4385
Toward 3D Free-breathing Cardiac Magnetic Resonance Fingerprinting1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Philips Healthcare, Guildford, United Kingdom
Synopsis
Magnetic Resonance Fingerprinting (MRF) has been introduced to simultaneously estimate multiple quantitative parameters but mainly applied to static organs. Recently the feasibility of 2D triggered cardiac MRF (cMRF) under breath-hold has been demonstrated and provides single slice simultaneous T1 and T2 maps. However, 2D cMRF provides insufficient coverage of the heart. Here we sought to develop a free-breathing 3D triggered cMRF sequence. Respiratory bellows drive an autofocus algorithm that is used to perform translation correction of respiratory motion followed by a low rank MRF reconstruction. The proposed 3D cMRF approach was evaluated in three healthy subjects, demonstrating considerable improvements in parametric maps when compared to no motion correction.
INTRODUCTION:
Magnetic Resonance Fingerprinting (MRF) offers the possibility of estimating multiple parametric maps from a transient state acquisition1. 2D triggered cardiac MRF2 (cMRF) has been proposed to enable simultaneous T1 and T2 myocardial tissue characterization from a single breath-hold acquisition. 2D cMRF relies on variable preparation pulses (inversion recovery and T2 preparation) in different heartbeats to achieve the required T1 and T2 encoding. However, 2D cMRF provides insufficient heart coverage and requires acquisition under breath-hold, which can be challenging in some patients. Here we sought to develop a free-breathing 3D triggered cMRF sequence. Respiratory motion can lead to errors in parametric maps3-5. In response, respiratory bellows are employed to drive a localized autofocus6-7 algorithm and correct for global translational motion. Translationally corrected k-space is reconstructed with a low rank inversion (LRI)8-10 reconstruction with locally low rank regularization (LLR)11-12. The proposed 3D cMRF approach was tested in three healthy subjects and compared to no motion correction.METHODS:
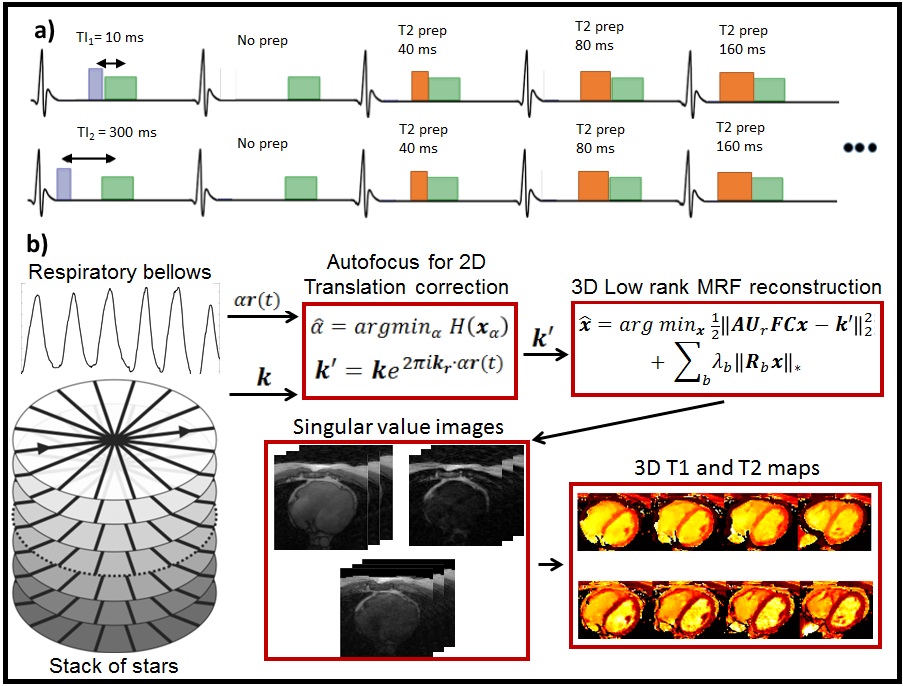
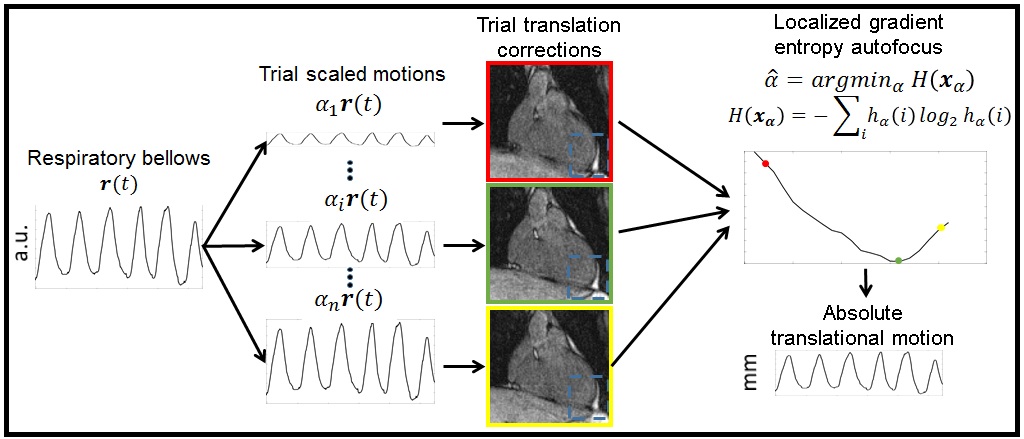
The proposed 3D cMRF framework acquires data with varying preparation pulses under free-breathing and ECG triggering, using a golden radial stack of stars trajectory (Fig.1). Respiratory bellows are employed, yielding a 1D (relative) respiratory signal $$$\boldsymbol{r(t)}$$$. The bellows signal is assumed to be the correct respiratory signal, up to a scaling factor. We propose to find this scaling factor along each spatial dimension via localized autofocus7. A trial of motion scaled signals $$$\boldsymbol{\alpha r(t)}$$$ is used to translationally correct k-space, building a bank of translationally corrected images using all acquired data. A region of interest is manually selected and localized gradient entropy metric $$$\boldsymbol{H}$$$ is used to determine the correct translational motion scale: $$$\boldsymbol{\hat{\alpha}=argmin_{\alpha}H(x_{\alpha})}$$$, where $$$\boldsymbol{x_{\alpha}}$$$ is the image translationally corrected by $$$\boldsymbol{\alpha r(t)}$$$ and $$$\boldsymbol{H(x_\alpha)=-\sum_{i}h_{\alpha}(i)log_{2}h_{\alpha}(i)}$$$, where $$$\boldsymbol{h_\alpha}$$$ is a normalized image gradient (Fig.2). The optimal motion signal is determined by evaluating the localized gradient entropy for every value of $$$\boldsymbol{\alpha}$$$; the resulting motion is used for beat-to-beat translation correction. Translationally corrected k-space data is reconstructed with LLR-MRF11 by solving: $$$\boldsymbol{\hat{x}=argmin_{x}\frac{1}{2}||AU_{r}FCx-k'||_2^2+\sum_{b}\lambda_{b}||R_{b}x||_*}$$$, where $$$\boldsymbol{x}$$$ are singular images, $$$\boldsymbol{A}$$$, $$$\boldsymbol{U_r}$$$, $$$\boldsymbol{F}$$$ and $$$\boldsymbol{C}$$$ are sampling, compression (obtained from a truncated singular value decomposition of the MRF dictionary), Fourier and coil sensitivity operators, $$$\boldsymbol{k'}$$$ is the translational corrected k-space data, $$$\boldsymbol{R_b}$$$ is a reshaping operator for local image block b and $$$\boldsymbol{\lambda_b}$$$ is the corresponding regularization strength. Maps were generated matching the reconstructed singular images to the compressed dictionary in a voxel-by-voxel basis.EXPERIMENTS:
Three healthy subjects were scanned in a 1.5T Philips MR scanner; short axis orientation was used, two subjects were acquired with resolution 2x2x6mm3 and 10 slices, one subject was acquired with resolution 2x2x3.2mm3 and 26 slices. The 3D cMRF free-breathing acquisition was performed with the following parameters: TE/TR = 2.2/4.4 ms, linear flip angle from 5º to 30º, 1000 radial spokes per slice, 1 radial spoke per time-point. Data were reconstructed with and without the proposed motion correction strategy; 2D in-plane translation correction was used for 2x2x6mm3 data, 3D translation correction was used for 2x2x3.2mm3 data. LLR-MRF was used in both cases and solved with the Alternating Direction Method of Multipliers (ADMM). Motion estimation and reconstruction parameters were empirically set: $$$\boldsymbol{\alpha}$$$ was sampled from [0:0.1:2]x$$$\beta$$$ ($$$\beta$$$ being the expected motion amplitude in a given dimension), $$$\boldsymbol{H(x_\alpha)}$$$ computed for every case to determine the correct translation, global low rank r = 8, local low rank $$$\boldsymbol{\lambda_b}$$$ = 0.1$$$\boldsymbol{S_b^1}$$$ ($$$\boldsymbol{S_b^1}$$$ being the first singular value at local block b), block size = 7 and 5 ADMM iterations.RESULTS:
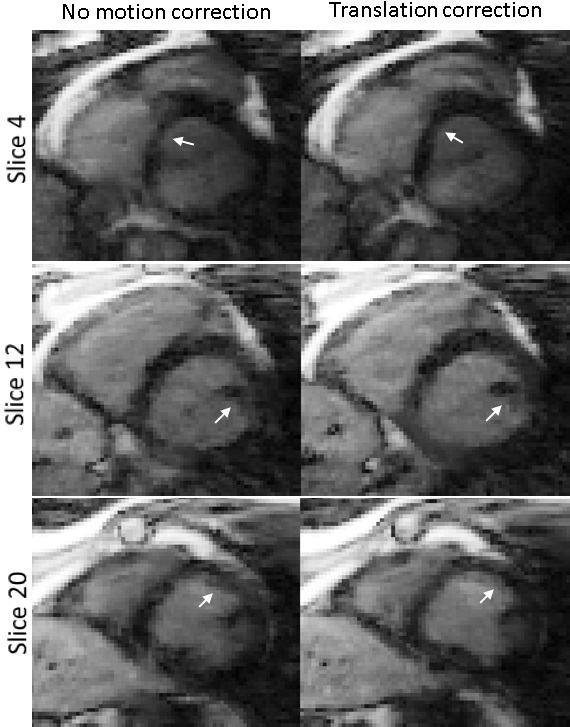
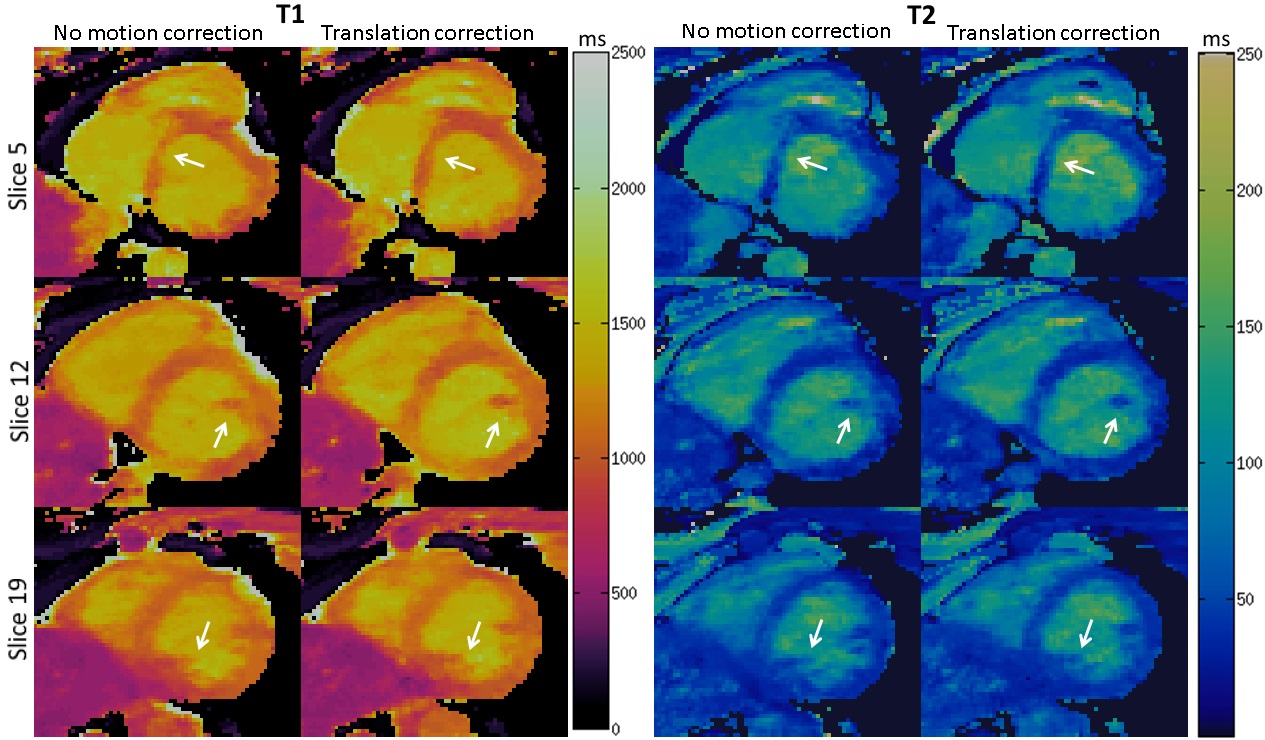
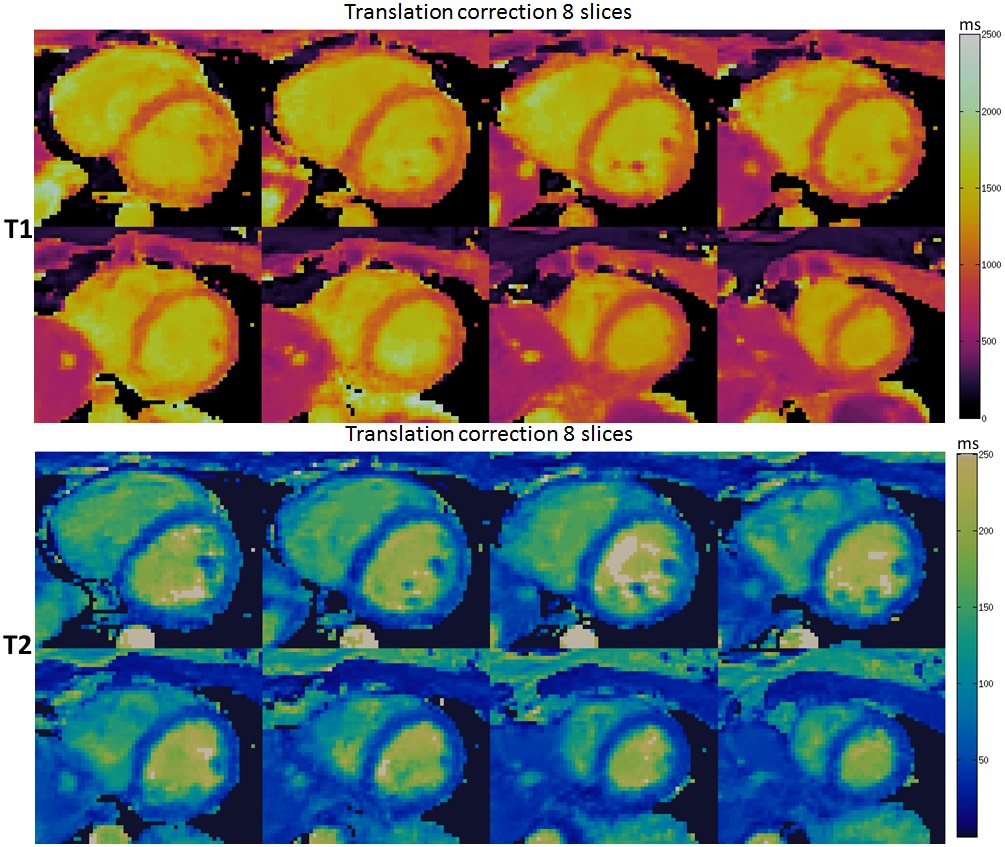
The proposed approach reduced respiratory motion artefacts, predominantly blurring, in the reconstructed singular images. This is shown for a 2x2x3.2mm3 healthy subject data in short-axis third singular images in Fig.3. Corresponding T1 and T2 maps show improved parametric map quality due to the reduction of respiratory motion artefacts (Fig.4). In the parametric maps, both ghosting and blurring artefacts are reduced, improving delineation of structures like papillary muscles. Parametric maps obtained with the proposed approach for a 2x2x6mm3 healthy subject data are shown in Fig.5 for 8 slices, showing consistent map quality throughout the 3D volume. T1 and T2 values measured in the septum for all subjects in maps with/without motion correction were: 988±20/1026±23ms and 46.8±3.2/48.3±3.6ms, respectively.CONCLUSION:
A novel approach for free-breathing 3D cardiac triggered MRF is proposed, based on respiratory bellows and localized autofocus to achieve global translation motion correction. Parametric map quality improves with the proposed approach; however residual motion artefacts remained after motion correction due to uncorrected non-rigid motion and spatially varying field inhomogeneities. Future work will explore more complex motion models and compare with conventional cardiac mapping methods.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/ A000049/1).References
1. Ma D, Gulani V, Seiberlich N, Liu K, Sunshine JL, Duerk JL, Griswold MA. Magnetic resonance fingerprinting. Nature 2013;495:187–192.
2. Hamilton JI, Jiang Y, Chen Y, et al. MR fingerprinting for rapid quantification of myocardial T 1 , T 2 , and proton spin density. MRM 2017;77:1446–1458.Mehta BB et al, MRM 2018;00:1-16
