4396
Free-Breathing 3D T1 Mapping of the Whole-Heart Using Low-Rank Tensor Modeling1Gordon Center for Medical Imaging, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States
Synopsis
T1 of the myocardium is an emerging quantitative biomarker for a variety of heart diseases. However,
Introduction
Myocardium T1 is an emerging quantitative biomarker for a variety of heart diseases, including infiltration, acute myocardial injury, and fibrosis1. Quantification of T1 over the entire myocardium is desirable for complete assessment and diagnosis of the heart, however, T1 mapping is challenging in the heart due to cardiac and respiratory motion. To overcome this issue, methods have been developed combining inversion2-11, saturation13-20, variable-flip-angle21 or signal-model22 based methods with electrocardiography (ECG) trigger-controlled single/multi-slice 2D2-4,11-16 or single-shot/segmented 3D5,9,10,17-22 acquisitions over breath-hold2-5,9-16 or with respiratory control using bellow/navigators for free-breathing acquisition17-22. Recently, low-rank tensor-based approaches have been proposed for MR to exploit correlations in high-dimensional data and enable image reconstruction at high acceleration factors23-26. Promising results have been demonstrated in various applications27-33 including quantitative cardiovascular imaging32,33. This work presents a low-rank tensor-based data acquisition and processing method to enable free-breathing 3D T1 mapping of the whole-heart.Methods
Low-Rank Tensor Modeling
We propose to model the image function $$$\rho(x,t_1,t_2)$$$ as high-order partially-separable (PS) functions (Figure 1)23,24,33:$$\rho(x,t_1,t_2)=\sum_{l=1}^L\sum_{m=1}^M\sum_{n=1}^Nc_{l,m,n}\theta_l(x)\phi_m(t_1)\psi_n(t_2)\space\space\space\space\space\space\space\space\space\space(1)$$ where $$$x$$$ denotes the spatial dimension, $$$t_1$$$ denotes the respiratory motion phase, $$$t_2$$$ denotes the inversion-recovery (IR) time, $$$\left\{\theta_l(x)\right\}_{l=1}^L$$$, $$$\left\{\phi_m(t_1)\right\}_{m=1}^M$$$ and $$$\left\{\psi_n(t_2)\right\}_{n=1}^N$$$ denotes the spatial, respiratory, and T1 recovery basis functions, respectively, $$$L$$$, $$$M$$$, and $$$N$$$ denotes the tensor rank, and $$$c_{l,m,n}$$$ denotes the core-tensor coefficients. The proposed model indicates that the high-dimensional imaging function resides in a low-dimensional subspace and thus can be recovered even from a highly under-sampled data. To ensure sufficient number of measurements are sampled for image reconstruction, we propose to fully-sample a limited number of locations at the k-space center and sparsely-sample all the other locations to provide extensive k-space coverage over the entire $$$(k,t_1,t_2)$$$-space (Figure 2). Note that the proposed model allows to reconstruct the image function (i) at different respiratory motion phases without involving any binning or image registration, and (ii) at each different IR times resulting from the natural variations in the heart-rate over time.
Reconstruction
With known respiratory and T1 recovery basis functions (denoted as $$$\left\{\hat{\phi}_m(t_1)\right\}_{m=1}^M$$$ and $$$\left\{\hat{\psi}_n(t_2)\right\}_{n=1}^N$$$), $$$\left\{c_{l,m,n}\right\}_{l,m,n=1}^{L,M,N}$$$ and $$$\left\{\theta_l(x)\right\}_{l=1}^L$$$ can be estimated by solving the following optimization problem:$${arg\min_{c_{l,m,n},\theta_l(x)}}\parallel{d(k,t_1,t_2)-\Omega F_s\left\{\Sigma_{l=1}^L\Sigma_{m=1}^M\Sigma_{n=1}^Nc_{l,m,n}\theta_l(x)\hat{\phi}_m(t_1)\hat{\psi}_n(t_2)\right\}}\parallel_2^2+R_1(vec\left\{c_{l,m,n}\right\})+R_2\left\{\theta_l(x)\right\}\space\space\space\space\space\space\space\space\space\space(2)$$where $$$d(k,t_1,t_2)$$$ denotes the sparsely-sampled k-space measurement, $$$\Omega$$$ denotes the sampling matrix, and $$$F_s$$$ denotes the spatial Fourier transform matrix. The optimization problem in Eq.(2) can be solved using alternating minimization algorithms with verified convergence property24.
