4327
Cancer screening using 18F-FDG PET/MR in asymptomatic subjects: a preliminary report1Universal Medical Imaging, Shanghai, China, 2MR collaboration, Diagnostic Imaging, Siemens Healthcare, Shanghai, China, 3MR Scientific Marketing, Diagnostic Imaging, Siemens Healthcare, Beijing, China
Synopsis
This study was performed to evaluate the diagnostic value of PET/MR for cancer screening in asymptomatic subjects. 1491 subjects in total were enrolled in this study. 33 cases were diagnosed with malignant tumors, whereas 17 cases were correctly detected by PET/MR and 16 cases were detected by other methods. The overall detection rate of PET/MR in asymptomatic subjects was 1.14%, and the sensitivity, specificity, positive predictive value, and negative predictive value of PET/MR were 51.52%, 99.66%, 77.27% and 98.91%, respectively. As a cancer screening method, FDG PET/MR has great potentials to detect various kinds of tumors and should be beneficial to combine with other screening modalities.
Introduction
Cancer is a leading cause of death worldwide. The diagnosis and treatment of the tumor in its early stage is the best way to improve prognosis. In recent years, PET/CT has been used as a new modality for cancer screening in asymptomatic subjects and shown great potential in detecting various malignant tumors.1-8 Compared to PET/CT, the advantages of 18F fluorodeoxyglucose (FDG) positron emission tomography/magnetic resonance imaging (PET/MRI) are 1) better soft tissue contrast, 2) low-dose radiation, 3) simultaneous acquisition of functional MRI and PET data, allowing multi-parametric tumor evaluation.9 There have been extensive studies on the diagnostic values of PET/MRI for local diseases. However, PET/MRI as a whole-body cancer screening method has not been studied on a large population of healthy subjects. This study aims to evaluate the clinical values of PET/MRI for cancer screening in a large cohort of asymptomatic subjects.Methods
After excluding individuals with history of malignant tumor or incomplete data, 1,491 individuals who took cancer screening program (January 1st 2017 to December 31st 2017) in our center were retrospectively selected. The mean ages of the subjects were 49.15±9.95 years (range 21-86 years). Besides PET/MRI examination, the screening methods included ultrasound, CT and tumor marker tests of carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), prostate-specific antigen (PSA for male) and carbohydrate antigen 125 (CA125 for female).
18F-FDG PET/MRI was performed on a whole-body PET/MRI scanner (Biograph mMR, Siemens Healthcare, Erlangen, Germany) with 5 to 6 bed positions. PET data acquisition started 60 mins after the injection of 18F-FDG (3.7 MBq/Kg). The MRI protocols included whole-body (WB) T1 VIBE, WB T2 HASTE, WB DWI, brain T2 FLAIR and spinal T2 TSE.
Subjects who had no positive findings in the following 10 months were considered as ‘cancer negative’ when calculating sensitivity, specificity, and positive and negative predictive values (PPV and NPV).
Results
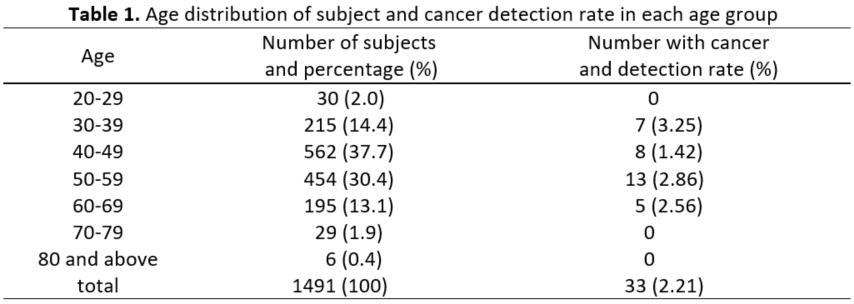
Among the total 1,491 subjects, 33 of them were found with malignant tumors, including 11 male and 22 female cases. The detection rate in each age group is summarized in Table 1.
