4345
Neurovascular, muscle, and skin changes on [18F]FDG PET/MRI in foot complex regional pain syndrome (CRPS)1Radiology, Stanford University, Stanford, CA, United States, 2Anesthesiology, Stanford University, Stanford, CA, United States, 3Orthopaedics, Stanford University, Stanford, CA, United States
Synopsis
Complex regional pain syndrome (CRPS) is a devastating chronic pain condition affecting 50,000 new patients every year in the U.S. Unfortunately, conventional methods for examining musculoskeletal damage such as physical exam or electrodiagnostic methods are very difficult to use for CRPS patients due to their extreme sensitivity to pain. In this abstract, we demonstrate the feasibility of [18F]FDG PET/MRI for investigating musculoskeletal changes from CRPS. Our results show the improved sensitivity of [18F]FDG PET to muscular, neurovascular, and skin changes over MRI, suggesting that [18F]FDG PET/MRI can be a valuable tool to monitor the pathologic process of CRPS.
Introduction
Every year, about 50,000 new cases of complex regional pain syndrome (CRPS) occurs in the U.S. (1), causing debilitating pain to the patients. Typical symptoms of CRPS include an extremely increased sensitivity to painful or nonpainful stimuli in the affected limbs, often suspected to be caused by traumatic nerve injury. Electrodiagnostic methods, the standard-of-care method for the assessment of nerve injury, are very difficult to employ because CRPS patients cannot often tolerate their invasive measurements. Recently, a simultaneous [18F]FDG PET/MRI method has demonstrated promising results in non-invasively detecting painful nerve damage and associated muscular changes (2). Encouraged by this research, we conducted a CRPS patient study using [18F]FDG PET/MRI to evaluate its feasibility for non-invasive detection of early musculoskeletal changes due to CRPS in comparison with conventional MRI.Methods
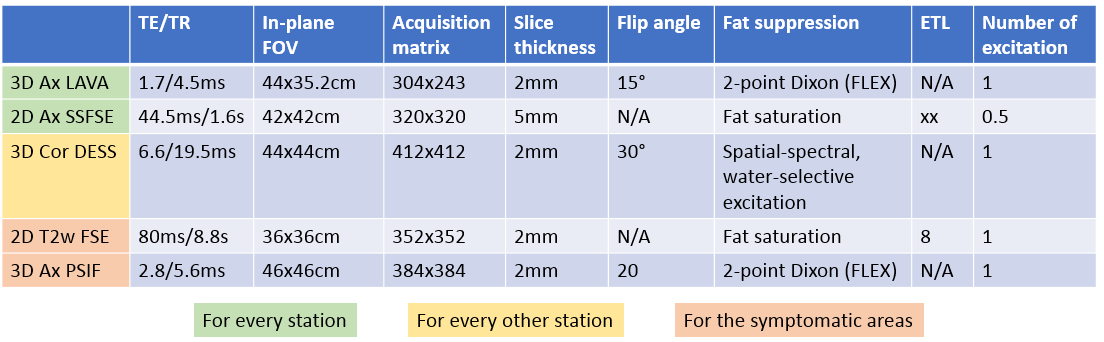
Seven CRPS patients presenting severe foot pain were recruited for our study. All patients satisfied the Budapest criteria (3) to be classified as a CRPS patient. An informed consent form reviewed by the Stanford institutional review board was obtained for each patient before the imaging study. A GE SIGNA PET/MRI system (time-of-flight PET; 3.0T bore) was used in our imaging study, and the imaging started one hour after a single 10 mCi injection of [18F]FDG. Eight to ten imaging stations were prescribed to scan the whole-body, where PET and MRI scans were performed simultaneously. MRI sequences adopted in each imaging station and additional sequences only for affected limb areas are summarized in Fig.1.
