4379
Free-Breathing Liver T1 and Fat Mapping Using a Golden-Angle-Ordered Variable Flip Angle Stack-of-Radial Sequence1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Physics and Biology in Medicine Interdepartmental Program, University of California, Los Angeles, Los Angeles, CA, United States, 3Department of Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Measurement of T1 and proton-density fat fraction (PDFF) in the liver can provide information about fibrosis and steatosis, respectively. Existing Cartesian acquisition schemes generally require breath-holding, which limits spatial coverage and may be difficult for sick, elderly or pediatric patients. In this study, we propose a golden-angle-ordered (GA) 3D stack-of-radial variable-flip-angle (VFA) sequence that can map T1 and PDFF simultaneously with close to full liver coverage under five minutes during free-breathing. Pilot studies in phantom and healthy subjects demonstrate feasibility and show good measurement repeatability.
Introduction
Quantitative MR parameters can be used to characterize liver diseases, such as T1 for fibrosis1-3 and proton-density fat fraction (PDFF) for steatosis4-6. Simultaneous T1 and PDFF mapping in the liver can be achieved with variable-flip-angle (VFA) multi-echo gradient-echo Cartesian protocols7, but their sensitivities to respiratory motion typically require breath holding which limits spatial coverage and is challenging for sick, elderly, and young subjects. Non-Cartesian acquisition schemes such as golden-angle-ordered (GA) 3D stack-of-radial sequence are more robust to motion and moderate undersampling. They can thus eliminate the need for breath-holding and offer larger coverage during a free-breathing scan8. We propose a 3D multi-echo gradient-echo golden-angle-ordered radial VFA sequence that can quantify liver T1 and PDFF in a single 4-minute free-breathing scan.Methods