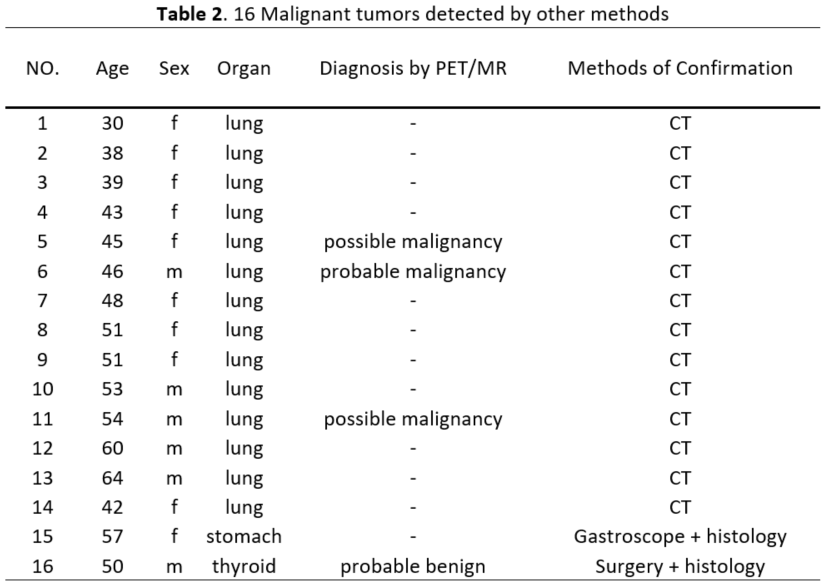
In theses 33 patients, 17 cases were correctly detected by PET/MRI, including lung tumor (1 case), breast tumor (7 cases), thyroid tumor (4 cases), stomach tumor (1 case), liver tumor (2 cases), salivary gland tumor (1 case) and cervix tumor (1 case). 16 cases were missed by PET/MRI but were detected by other modalities (considered as false negative). These 16 malignant cases comprised lung tumor (14 cases), thyroid tumor (1 case) and stomach cancer (1 case), as shown in Table 2.
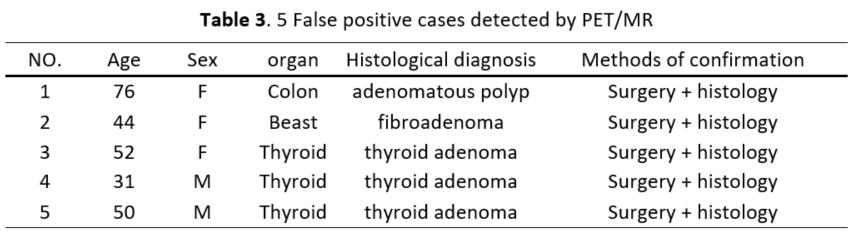
Using PET/MRI, 22 subjects were suspected to have malignant lesions and only 17 of them were correctly diagnosed. The 5 false-positive subjects found by PET/MRI included thyroid cancer (3 cases), breast cancer (1 case), and colon cancer (1 case). These cases have been confirmed as benign lesions by surgery (Table 3).
The detection rates of the complete screening program and PET/MRI-only screening were 2.21% (33/1,491) and 1.14% (17/1491), respectively. The sensitivity, specificity, PPV and NPV of PET/MRI screening were 51.52% (17/33), 99.66% (1453/1458), 77.27% (17/22) and 98.91% (1453/1469), respectively.