In this work, the T1 recovery basis functions were estimated by performing singular value decomposition (SVD) on a dictionary of magnetization signal generated using Bloch equation simulation37 over the clock-time with a range of T1 (100 to 2000ms) and flip angle values (5 to 15$$$^\circ$$$) to account for the B1 inhomogeneity effect. The respiratory basis functions were estimated via a multi-step procedure. The proposed model in Eq.(1) was first reduced to a PS model ($$$\rho(x,t)$$$, where $$$t$$$ denotes clock-time)23,24,34,35 and underwent a preliminary low-rank-based PS reconstruction35. Afterwards, the clock-time ($$$t$$$) was correlated with the respiratory motion phase ($$$t_1$$$) based on the liver motion in the reconstructed image. The respiratory basis functions were then estimated by performing SVD on the spatial-respiratory motion phase dataset $$$\rho(x,t_1)$$$ at a fixed IR time. Note that the proposed model is not limited to this approach of basis estimation. For example, the respiratory basis functions can also be estimated via alternating minimization with known $$$\left\{\hat{\psi}_n(t_2)\right\}_{n=1}^N$$$ and estimated temporal basis functions from the fully-sampled data acquired over the k-space center using the PS model23. Lastly, regularizations exploiting sparsity and spatial-temporal frequency sparsity was used for $$$R_1(\cdot)$$$ and for $$$R_2(\cdot)$$$, respectively.
Results
All experiments were performed on a whole-body MR scanner. One healthy volunteer was imaged under a study protocol approved by the Institutional Review Board (IRB). Acquisitions were performed using an IR-FLASH sequence at the end-diastole with ECG-triggering. Non-selective inversion pulses were inserted every 4-cardiac-cycles with alternating inversion-time delays of 100 and 200ms. The imaging parameters were: FOV=360$$$\times$$$304$$$\times$$$144mm3, matrix size=192$$$\times$$$162$$$\times$$$24, TR/TE=4/2ms, flip-angle=10$$$^\circ$$$, PE lines sampled per cardiac-cycle=54 (in which 10 lines were fully-sampled at the center of k-space), total acquisition time=10min. for heart-rate of 80bpm. For comparison, T1 map of a single 2D slice was acquired using MOLLI2,3. T1 was estimated for each voxel via least-square fitting using variable-projection-algorithm36 and Look-Locker equation for MOLLI37 and Bloch equation simulation for our proposed method.
