4328
Hybrid Rectal Multiparametric F18-FDG PET/MR in Restaging Locally Advanced Rectal Cancer: An initial experience1Radiology, Mayo Clinic Arizona, Scottsdale, AZ, United States, 2Surgery, Mayo Clinic Arizona, Scottsdale, AZ, United States, 3Radiation Oncology, Mayo Clinic Arizona, Scottsdale, AZ, United States
Synopsis
Rectal cancer is a leading cause of cancer death in the United States. Current standard of care in locally advanced rectal cancer includes chemoradiation therapy followed by surgical resection. Accurate radiological restaging therapy is essential for success of surgery. In this preliminary study, we investigated the synergistic role of rectal mpMRI and F18-FDG PET/MR in evaluation of response to therapy in advanced rectal cancer. Our data show promising added value of this “one-stop” imaging modality in providing complementary morphological and functional information in the detection of viable primary tumor as well as nodal and distal metastases, utilizing both MRI and PET molecular imaging biomarkers.
Introduction
Colorectal cancer is the third leading cause of cancer-related deaths in the United States. There have been significant changes in the management of rectal cancer over the past 10 to 15 years with pre-operative chemoradiation therapy adapted as the first-line management approach in locally advanced rectal cancer. Accurate radiological restaging after chemoradiation therapy contributed to improvements in the management and survival of patients. Gadolinium-enhanced multiparametric (mp) rectal MRI is the preferred imaging modality for the staging of rectal cancer. F18-FDG PET/MR is a