Discussion
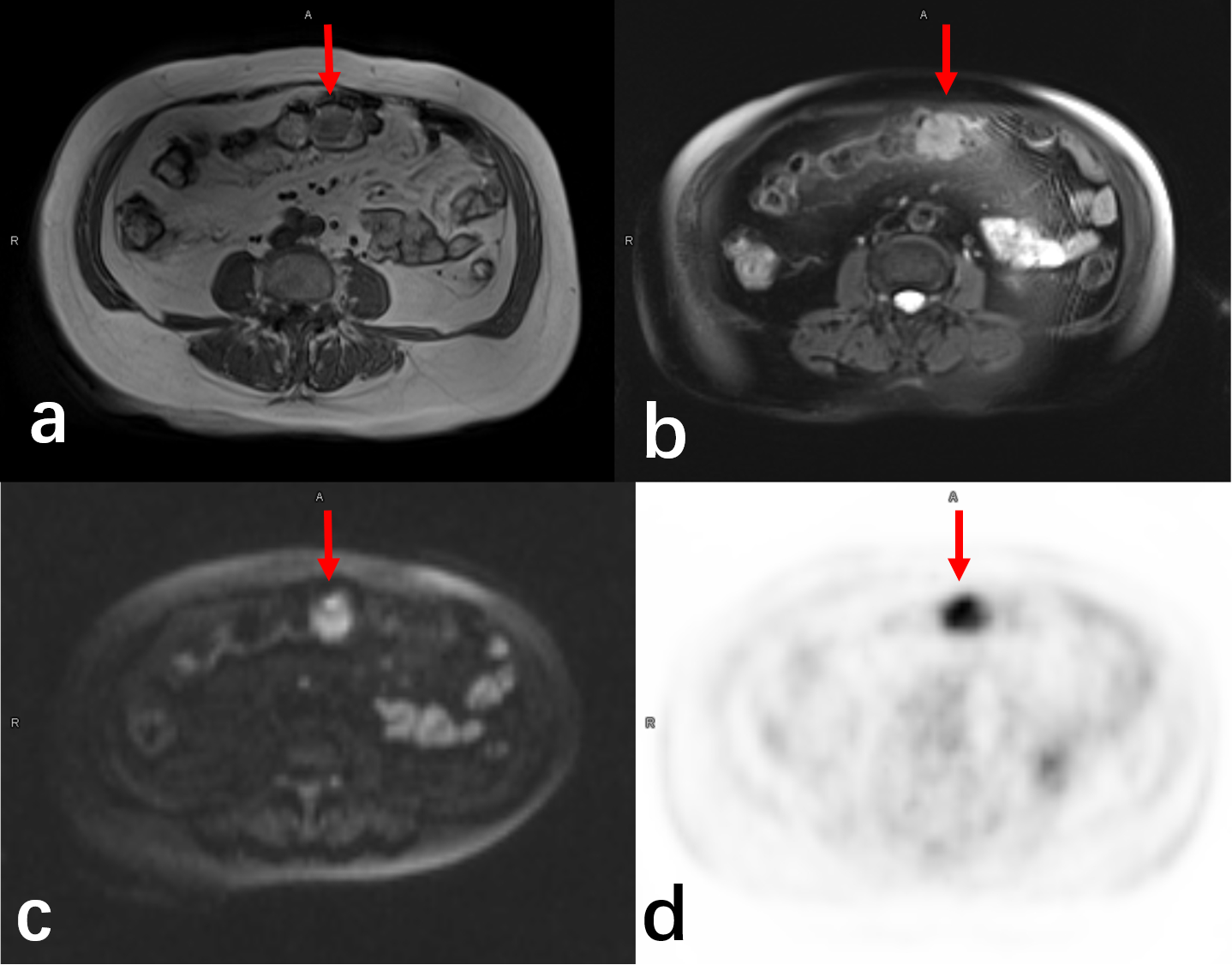
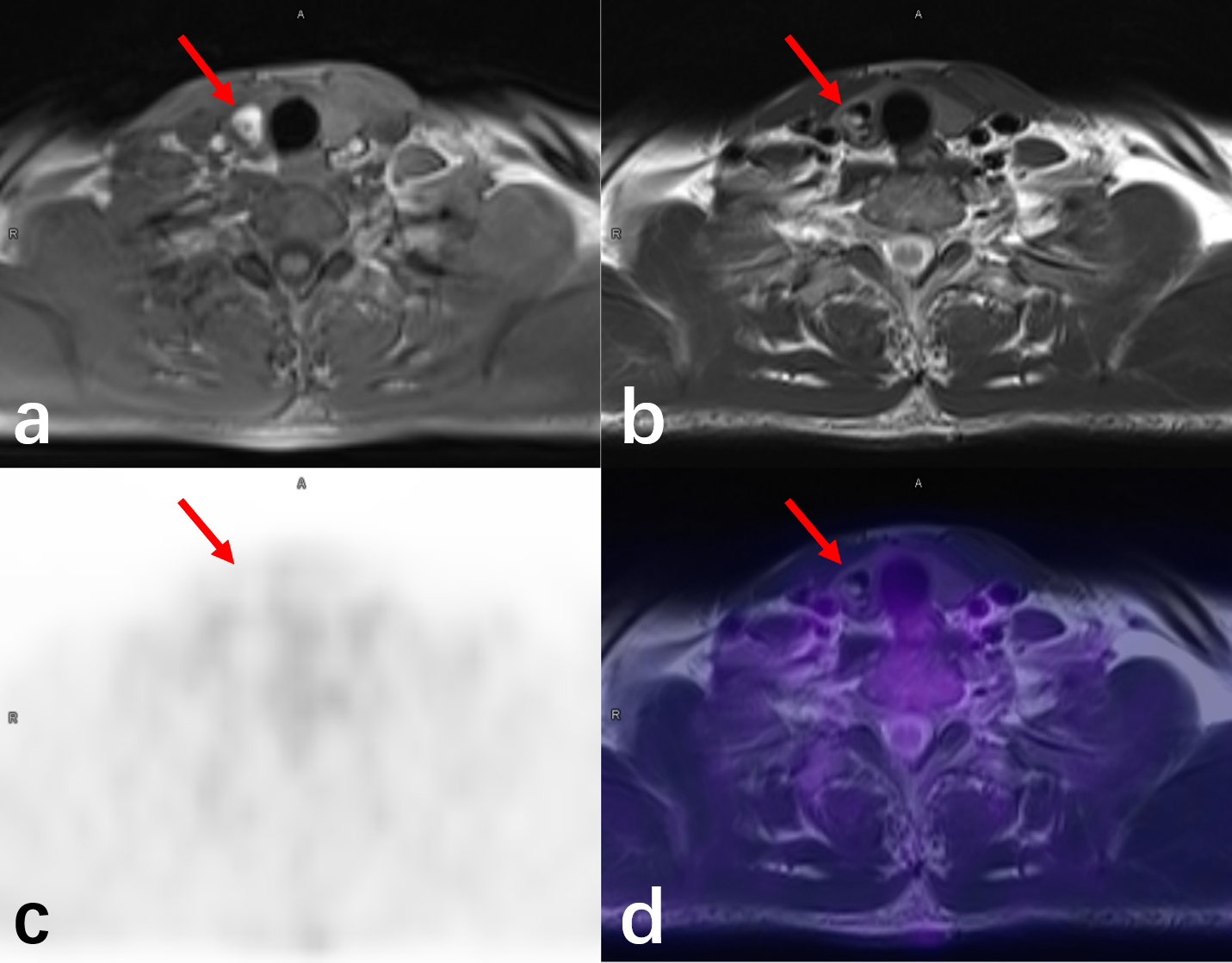
To the best of our knowledge, this is the first study on evaluating the clinical values of FDG PET/MRI for cancer screening in a large cohort of asymptomatic volunteers. In this study, the cancer detection rate of PET/MRI was 1.14%, which is similar to the rate of PET/CT ranging from 0.9% to 1.3% in previous studies [1-8]. It should be noted that most of the false-negative cases by PET/MRI (14/16) were lung cancer, for which CT has a very high detecting accuracy. Therefore, a supplementary CT examination is necessary for PET/MRI screening. If missed lung cancer cases were correctly diagnosed, the detection rate would be increased to 2.08% that is much higher than PET/CT. Some benign tumors may also have high uptake of FDG and lead to false positive detections (Figure 1). An example of false negative is shown in Figure 2.