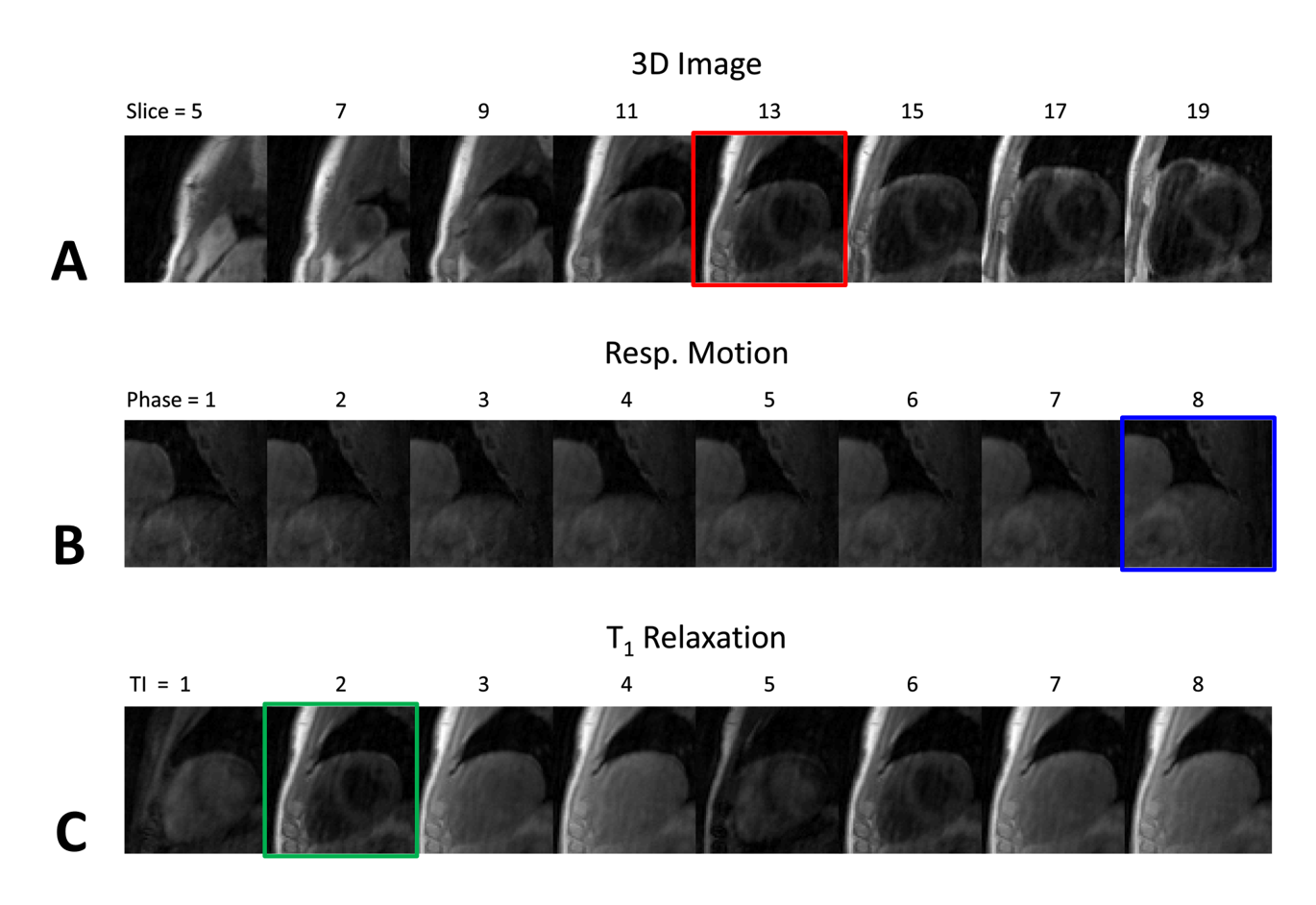
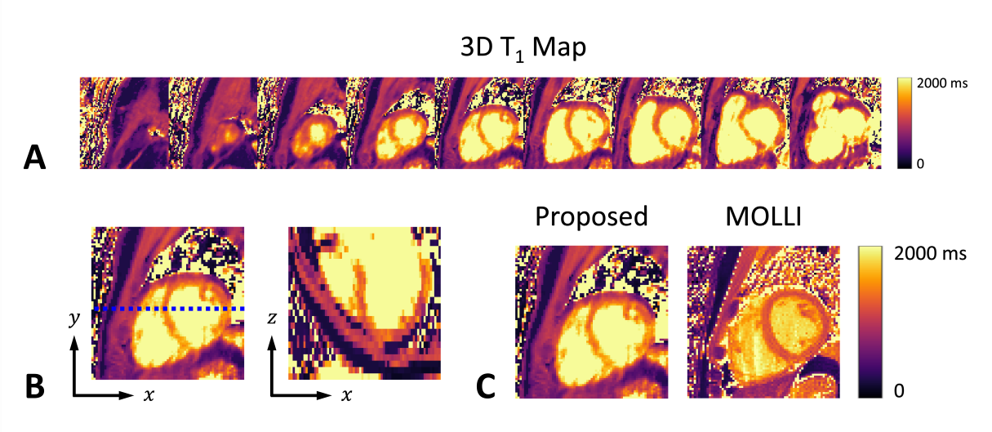
Overall, the proposed approach successfully reconstructed the 3D image including the whole-heart over different respiratory motion phases and IR times (Figures 3 and 5). Estimation of T1 over the whole-heart was also feasible using the proposed method, with mean myocardium T1 values similar to those from 2D MOLLI (Figure 4).