valuable staging tool for detecting distant metastasis as well as for the evaluation of residual viable tumor and pelvic lymph nodes. Combining excellent soft tissue contrast with functional molecular imaging information, hybrid rectal PET/MR has the potential to add significant value to the initial workup and assessment of treatment course in rectal cancer.Methods
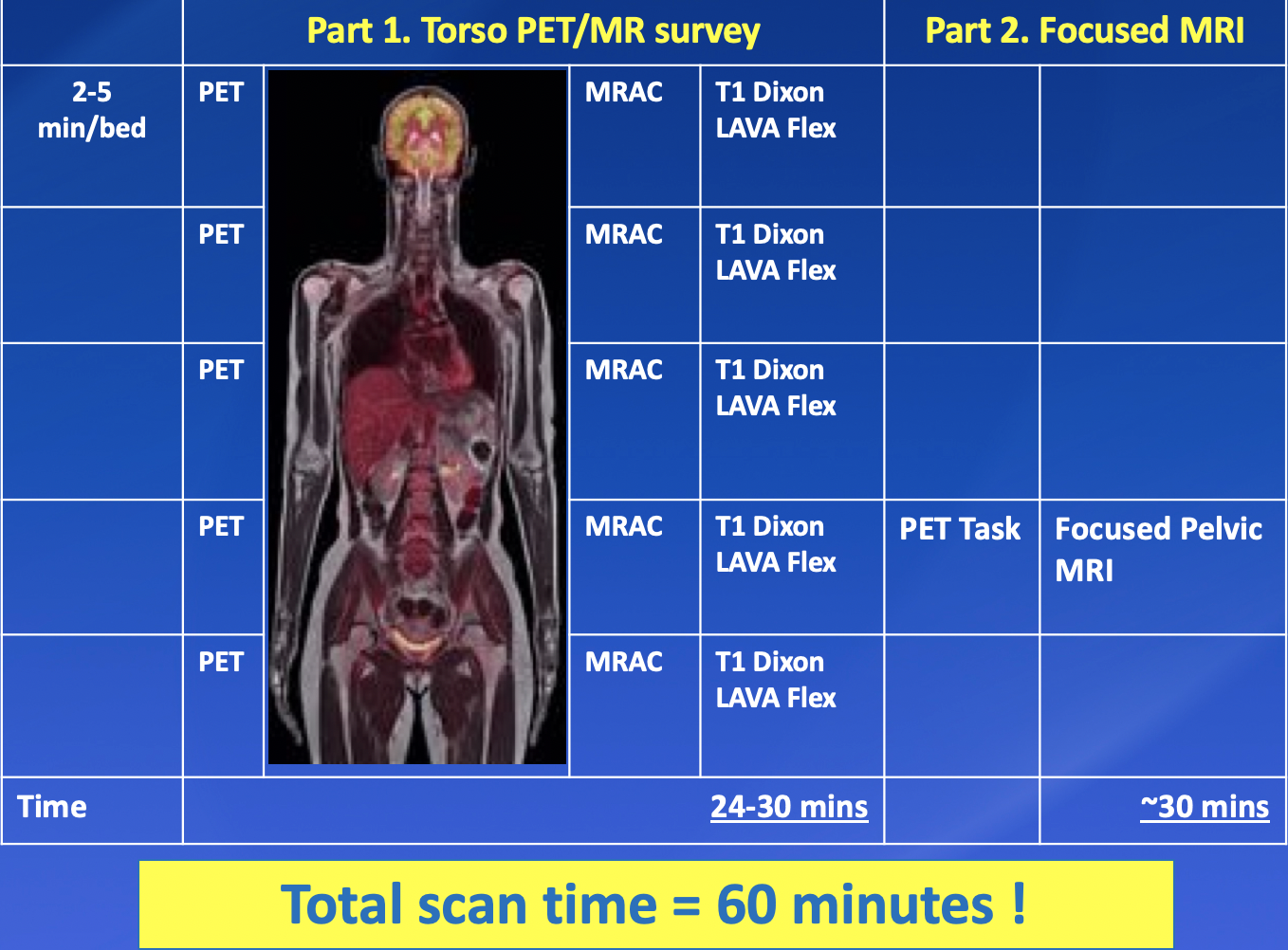
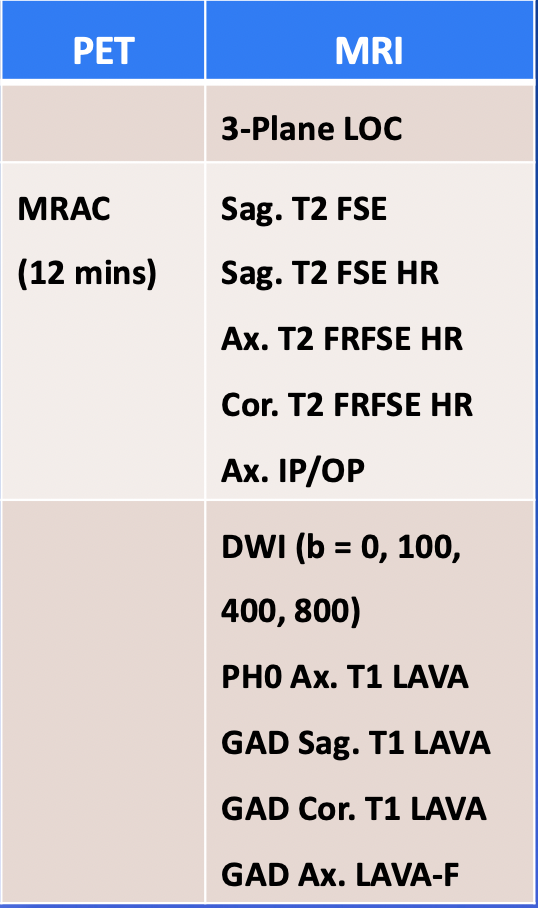
We reviewed the PET/MR images of the 19 locally advanced rectal cancer patients at our institution. All patients underwent F18-FDG PET/MR scans on a 3T PET/MR scanner 60 minutes after intravenous administration of 10 ± 1 mCi FDG. The hybrid F18-FDG PET/MR protocol consisted of two parts (Figure 1): 1) torso PET/MR survey and 2) focused pelvic/rectal mpMRI. During the torso PET/MR survey, 5 bed positions covering vertex of skull to thigh were performed over 24 to 30 minutes. MR-based attenuation correction (MRAC) images and four segmented T1-weighted DIXON-LAVA sequences (water, in/oppose-phase and fat) were acquired simultaneously and reconstructed using time-of-flight (TOF) method. The focused pelvic/rectal mpMRI was performed at a single bed position and comprised multi-planar T1- and T2-weighted sequences, diffusing weighted imaging (DWI) with b values at 0, 100, 400 and 800, respectively, as well as multiphase post-contrast T1-weighted images. During the focused rectal mpMRI acquisition, a simultaneous PET task was also performed, including an MRAC series and 12-minute PET data acquisition, ensuring accurate PET/MR fusion and increasing lesion conspicuity (Figure 2).
