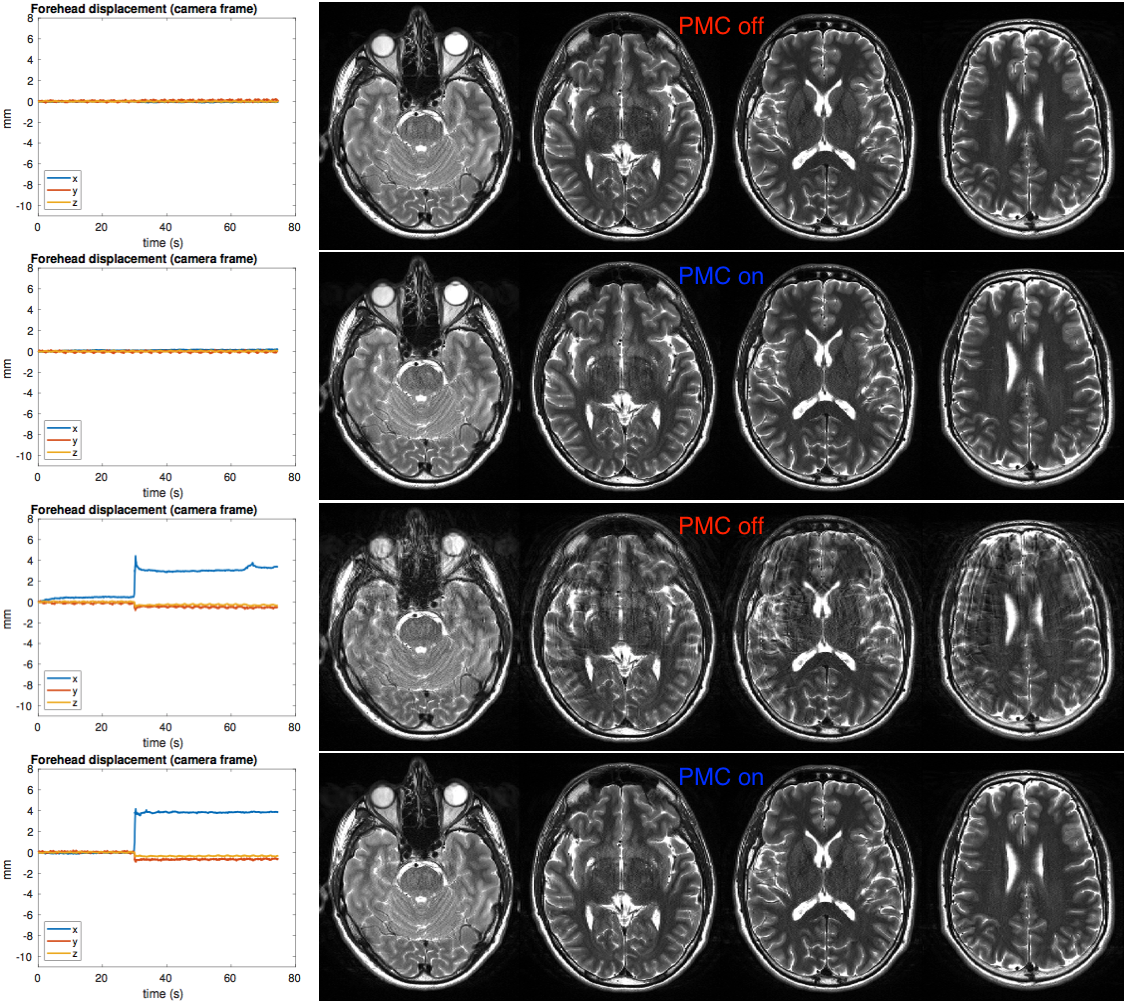
1:16min “T2-fast” protocol: TR=8.31s, TE=106ms, FOV=220x178.9mm2, matrix=512x358, 36 axial 3mm slices, in-plane GRAPPA R=2, echo-spacing=10.6ms, turbo factor=21, 8 echo-trains per slice (ETPS).