We performed a radiologic review of the PET/MRI images to identify metabolic (PET) and anatomic (MRI) abnormalities in patients. The maximum SUV (SUVmax) of [18F]FDG on the lesions in three different tissue types (muscle, neurovascular bundle, skin) were measured using image analysis software (OsiriX v.6.0). The two-tailed Mann-Whitney U-test was employed to compare the SUVmax between the detected lesions and the corresponding tissues from 7 healthy controls
Results
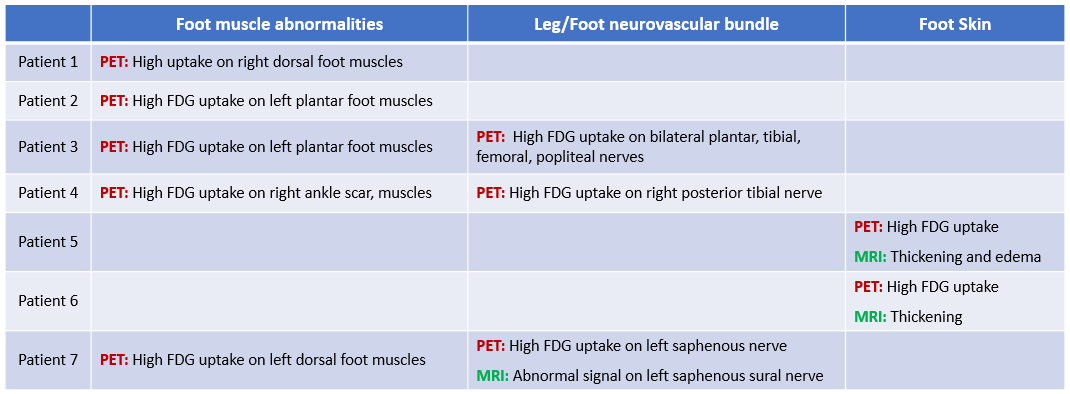
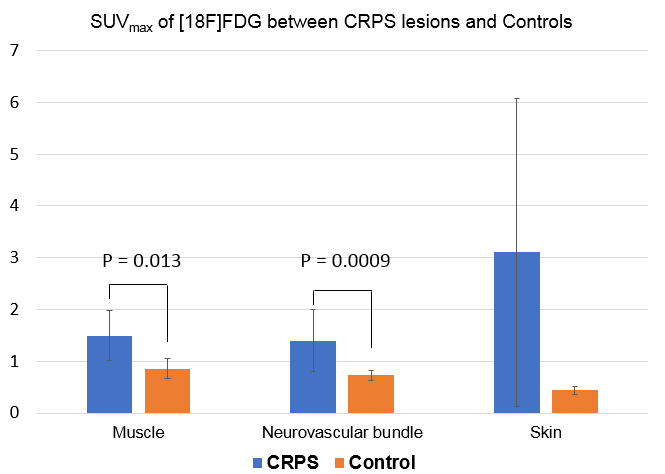
We found abnormally high [18F]FDG uptake in foot muscles (5 patients), neurovascular bundles in the legs (3 patients), and skin (2 patients). MRI abnormalities were also found on the skin lesions of high [18F]FDG uptake, but much less frequently in the neurovascular bundle and foot muscle lesions of high [18F]FDG uptake (Fig.2). The mean and standard deviation of SUVmax from the muscular / neurovascular / skin lesions were 1.49±0.50 / 1.40±056 / 3.10±2.97 while those values for the healthy volunteers were 0.86±0.19 / 0.6±0.05 / 0.4±0.08 (Fig.3). The difference of the [18F]FDG uptake was significant with the p-values of the U-test being 0.013 (muscular lesion vs controls) and 0.0009 (neurovascular lesions vs controls). The p-value of the skin lesions was unavailable due to a small sample size.