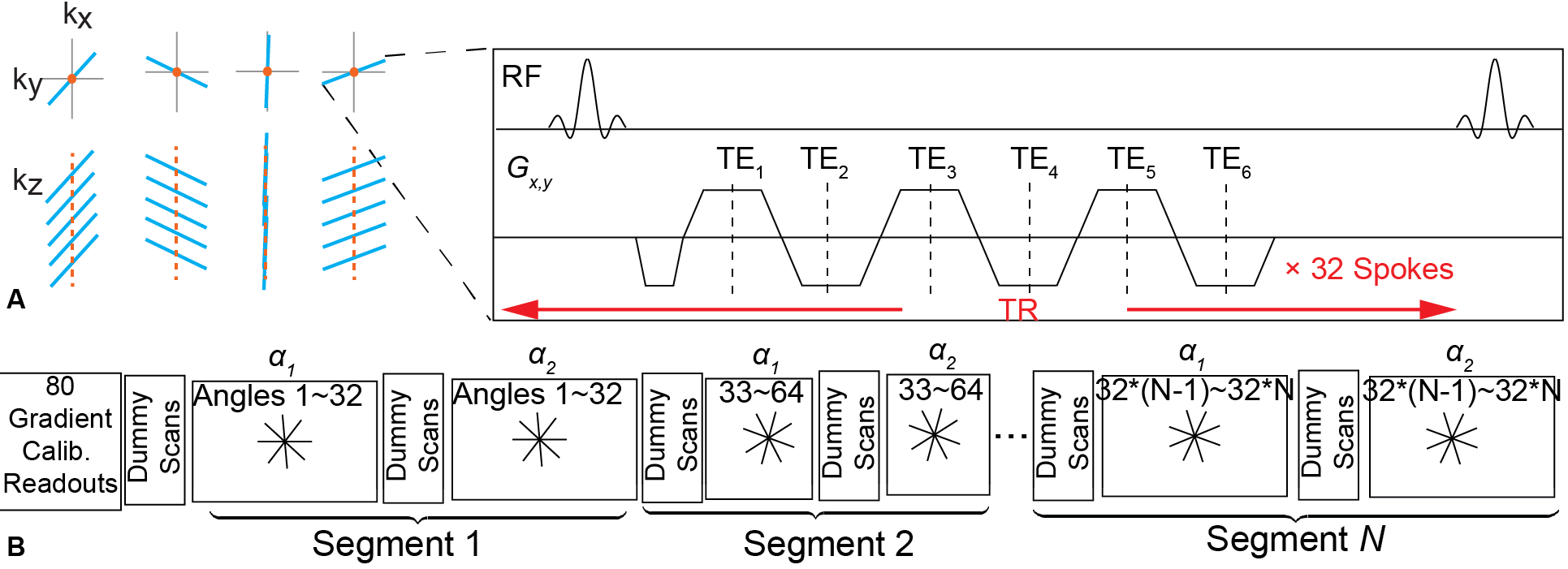
Fig.1 shows a diagram of the new sequence. A 3D stack-of-radial trajectory is acquired as segments of GA-ordered multi-echo readouts (Fig.1A) with alternating flip angles (radial VFA). 192 radial angles (6 segments) were acquired in total per slice, resulting in a 2.4-fold undersampling. Complex images were reconstructed for each channel and adaptively combined. Magnitude images of all echoes were combined as sum-of-squares for VFA T1 fitting. PDFF was calculated using the complex images of all TEs with a seven-peak fat model9 and single R2*10. T1 measurement using the proposed sequence was first evaluated in a standard T1/T2 phantom versus Cartesian inversion recovery (IR) and VFA protocols. Interclass correlation coefficient (ICC) was calculated to quantify the agreement. T1 and PDFF were then evaluated in healthy adult subjects (n=5 males), who underwent one radial VFA scan during normal breathing and one Cartesian gradient-echo VFA scan with reduced slice coverage in a single breath-hold. Both protocols were repeated to assess their repeatability. 40 regions of interest (ROI) each containing 16 voxels were drawn in T1 maps in slices shared by radial and Cartesian VFA acquisitions. 