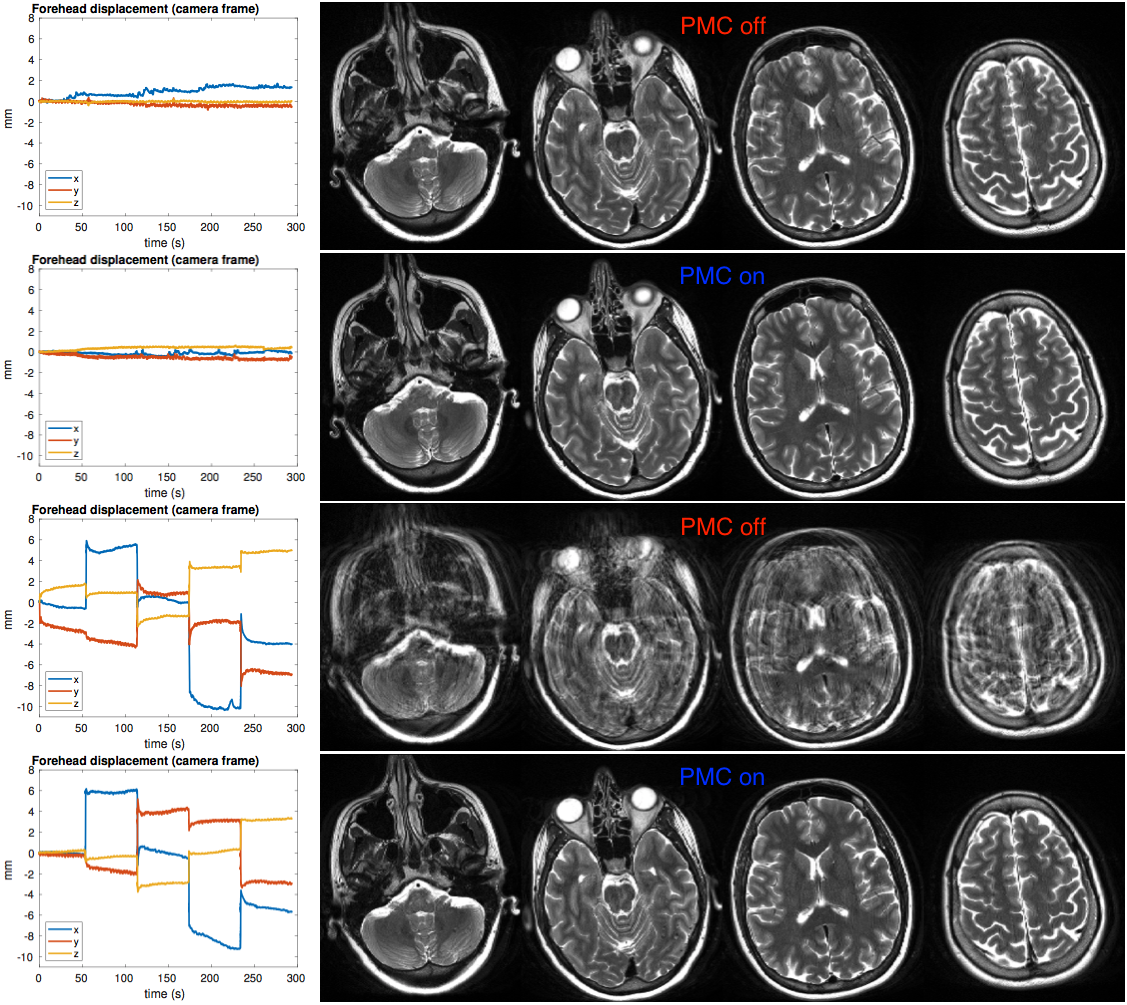
4:55min “T2” protocol: TR=11.75s, TE=93ms, FOV=200x162.6mm2, matrix=512x358, 60 axial 2.5mm slices, in-plane GRAPPA R=2, echo-spacing=9.31ms, turbo factor=13, 12 ETPS, 2 averages.
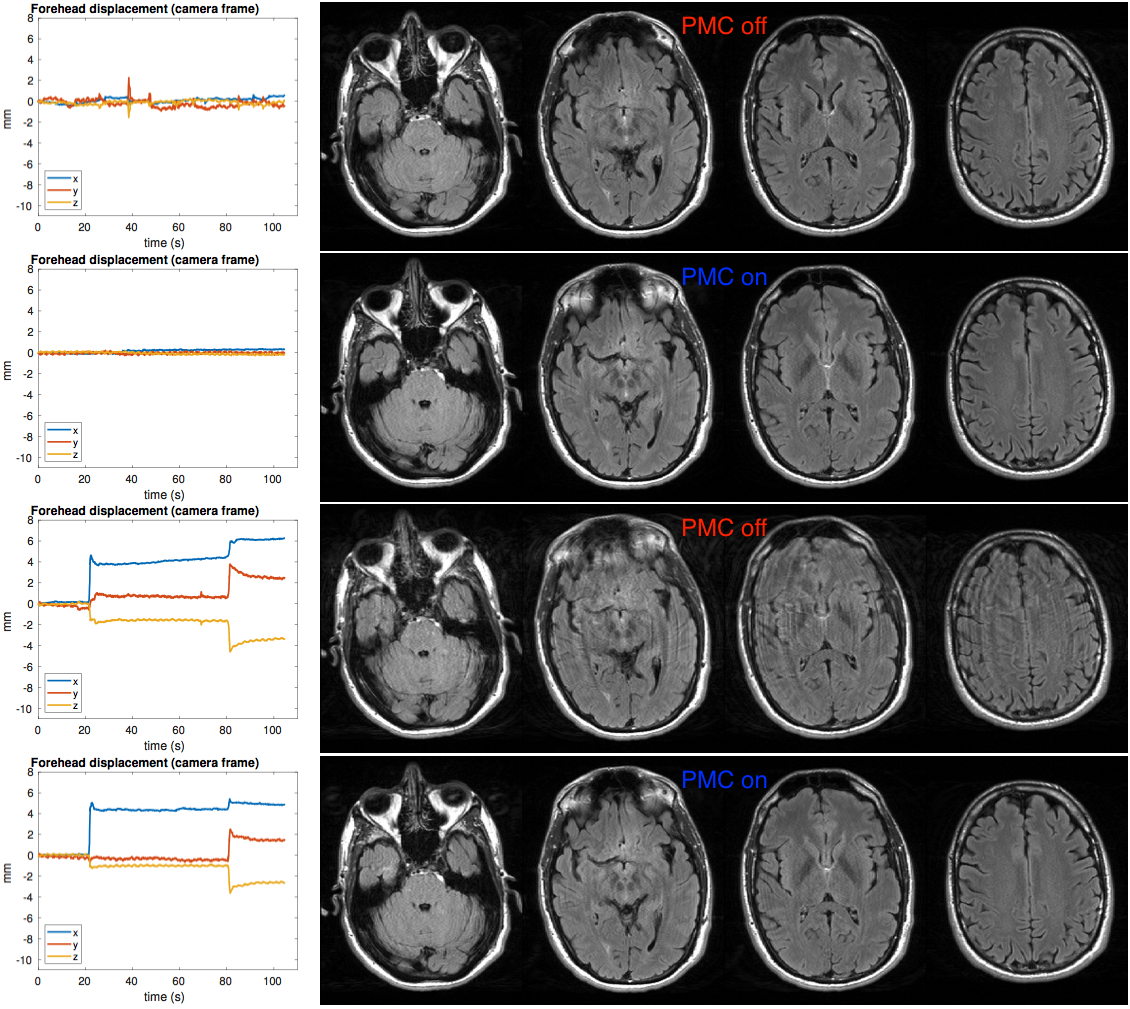
1:50min “FLAIR” protocol with 2 concatenations for odd/even slices: TI=2.5s, TR=9s, TE=85ms, FOV=220x178.9mm2, matrix=256x192, 36 axial 3mm slices, in-plane GRAPPA R=3, echo-spacing=8.5ms, turbo factor=16, 5 ETPS.
Five healthy subjects were scanned in accordance with Institutional Review Board guidelines. PMC was tested by prompting subjects to repeat similar motion in scans with PMC off and on. There was approximately one change in head position per minute, hence there were 1, 2 and 4 movements during the T2-fast, FLAIR, and T2 protocols, respectively. A subset of the T2-fast, T2, and FLAIR experiments was performed in each subject, with all three acquired with subject 5. For each protocol, two scans without intentional movement were acquired with PMC off and on. Movement instruction times:
- T2-fast: 45s of scan remaining (moving “right” and “up” tested separately)
- FLAIR: 1:25min and 25s of scan remaining (moving “right” then “up”)
- T2: 4, 3, 2, and 1min of scan remaining (moving “right”, “up”, “left”, “down”)
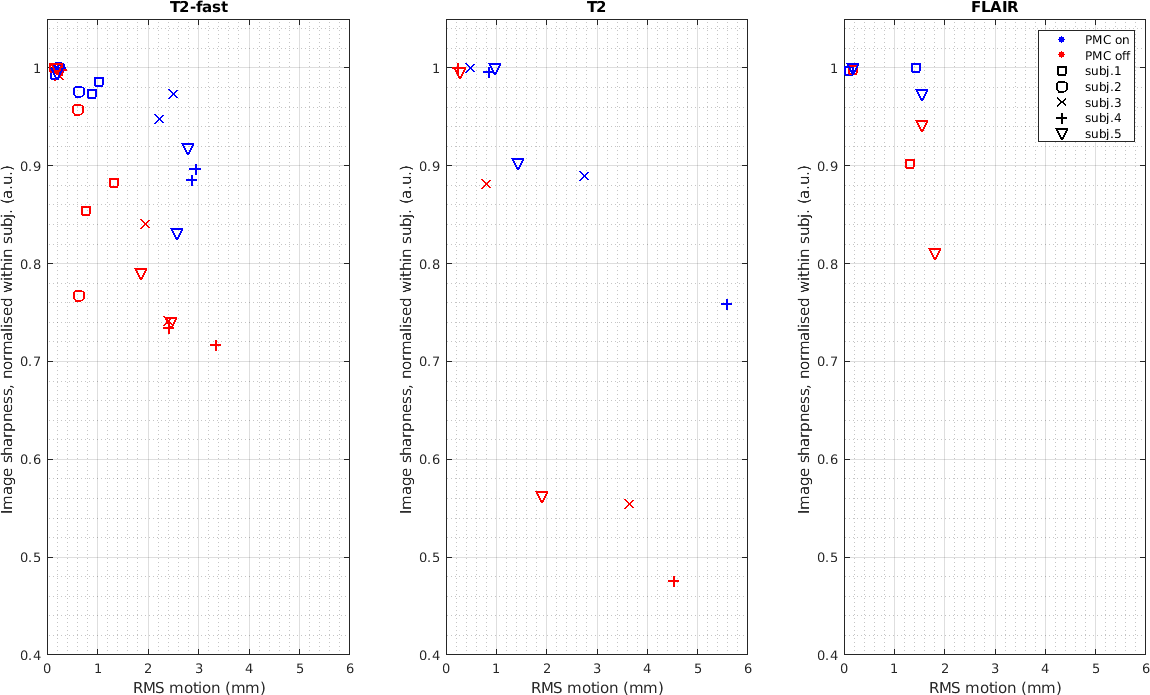
Image sharpness was estimated in each slice using the Tenengrad metric7 and the mean over all slices was computed. In a group of motion scans for each subject with a particular scan (T2-fast, T2, or FLAIR), the maximum sharpness was used to calculate the normalized sharpness in the remaining scans. The RMS deviation of the head8 relative to the start of the scan and time-averaged over the scan was calculated from the tracking data for all scans.
