4411
Effects of acquisition and compressed sensing reconstruction parameters on 3D-QALAS multi-parameter quantitation and synthetic imaging of the brain1Department of Imaging Physics, The University of Texas M.D. Anderson Cancer Center, Houston, TX, United States, 2SyntheticMR, Linkoping, Sweden, 3GE Healthcare, Waukesha, WI, United States, 4Department of Radiology, The University of Texas M.D. Anderson Cancer Center, Houston, TX, United States
Synopsis
3D QALAS is a promising new technique that simultaneously maps T1, T2, and PD in a single 3D acquisition. We investigate the robustness of this technique to several acquisition and compressed sensing reconstruction parameters in phantom and brain images. Parameter maps were shown to be robust to B1 through the center portion of the slab, while compressed sensing did not demonstrate any effects on parameters in phantom or cause additional artifacts on parameter maps in human brain. 3D QALAS thus presents an attractive quantification method for therapy planning and tissue volume measurement applications.
Introduction
The introduction of SyMRI and MAGIC [1] has enabled rapid multi-parameter mapping and synthetic imaging for clinical use. 3D QALAS [2,3] (3D-quantification using an interleaved Look-Locker acquisition sequence with T2 preparation pulse) is a more recent development that potentially provides similar capability in a fast 3D acquisition, enabling isotropic imaging with smaller voxel sizes. This technique relies on the use of T2 and inversion preparation pulses interleaved with segmented gradient echo readouts for parameter fitting. While the use of low flip angles reduces the need for explicit system B1 corrections, the imperfect slab profile may still affect parameter quantification. And while the multiple phases and 3D acquisition geometry lends itself to compressed sensing (CS) techniques for acceleration, the effects of reconstruction on quantification have not been explored for this technique. This study examines the influence of slab selection, inversion times, and reconstruction parameters on quantitation in a phantom and human subjects.Methods
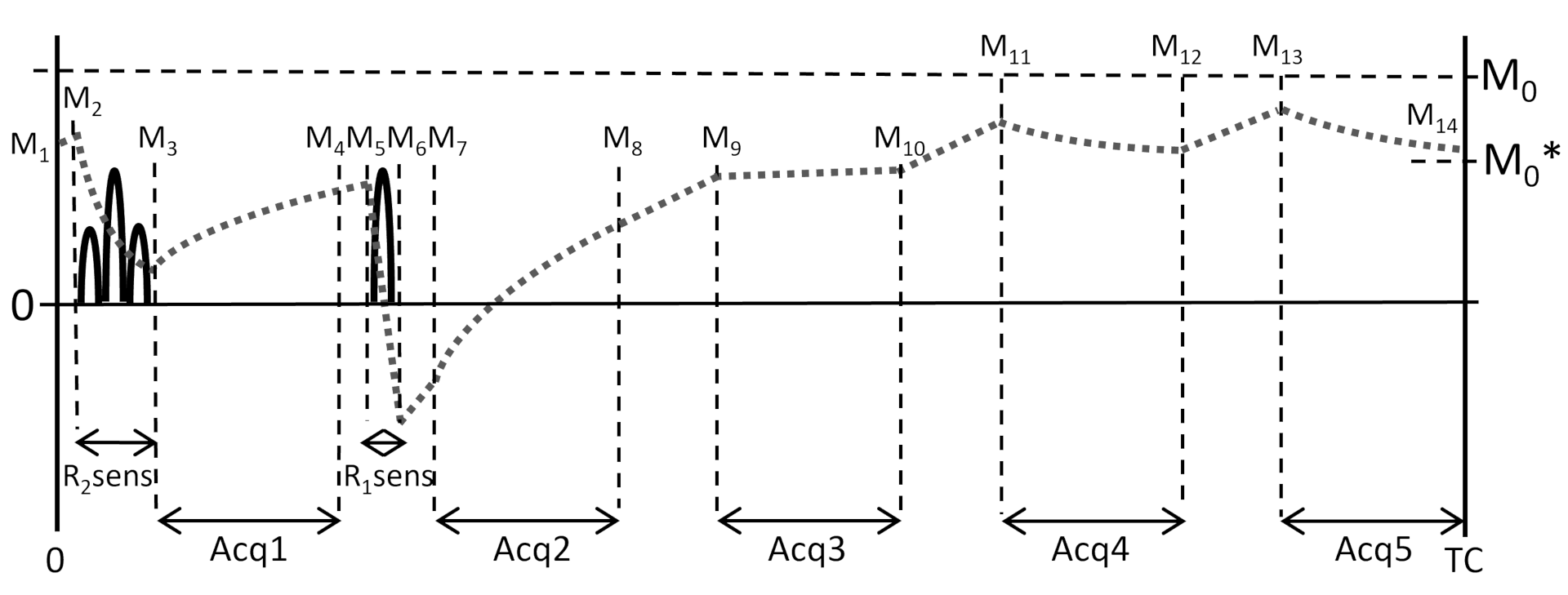
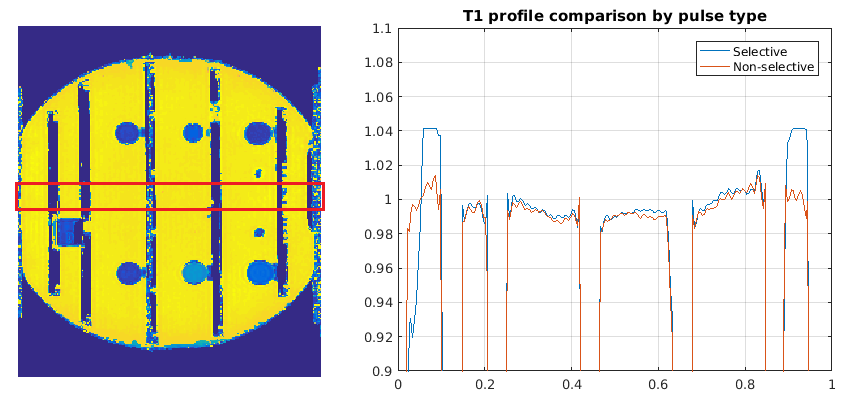
The 3D QALAS sequence was implemented for non-triggered acquisitions in the head and body. This sequence consists of 5 phases of varying contrasts acquired with 3D gradient echo readouts in a single cycled acquisition. A T2 prep pulse precedes the first phase, followed by an inversion T1 prep pulse and 4 delayed phases (figure 1). One cycle would acquire one segment of Cartesian k-space for each of the 5 phases with spoiled gradient echo readouts, such that repeating the cycle would fill all segments of k-space for 5 image sets. The sequence timing was arranged such that the 5 phases of the acquisition were equally spaced in time at 0.87-1.0 sec, mimicking a triggered cardiac acquisition. 