160 more ROIs were drawn in two repeated radial VFA scans. Bland-Altman analysis was performed to compare T1 measured by Cartesian and radial VFA and evaluate the repeatability of T1 and PDFF by radial VFA. MR spectroscopy (HISTO, Siemens) was acquired in a 15×15×15mm3 voxel during breath-hold as a reference for PDFF. To calibrate flip angles, B1+ maps were acquired during breath-holding using a vender-recommended protocol11. Scan parameters are listed in Table 1.Results
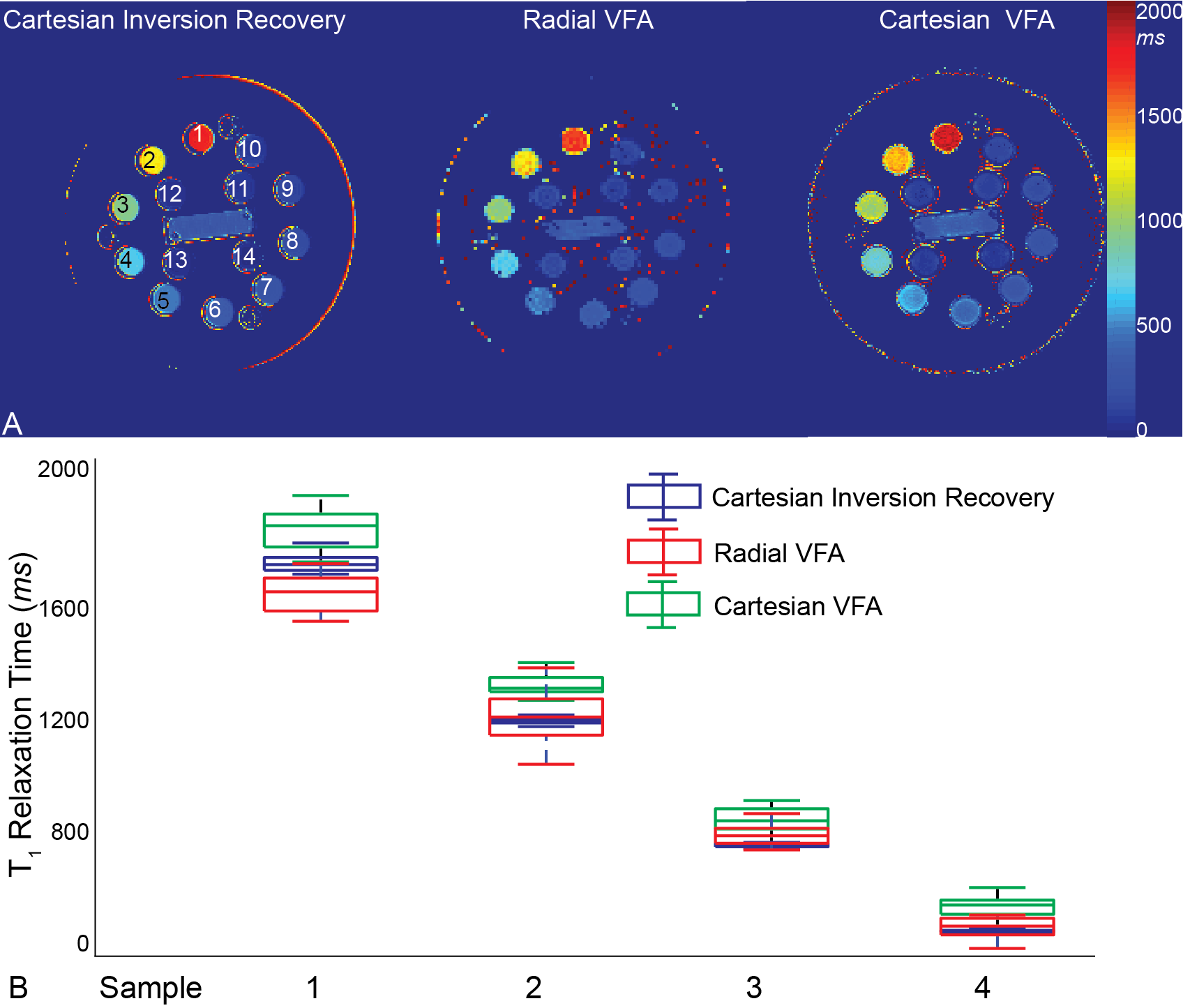
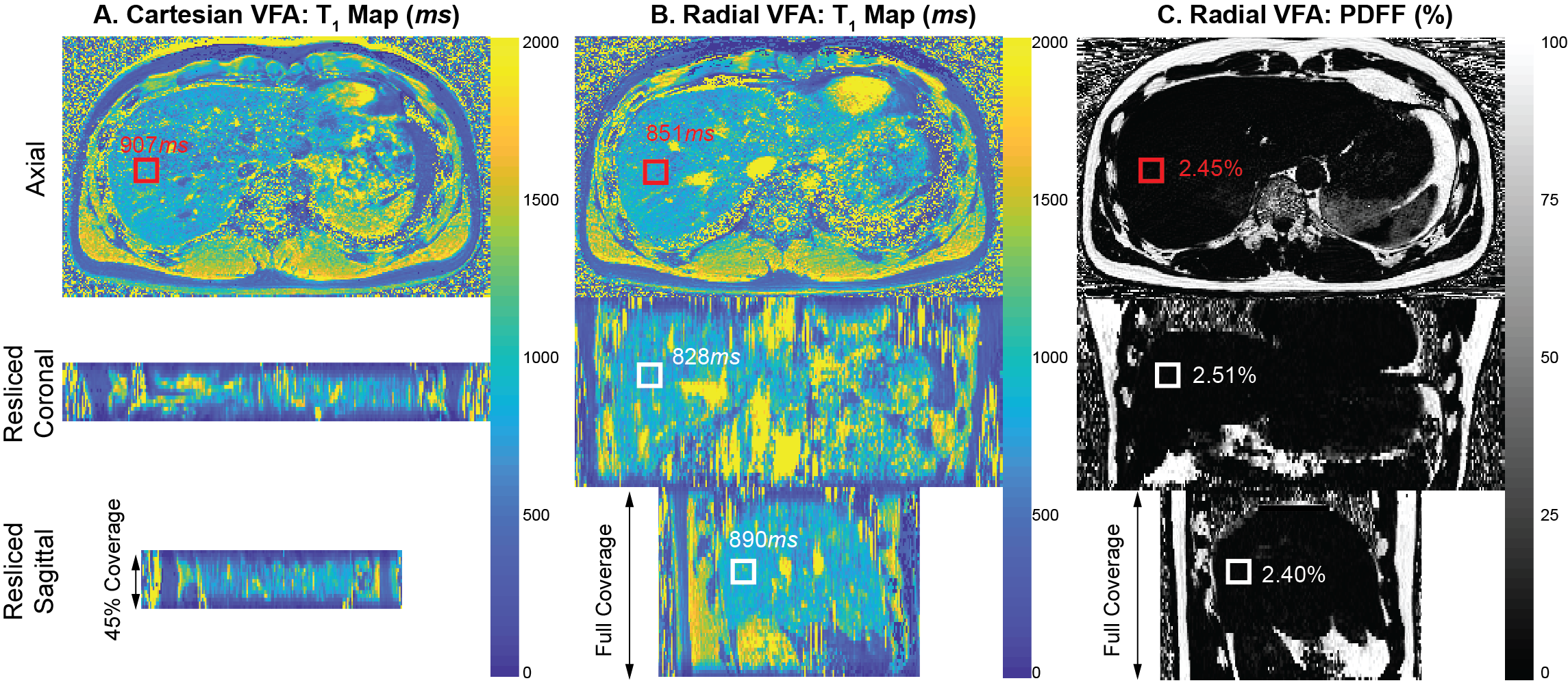
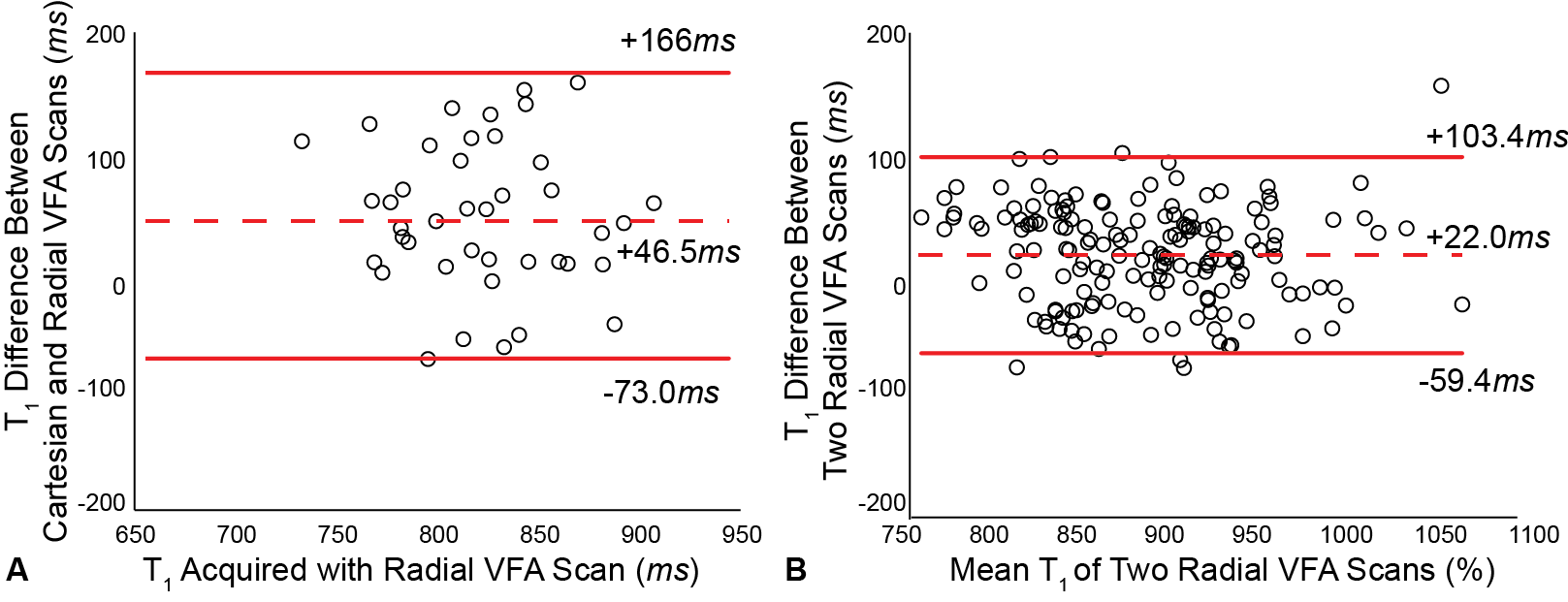
T1 maps obtained with radial VFA, Cartesian IR and VFA in the T1/T2 phantom are shown in Fig.2A. Box plots (Fig.2B) of samples 1~4, which had T1 close to expected liver T1, gave ICC=0.9796 between radial VFA and Cartesian IR and ICC=0.9461 between radial and Cartesian VFA. Fig.3 shows T1 maps acquired in one volunteer using Cartesian and radial VFA protocols, and PDFF maps using radial VFA. The ROI in which HISTO was acquired is shown in red, whose PDFF of 2.4% agreed well with radial VFA. Cartesian VFA generally yielded higher T1 than radial VFA (Fig.4A), consistent with phantom data, with mean difference of 46.5ms and limits of agreement (LoA) of [-73.0ms, 166.0ms]. Bland-Altman analysis of repeated Cartesian scans yielded a mean T1 difference of 30.2ms and LoA of [-100.5ms, 130.7ms], while in repeated radial VFA scans they were 22.0ms and [-59.4ms, 103.4ms], respectively, for T1 (Fig.4B), and 0.006% and [-0.618%, 0.630%] for PDFF. In repeated radial VFA scans ICC for T1 and PDFF were 0.7664 and 0.886, respectively. They also averaged to (889.4±60.1)ms and (2.66±0.29)% in all ROIs.Discussion and Conclusion