Conclusion
Free-breathing 3D T1 mapping of the whole-heart can be achieved by low-rank tensor modeling. The proposed method can enable new clinical applications of T1 mapping in cardiac MR imaging.Acknowledgements
This work was partially supported by the National Institutes of Health (P41EB022544, R01CA165221, R01HL137230, R01HL118261, and T32EB013180).References
1. Messroghli DR et al. "Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI)." Journal of Cardiovascular Magnetic Resonance 19.1 (2017): 75.
2. Messroghli DR et al. "Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 52.1 (2004): 141-146.
3. Piechnik SK et al. "Shortened Modified Look-Locker Inversion recovery (ShMOLLI) for clinical myocardial T1-mapping at 1.5 and 3 T within a 9 heartbeat breathhold." Journal of cardiovascular magnetic resonance 12.1 (2010): 69.
4. Coniglio A et al. "Multiple 3D inversion recovery imaging for volume T1 mapping of the heart." Magnetic resonance in medicine 69.1 (2013): 163-170.
5. Kvernby S et al. "Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS." Journal of Cardiovascular Magnetic Resonance 16.1 (2014): 102.
6. Mehta BB et al. "Accelerated and navigator-gated look-locker imaging for cardiac t1 estimation (ANGIE): Development and application to T1 mapping of the right ventricle." Magnetic resonance in medicine 73.1 (2015): 150-160.
7. Weingärtner S et al. "Free-breathing multislice native myocardial T1 mapping using the slice-interleaved T1 (STONE) sequence." Magnetic resonance in medicine 74.1 (2015): 115-124.
8. Weingärtner S et al. "Free-breathing post-contrast three-dimensional T1 mapping: volumetric assessment of myocardial T1 values." Magnetic resonance in medicine 73.1 (2015): 214-222.
9. Weingärtner S et al. "Simultaneous multislice imaging for native myocardial T1 mapping: Improved spatial coverage in a single breath-hold." Magnetic resonance in medicine 78.2 (2017): 462-471.
10. Chen Y et al. "Single breath-hold 3D cardiac T1 mapping using through-time spiral GRAPPA." NMR in Biomedicine 31.6 (2018): e3923.
11. Becker KM et al. "Simultaneous high-resolution cardiac T1 mapping and cine imaging using model-based iterative image reconstruction." Magnetic resonance in medicine (2018).
12. Marty B et al. "Fast, precise, and accurate myocardial T1 mapping using a radial MOLLI sequence with FLASH readout." Magnetic resonance in medicine 79.3 (2018): 1387-1398.
13. Chow K et al. "Saturation recovery single-shot acquisition (SASHA) for myocardial T1 mapping." Magnetic resonance in medicine 71.6 (2014): 2082-2095.
14. Higgins DM et al. "T1 measurement using a short acquisition period for quantitative cardiac applications." Medical physics 32.6Part1 (2005): 1738-1746.
15. Fitts M et al. "Arrhythmia insensitive rapid cardiac T1 mapping pulse sequence." Magnetic resonance in medicine70.5 (2013): 1274-1282.
16. Weingärtner S et al. "Combined saturation/inversion recovery sequences for improved evaluation of scar and diffuse fibrosis in patients with arrhythmia or heart rate variability." Magnetic resonance in medicine 71.3 (2014): 1024-1034.