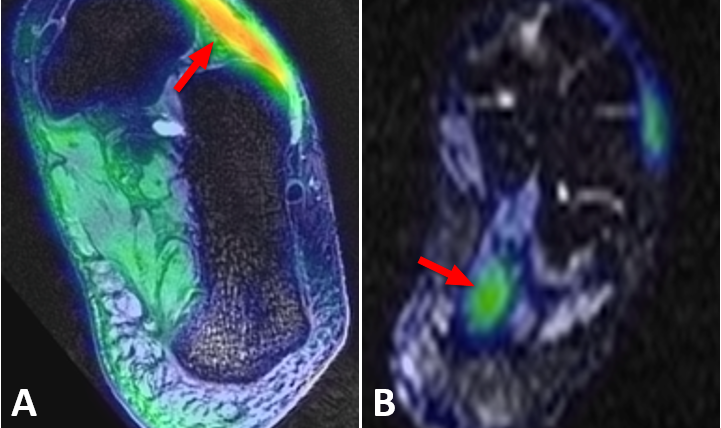
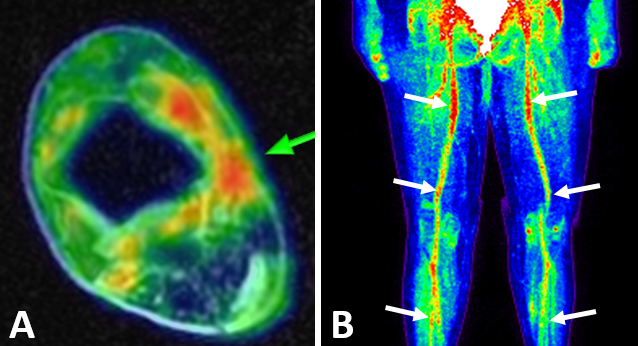
Fig.4 shows two cases of significantly increased [18F]FDG uptake on the extensor digitorum brevis (Fig.4A) and the flexor digitorum brevis muscle (Fig.4B). The location of the high [18F]FDG uptake coincided with the site of pain, but no abnormalities (e.g. edema, atrophy, fat infiltration) were identified on MRI. Fig.5 presents PET/MRI abnormalities on neurovascular bundles. Fig.5A shows locally increased [18F]FDG uptake in the tibial nerve at the ankle surrounded by scar tissue. Fig.5B shows globally increased [18F]FDG uptake on major neurovascular bundles from the pelvis to foot, involving femoral, popliteal, and tibial neurovascular bundles. Interestingly, the patient’s pain was limited to the lower calf and the foot.
Discussion
In this study, we investigated the feasibility of [18F]FDG PET/MRI to examine the changes on muscles, neurovascular bundles, and skin in the symptomatic limbs of CRPS patients. In most patients, significantly increased metabolism was observed on the muscles at the painful area whereas no obvious damage was found on MRI. This may demonstrate the sensitivity of [18F]FDG PET to early inflammatory changes before the onset of severe muscle atrophy visible on MRI. Due to the relatively coarse resolution of PET imaging (about 4mm), the uptake between the peripheral nerve and the surrounding blood vessels could not be separated, and thus they were presented together as neurovascular bundle uptake. Further developments from high-resolution MRI can be a potential solution for better separation. The case of global [18F]FDG uptake on multiple neurovascular bundles may indicate the possibility of differentiating CRPS into subtypes depending on the existence of global uptake patterns, which could be a surrogate marker for the autoimmune component being increasingly investigated in the etiology of CRPS.Conclusion
In summary, we have demonstrated the feasibility of [18F]FDG PET/MRI for investigating muscular, neurovascular, and skin changes due to CRPS. Our approach showed improved sensitivity over the conventional MRI examination.Acknowledgements
NIH R01 AR0063643, NIH P41 EB015891, GE Healthcare.References
1. A.T. Borchers, and M.E. Gershwin, Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev, 13(3): p. 242-65, 2014.
2. P. Cipriano, D. Yoon, H. Gandhi, D. Holley, D. Thakur, M. Ith, B. Hargreaves, D. Kennedy, M. Smuck, I. Cheng, S. Biswal. 18F-FDG PET/MRI in Chronic Sciatica: Early Results Revealing Spinal and Non-spinal Abnormalities. J. Nucl. Med., 2017 (online available)
3. R.N. Harden at al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regiona Pain Syndrome. Pain, 150:268-74, 2010.
Figures