Results
Examples of image quality improvements with PMC in the presence of motion during T2-fast, T2 and FLAIR are shown in Figs. 2-4, respectively. Normalized image sharpness is plotted versus RMS motion relative to the start of the scan in Fig. 5 showing that the sharpness was always improved in scans with PMC.Discussion
The markerless PMC substantially improved in vivo image quality in these clinical protocols during the discrete motion experiments. Good image quality could be recovered with PMC in cases with severe artefacts in the equivalent PMC off scan. Even the 1:16 min T2 protocol was found to be sensitive to one change in head position. PMC applied before the acquisition of each slice appeared to be relatively successful and attempting correction within the echo-trains was not attempted given that the RARE echo-trains lasting 100-200ms are on the order of the ~33ms markerless tracking interval. Modest reacquisition may be helpful to correct some artefacts caused by motion during echo-trains.Conclusion
Markerless real-time motion correction using tracking of the subject’s face is a promising approach to reduce artefacts in clinical MRI.Acknowledgements
We are grateful for technical support from TracInnovations and the following funding sources: NICHD R01HD093578, NICHD R01HD085813, NIMH R44MH086984, NIDA U24DA041123, NIA R21AG046657, NICHD R01HD071664, NINDS R44NS083101, NCI R42CA183150, NICHD R00HD074649.References