17. Weingärtner S et al. "Free-breathing combined three-dimensional phase sensitive late gadolinium enhancement and T1 mapping for myocardial tissue characterization." Magnetic resonance in medicine 74.4 (2015): 1032-1041.
18. Nordio G et al. "3D myocardial T1 mapping using saturation recovery." Journal of Magnetic Resonance Imaging46.1 (2017): 218-227.
19. Guo R et al. "Three-dimensional free breathing whole heart cardiovascular magnetic resonance T 1 mapping at 3 T." Journal of Cardiovascular Magnetic Resonance 20.1 (2018): 64.
20. Nordio G et al. "3D SASHA myocardial T1 mapping with high accuracy and improved precision." Magnetic Resonance Materials in Physics, Biology and Medicine (2018): 1-9.
21. Clique H et al. "3D myocardial T1 mapping at 3T using variable flip angle method: pilot study." Magnetic resonance in medicine 71.2 (2014): 823-829.
22. Hu C et al. "T1-refBlochi: high resolution 3D post-contrast T1 myocardial mapping based on a single 3D late gadolinium enhancement volume, Bloch equations, and a reference T1." Journal of Cardiovascular Magnetic Resonance19.1 (2017): 63.
23. Liang ZP. "Spatiotemporal imaging with partially separable functions." Biomedical Imaging: From Nano to Macro, 2007. ISBI 2007. 4th IEEE International Symposium on. IEEE, 2007.
24. J. He et al. "Accelerated High-Dimensional MR Imaging With Sparse Sampling Using Low-Rank Tensors," IEEE transactions on medical imaging, vol. 35, pp. 2119-29, Sep 2016.
25. Trzasko JD and Manduca A. "A unified tensor regression framework for calibrationless dynamic, multi-channel MRI reconstruction." Proceedings of the 21st Annual Meeting of ISMRM, Salt Lake City, Utah, USA. Vol. 603. 2013.
26. Yu Y et al. "Multidimensional compressed sensing MRI using tensor decomposition-based sparsifying transform." PloS one 9.6 (2014): e98441.
27. Christodoulou AG et al. "Fast dynamic electron paramagnetic resonance (EPR) oxygen imaging using low-rank tensors." Journal of Magnetic Resonance 270 (2016): 176-182.
28. Ma C et al. "High-resolution dynamic 31P-MRSI using a low-rank tensor model." Magnetic resonance in medicine 78.2 (2017): 419-428.
29. Ramb R et al. "Low-rank plus sparse tensor reconstruction for high-dimensional cardiac MRI." Proc. ISMRM. Vol. 1199. 2017.
30. Liu L et al. "Accelerated high b-value diffusion-weighted MR imaging via phase-constrained low-rank tensor model." Biomedical Imaging (ISBI 2018), 2018 IEEE 15th International Symposium on. IEEE, 2018.
31. Wang N et al. "Quantitative 3D dynamic contrast-enhanced (DCE) MR imaging of carotid vessel wall by fast T1 mapping using Multitasking." Magnetic Resonance in Medicine (2018).
32. Christodoulou AG and Liang ZP. "3D dynamic T1 mapping of the myocardium using a time-varying subspace." Proc. Int. Soc. Magn. Reson. Med. 2015.
33. Christodoulou AG et al. "Magnetic resonance multitasking for motion-resolved quantitative cardiovascular imaging." Nature Biomedical Engineering 2.4 (2018): 215.
34. Haldar, Justin P., and Zhi-Pei Liang. "Spatiotemporal imaging with partially separable functions: A matrix recovery approach." Biomedical Imaging: From Nano to Macro, 2010 IEEE International Symposium on. IEEE, 2010.
35. Zhao B et al. "Image reconstruction from highly undersampled-space data with joint partial separability and sparsity constraints." IEEE transactions on medical imaging 31.9 (2012): 1809-1820.