The major advantage of the proposed radial VFA sequence is fast (<5min), free-breathing simultaneous mapping of liver T1 and PDFF. It provides large spatial coverage of the liver (90%~100% of the liver along slice direction) and eliminates breath holding. The accuracy of the new sequence in T1 measurement was first confirmed with phantom studies. In vivo liver scans saw differences in T1 between Cartesian and radial VFA, which may be due to slice position mismatch and/or imperfect breath-holding during Cartesian scan. Radial VFA demonstrated good repeatability in T1 measurements despite imperfect B1+ maps. Repeatability of radial VFA PDFF quantification was confirmed with small inter-scan mean difference. The new sequence was only evaluated in a pilot study of healthy subjects and more evaluation is needed. Further improvement may include using phase-sensitive parallel imaging reconstruction techniques12 to suppress streaking artifacts caused by undersampling. Though this study only measured pre-contrast T1, the proposed sequence could evaluate T1 change after the injection of contrast agents. In conclusion, we have demonstrated the feasibility of a golden-angle-ordered stack-of-radial VFA free-breathing liver MRI method to achieve large spatial coverage and quantify T1 and PDFF within a few minutes.Acknowledgements
This work was supported by the Department of Radiological Sciences, UCLAReferences
1. Hoad CL, Palaniyappan N, Kaye P et al. A study of T1 relaxation time as a measure of liver fibrosis and the influence of confounding histological factors. NMR Biomed. 2015;28(6):706-714
2. Banerjee R, Pavlides M, Tunnicliffe EM et al. Multiparametric magnetic resonance for the non-invasive diagnosis of liver disease. J Hepatol. 2014;60(1):69-77