The risk of radiation-induced cancer is 5/10,000 for an effective dose of 10 mSv.10 For a male subject of 75kg, the received does and cancer risk from PET/MRI are 4.71 mSv (0.017 mSv/MBq × 3.7 MBq/Kg × 75Kg) and 2.36/10,000, respectively, which is about one third from that of PET/CT.11
Conclusion
Based on the findings in this study, we suggest that FDG PET/MR might be an effective cancer screening modality in appropriate combination with other screening modalities.Acknowledgements
No acknowledgement found.References
1 Chen YK, Ding HJ, Su CT, Shen YY, Chen LK, Liao AC, Hung TZ, Hu FL, Kao CH. Application of PET and PET/CT imaging for cancer screening. Anticancer Res 24(6):4103-4108, 2004.
2 Ono K, Ochiai R, Yoshida T, Kitagawa M, Omagari J, Kobayashi H, Yamashita Y. The detection rates and tumor clinical/pathological stages of whole-body FDG-PET cancer screening. Ann Nucl Med 21(1):65-72, 2007.
3 Shen YY, Su CG, Chen YK, Liao AC, Tsai FS. The value of 18F-fluorodeoxyglucose positron emission tomography with the additional help of tumor markers in cancer screening. Neoplasma 50(3):217-221, 2003.
4 Kojima S, Zhou B, Teramukai S, Hara A, Kosaka N, Matsuo Y, Suzuki H, Torigoe S, Suzuki T, Uno K, Fukushima M. Cancer screening of healthy volunteers using whole-body 18F-FDG-PET scans: The Nishidai clinic study. Eur J Cancer 43(12):1842-1848, 2007.
5 Terauchi T, Murano T, Daisaki H, Kanou D, Shoda H, Kakinuma R, Hamashima C, Moriyama N, Kakizoe T. Evaluation of whole-body cancer screening using 18F-2-deoxy-2-fluoro-D-glucose positron emission tomography: a preliminary report. Ann Nucl Med 22(5):379-385, 2008.
6 Minamimoto R, Senda M, Uno K, Jinnouchi S, Iinuma T, Ito K, Okuyama C, Oguchi K, Kawamoto M, Suzuki Y, Tsukamoto E, Terauchi T, Nakashima R, Nishio M, Nishizawa S, Fukuda H, Yoshida T, Inoue T. Performance profile of FDG-PET and PET/CT for cancer screening on the basis of a Japanese Nationwide Survey. Ann Nucl Med 21(9):481-498, 2007.
7 Tong J, Zou Y, Jiang J, et al. Cancer screening of asymptomatic individuals using 18F-FDG PET/CT in China: a retrospective study. Discovery medicine 22(121): 181-188, 2016.
8 Lee JW, Kang KW, Paeng JC, Lee SM, Jang SJ, Chung JK, Lee MC, Lee DS. Cancer screening using 18F-FDG PET/CT in Korean asymptomatic volunteers: a preliminary report. Ann Nucl Med 23(7):685-691, 2009.
9 Gatidis S, Schmidt H, Claussen CD, Schwenzer NF. Multiparametrische Bildgebung mittels simultaner MR/PET. Radiology. 53:669–75, 2013.
10 International Commission on Radiological Protection. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann ICRP 37(2-4):199-203, 2007.
11 Huang B, Law M W M, Khong P L. Whole-body PET/CT scanning: estimation of radiation dose and cancer risk[J]. Radiology, 251(1): 166-174, 2009.
Figures