3D QALAS data was acquired of the ISMRM NIST system phantom (Model 130, QalibreMD, Boulder, CO) in a 3T scanner (MR750, GE Healthcare, Waukesha, WI). Sequence parameters were: FOV = 24.0 cm, matrix = 224x224, slice locations = 128, thickness = 1.6mm, flip = 4, views per segment=100, acquisition spacing = 1.0 sec. Sequence was repeated with two inversion delay times of 30 and 100 msec, and with slab selective and nonselective pulses. Poisson disk undersampling and CS reconstructions were performed using the Berkeley Advanced Reconstruction Toolbox (BART, The University of California, Berkeley, CA), with L1 wavelet and TV regularization functions employing joint sparsity over coils as well as the multiple acquisitions of the sequence. Quantitative T1, T2, and PD maps were reconstructed from both acquisitions using a research version of SyMRI (SyntheticMR, Linkoping, Sweden). Human volunteer images were also acquired and reconstructed with similar parameters. On the parameter maps of the phantom images, profiles along the slab selection direction were measured across a homogeneous section of the phantom and smoothed to suppress Gibbs ringing. Mean values were recorded of ROI’s drawn in the T1 and T2 compartments of the phantom. CS reconstructed images were observed for sharpness and artifacts.Results
With the non-selective pulse, T1 variation was within +/- 1.7% across the entire profile. The same variation was observed within the center 70% of the slab selective pulse, with an upward trend towards a maximum of 4.1% at the edges of the profile. Accuracy of T1 measurements was within 3.4% in T1 compartments ranging from 497 to 984 msec. In phantoms, CS reconstructions caused no observable deviation in T1 values for overall acceleration factors of 2.15 and 2.87 relative to full elliptical k-space sampling.Discussion and Conclusion
The effects of B1 were relatively small over the entire brain volume, as also observed by other groups using modeled 3D techniques [4]. Thus the technique does not require correction for much of the center portion of the slab, though slight T1 overestimation was observed in approximately the outer 10% of each side of the slab. It should be noted that the main compartment of the phantom consists of water, and the acquisition was not optimized for relaxation values that much longer than brain tissues. The shorter inversion delay time increases dynamic range of the T1 recovery curve, improving the accuracy of model fitting. CS reconstruction is not expected to influence fitted spin parameters in a phantom with large compartments. While CS could impact the appearance of structures in human images, fitted quantitation maps did not demonstrate additional artifacts or smoothing effects compared to the CS reconstructed base images. Thus quantification appears robust to variations in acquisition and reconstruction protocol, which may occur when adapted for different geometries or scan times. 3D QALAS with compressed sensing is shown to be a robust technique for multiplanar diagnosis, as well as for therapy planning and tissue volume segmentation applications.Acknowledgements
Research support was provided in part by GE Healthcare.References
1. Warntjes JB, Leinhard OD, West J, Lundberg P. Rapid magnetic resonance quantification on the brain: Optimization for clinical usage. Magn Reson Med. 2008 ; 60:320-9
2. Kvernby S, Warntjes MJ, Haraldsson H, Carlhäll CJ, Engvall J, Ebbers T. Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS. J Cardiovasc Magn Reson. 2014; 16:102
3. Hwang KP, Banerjee S, Zhang T, Wanrtjes M. 3D isotropic multi-parameter mapping and synthetic imaging of the brain with 3D-QALAS: comparison with 2D MAGIC. Proc ISMRM, #5627.
4. Tamir JI, Uecker M, Chen W, Lai P, Alley MT, Vasanawala SS, Lustig M. T2 shuffling: Sharp, multicontrast, volumetric fast spin-echo imaging. Magn Reson Med. 2017; 77:180-195.
Figures