3. Li Z, Sun J, Hu X et al. Assessment of liver fibrosis by variable flip angle T1 mapping at 3.0T. J Magn Reson Imaging. 2016;43(3):698-703
4. Tang A, Tan J, Sun M et al. Nonalcoholic fatty liver disease: MR imaging of liver proton density fat fraction to assess hepatic steatosis. Radiology. 2013;267(2):422-431
5. Armstrong T, Martin T, Stemmer A et al. Free-breathing fat quantification in the liver using a multiecho 3D stack-of-radial technique: investigation of motion compensation and quantification accuracy. Proc. ISMRM. Paris, France 2017;p0363
6. Idilman IS, Aniktar H, Idilman R et al. Hepatic steatosis: quantification by proton density fat fraction with MR imaging versus liver biopsy. Radiology. 2013;267(3):767-75
7. Tamada D, Wakayama T, Onishi H et al. Multiparameter estimation using multi-echo spoiled gradient echo with variable flip angles and multicontrast compressed sensing. Magn Reson Med. 2018;80(4):1546-55
8. Armstrong T, Dregely I, Stemmer A et al. Free-Breathing liver fat quantification using a multiecho 3D stack-of-radial technique. Magn Reson Med. 2018;79(1):370-82
9. Ren J, Dimitrov I, Sherry AD et al. Composition of adipose tissue and marrow fat in humans by 1H NMR at 7 Tesla. J Lipid Res. 2018;49(9):2055-62
10. Hernando D, Kellman P, Haldar JP et al. Robust water/fat separation in the presence of large field inhomogeneities using a graph cut algorithm. Magn Reson Med. 2010;63(1):79-90
11. Chung S, Kim D, Breton E et al. Rapid B1+ mapping using a preconditioning RF pulse with TurboFLASH readout. Magn Reson Med. 201;64(2):439-46
12. Uecker M, Lustig M. Estimating absolute-phase maps using ESPIRiT and virtual conjugate coils. Magn Reson Med. 2017;77(3):1201-7
Figures