3. Mehta BB, Ma D, Pierre EY, Jiang Y, Coppo S, Griswold MA. Image reconstruction algorithm for motion insensitive MR Fingerprinting (MRF): MORF. MRM 2018;80:2485-2500.
4. Cruz G, Jaubert O, Schneider T, Botnar RM, Prieto C. Rigid motion-corrected magnetic resonance fingerprinting. MRM 2018;00:1-15.
5. Yu Z, Zhao T, Assländer J, Lattanzi R, Sodickson DK, Cloos MA. Exploring the sensitivity of magnetic resonance fingerprinting to motion. MRI. 2018 Dec 1;54:241-8
6. Atkinson D, Hill DLG, Stoyle PNR, Summers PE, Clare S, Bowtell R, Keevil SF. Automatic compensation of motion artifacts in MRI. MRM 1999;41:163–170.
7. Cheng JY, Alley MT, Cunningham CH, Vasanawala SS, Pauly JM, Lustig M. Nonrigid motion correction in 3D using autofocusing with localized linear translations. MRM 2012;68:1785–1797.
8. McGivney DF, Pierre E, Ma D, Jiang Y, Saybasili H, Gulani V, Griswold MA. SVD compression for magnetic resonance fingerprinting in the time domain. IEEE Trans Med Imaging 2014;33(12):2311-22.
9. Assländer J, Cloos MA, Knoll F, Sodickson DK, Hennig J, Lattanzi R. Low Rank Alternating Direction Method of Multipliers Reconstruction for MR Fingerprinting. MRM 2017; 79:83-96. doi:10.1002/mrm.26639.
10. Zhao B, Setsompop K, Adalsteinsson E, Gagoski B, Ye H, Ma D, Jiang Y, Ellen Grant P, Griswold MA, Wald LL. Improved magnetic resonance fingerprinting reconstruction with low-rank and subspace modelling. MRM 2018; 79(2):933-942. doi: 10.1002/mrm.26701.
11. Zhang T, Pauly JM, Levesque IR. Accelerating parameter mapping with a locally low rank constraint. MRM 2015;73:655–661.
12. Cruz G, Bustin A, Jaubert O, Schneider T, Botnar RM, Prieto C. Locally Low Rank Regularization for Magnetic Resonance Fingerprinting. ISMRM 2018; abstract number 3548.
Figures