36. Golub, Gene et al. "Separable nonlinear least squares: the variable projection method and its applications." Inverse Problems 19.2 (2003): R1.
37. Deichmann, R. et al. "Quantification of T 1 values by SNAPSHOT-FLASH NMR imaging." Journal of Magnetic Resonance 96.3 (1992): 608-612.
Figures
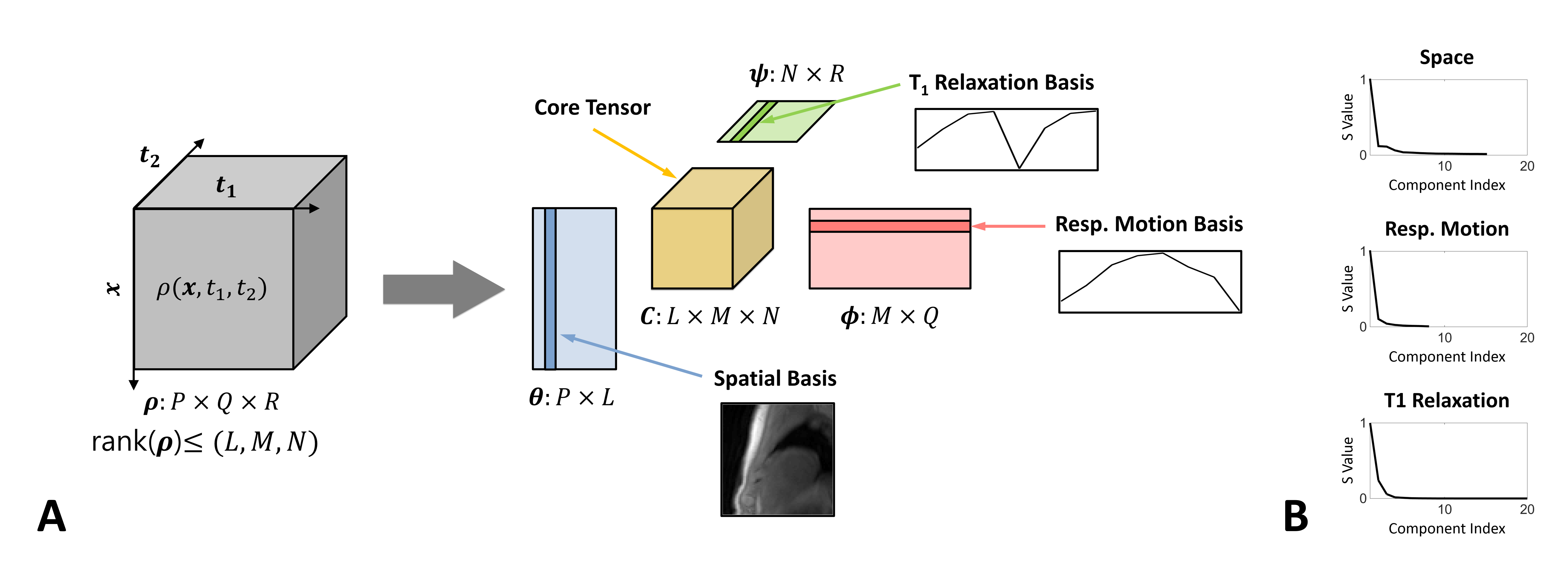
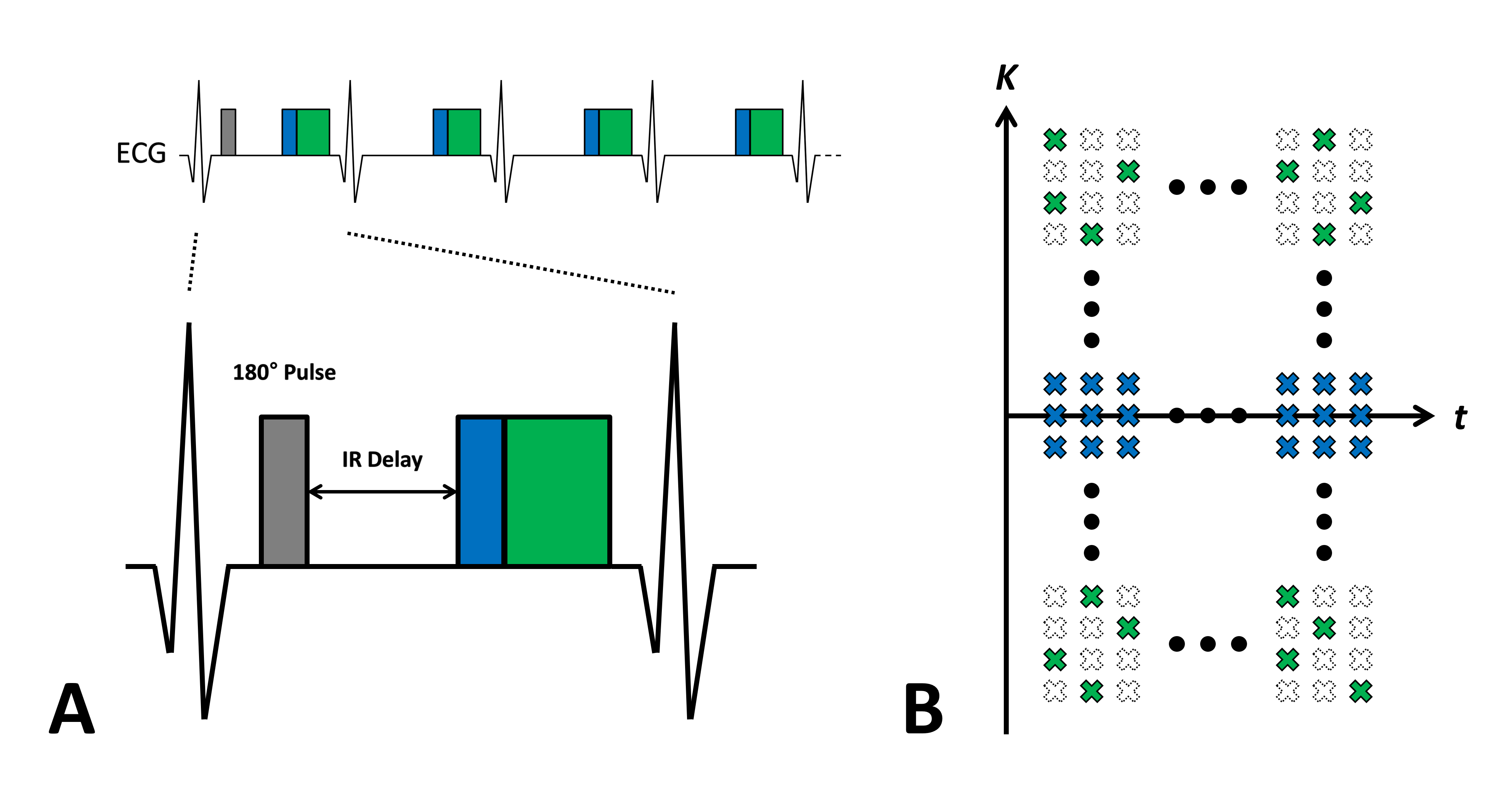
Figure 2. Illustration of the acquisition scheme. A: Schematic diagram of acquisition. A non-selective 180° inversion pulse is inserted for T1 relaxation and data acquisition is performed at end-diastole with ECG triggering. B: Schematic diagram of data-sampling. A limited number of k-space locations at the k-space center (blue) are fully-sampled over the entire cardiac-cycle, whereas all the other k-space locations (green) are sparsely-sampled to provide extensive k-space coverage over the entire (k,t1,t2)-space and to ensure a sufficient number of measurements are sampled for reconstruction.