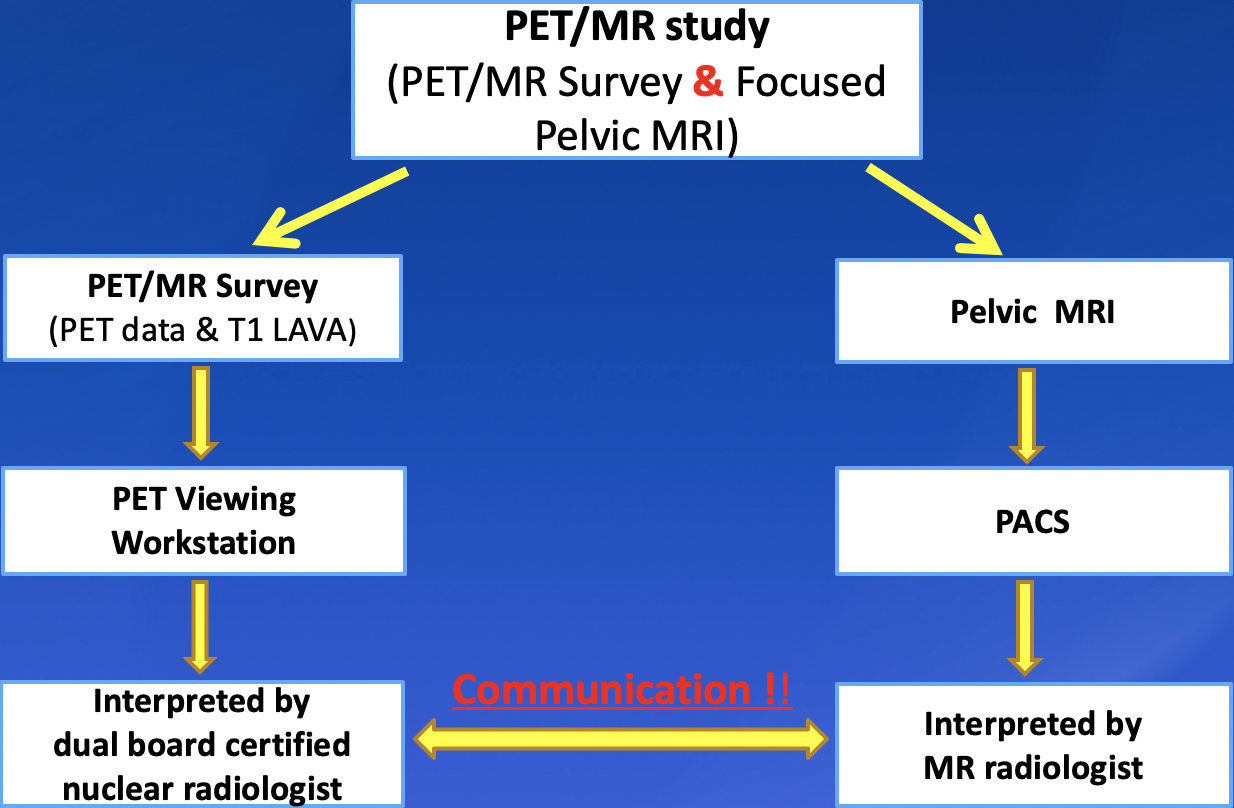
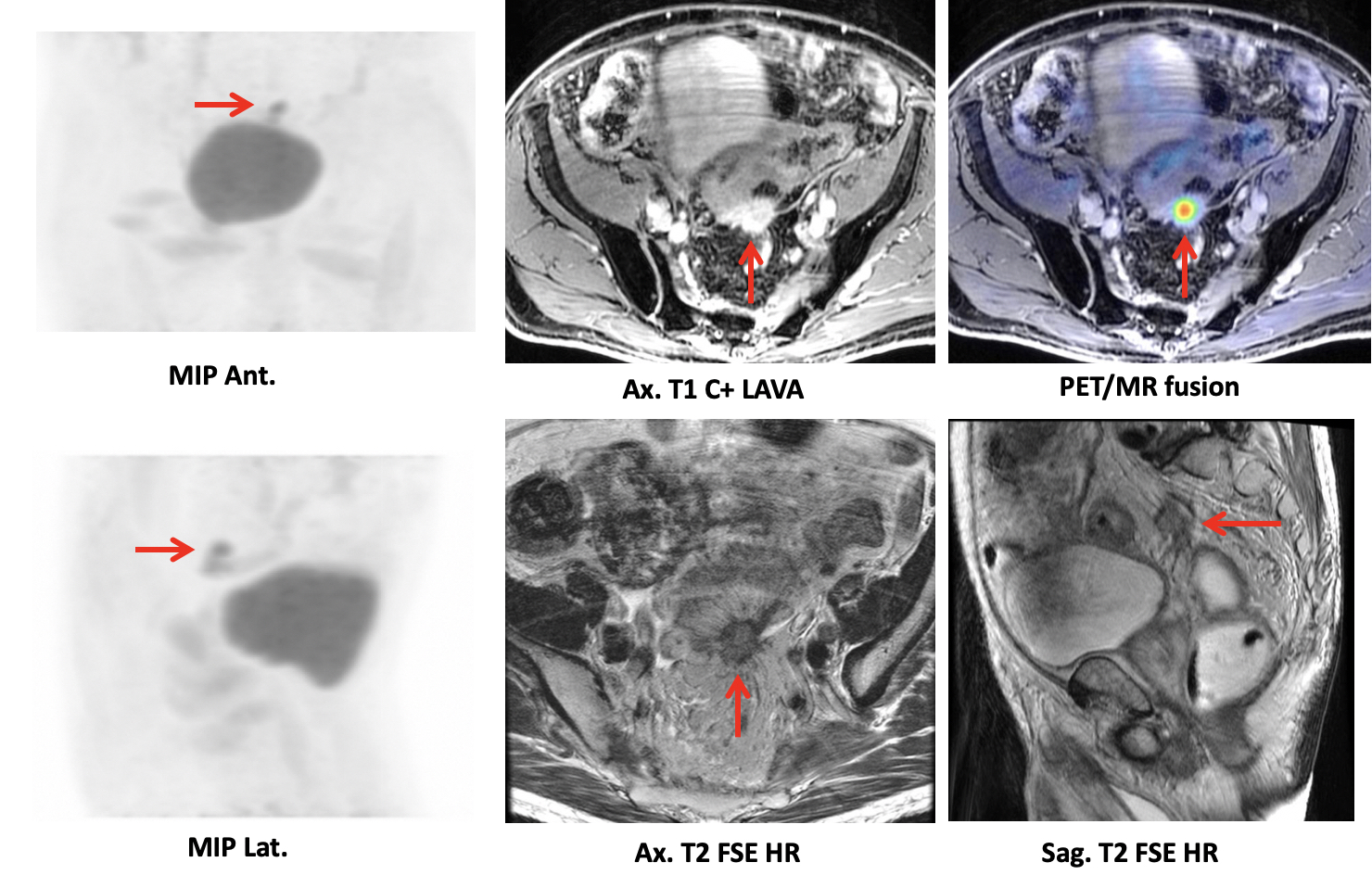
Imaging analysis: The torso PET/MR survey series were reviewed by a dual-board certified nuclear radiologist on a MIM Vista workstation. The maximum standard uptake value (SUVmax) of the rectal neoplasm, locoregional lymph nodes and distant metastases were measured. The focused rectal mpMRI images were reviewed on a PACS workstation by an experienced abdominal MR radiologist. Consensus diagnosis of each lesion was achieved by both radiologists (Figure 3).
Results
Of 19 patients with PET/MR scans, 14 were performed for re-staging purposes. Among these 14 patients, 10 (71%) had received chemoradiation therapy for primary malignancy and 4 (29%) received 5-FU therapy with/without Avastin.
All primary rectal neoplasms showed abnormal MR imaging features and variable degree FDG uptake (SUVmax 2.2 to 10.2).
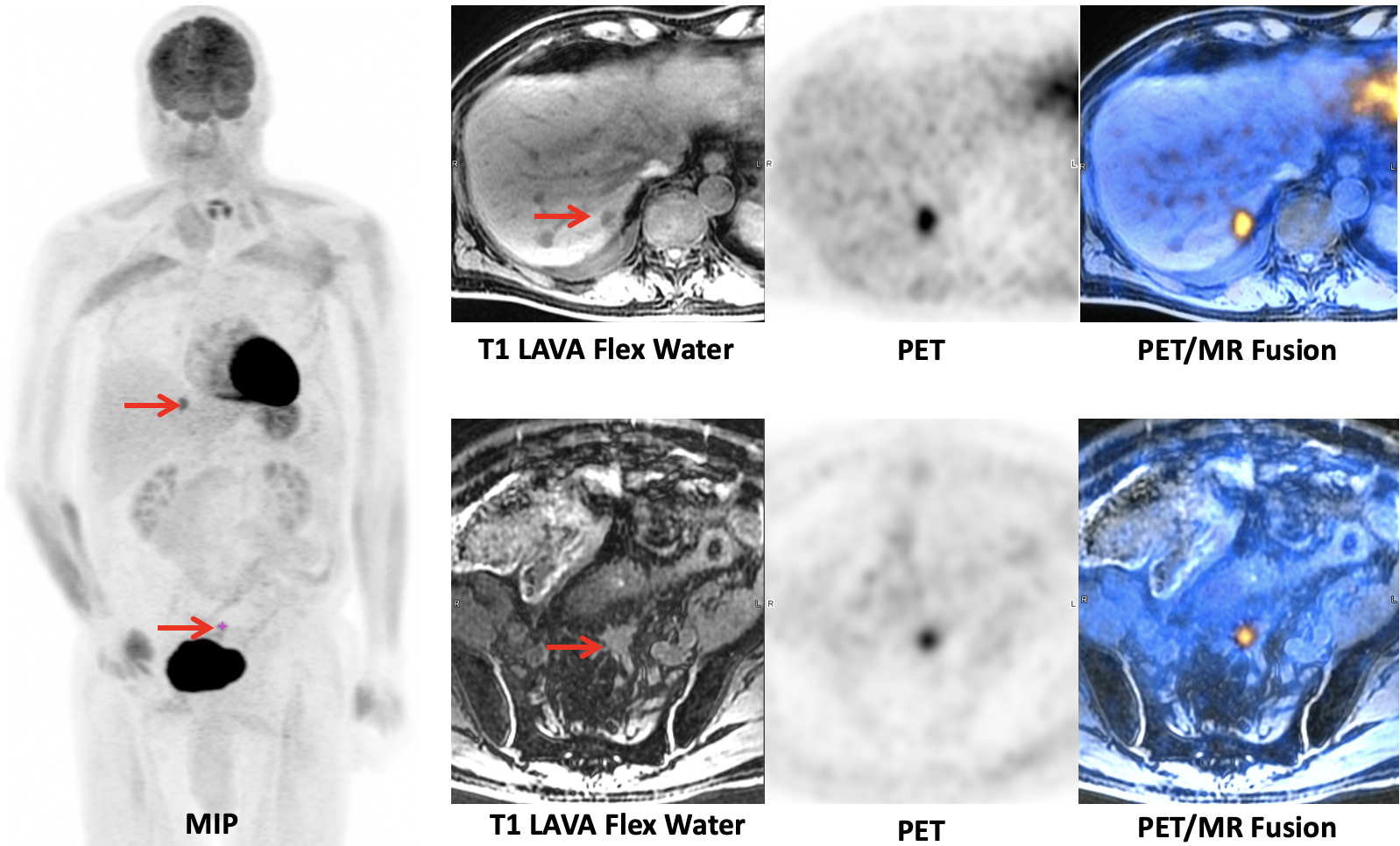