1. Andre JB, Bresnahan BW, Mossa-Basha M, Hoff MN, Smith CP, Anzai Y, Cohen WA. Toward Quantifying the Prevalence, Severity, and Cost Associated With Patient Motion During Clinical MR Examinations. J Am Coll Radiol 2015;12:689–695.
2. Olesen OV, Sullivan JM, Mulnix T, Paulsen RR, Hojgaard L, Roed B, Carson RE, Morris ED, Larsen R. List-mode PET motion correction using markerless head tracking: proof-of-concept with scans of human subject. IEEE Trans Med Imaging 2013;32:200–209.
3. Olesen OV, Wilm J, van der Kouwe A, Jensen RR, Larsen R, Wald LL. An MRI compatible surface scanner. In: Proceedings of the 22nd Annual Meeting of ISMRM, 2014 (abstract 1303).
4. Benjaminsen C, Jensen RR, Wighton P, Tisdall MD, Johannesen HH, Law I, van der Kouwe AJW, Olesen OV. Real time MRI motion correction with markerless tracking. In: Proceedings of the 24th Annual Meeting of ISMRM, 2016 (abstract 1860).
5. Frost R, Wighton P, Karahanoglu FI, Robertson RL, Grant PE, Fischl B, Tisdall MD, van der Kouwe AJW. Markerless real-time motion correction for T1- and T2-weighted neuroanatomical MRI. In: Proceedings of the 26th Annual Meeting of ISMRM, 2018 (abstract 1167).
6. Hennig J, Nauerth A, Friedburg H. RARE imaging: a fast imaging method for clinical MR. Magn Reson Med 1986;3:823–833.
7. Krotkov E. Focusing. International Journal of Computer Vision 1988;1:223–237.
8. Reuter M, Tisdall MD, Qureshi A, Buckner RL, van der Kouwe AJW, Fischl B. Head motion during MRI acquisition reduces gray matter volume and thickness estimates. Neuroimage 2015;107:107–115.
Figures