Nodal and distant metastases: There were greater than 10 FDG-avid lymph nodes (SUVmax 2.9 to 24.2) identified on PET, regardless of their overall size, in 8 patients.
Distant metastases were detected in 5 of 14 (36%) patients (Figures 4 and 5), with lesions located in lung, liver, mesentery and skeleton (SUVmax 6.2 to 15.8). All 5 of these patients were excluded for planned radical surgical resection of primary tumor.
Discussion
Our initial experience with F18-FDG PET/MR with focused pelvic MR protocol has shown benefit in pre-operative evaluation of locally advanced rectal cancer based on assessment of tumor burden and distant metastatic disease following neoadjuvant chemotherapy and/or radiation therapy. Preliminary data suggest added value of metabolic data to the high-resolution pelvic MRI protocol via the detection of locoregional nodal metastases that may be below specific size parameters on conventional MRI, as well as the detection of distant metastases including skeletal, liver, and lung.Conclusion
Hybrid rectal F18-FDG PET/MRI is a novel “one-stop” imaging modality in evaluation of response to therapy for locally advanced rectal cancer. The complementary information derived from mpMRI and PET molecular imaging biomarkers is able to provide accurate restaging information and guide clinical management.Acknowledgements
We thank the multidisciplinary oncology team at the Mayo Clinic in Arizona for its support.References
1. Agarwal A, Marcus C, Xiao J, Nene P, Kachnic LA, Subramaniam RM. FDG PET/CT in the management of colorectal and anal cancers. AJR Am J Roentgenol 2014;203(5):1109-19.
2. Jhaveri KS, Hosseini-Nik H. MRI of Rectal Cancer: An Overview and Update on Recent Advances. AJR Am J Roentgenol 2015;205(1):W42-55.
3. Kang B, Lee JM, Song YS, Woo S, Hur BY, Jeon JH, et al. Added Value of Integrated Whole-Body PET/MRI for Evaluation of Colorectal Cancer: Comparison With Contrast-Enhanced MDCT. AJR Am J Roentgenol 2016;206(1):W10-20.
Figures