4310
Hyperpolarised [1-13C]pyruvate imaging of response to Bevacizumab1Division of Neurosurgery, Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom, 2CRUK Cambridge Institute, University of Cambridge, Cambridge, United Kingdom
Synopsis
13C chemical shift images were obtained from orthotopic rat models of glioblastoma prior to and following treatment with Bevacizumab. The resulting change in the hyperpolarized [1-13C]lactate/[1-13C]pyruvate ratio differed depending upon the model used. In U87 tumors the ratio increased and in patient-derived xenografts it decreased, with long term treatment of this latter model producing an invasive phenotype.
INTRODUCTION Bevacizumab is a recombinant, humanized monoclonal antibody that inhibits VEGF receptor-mediated cell signalling by sequestration of its ligand VEGF-A. Despite efficacy in several phase 2 trials, three recent phase 3 trials failed to show an increase in overall survival, with increased adverse effects noted (1-3), although there was an increase in progression free survival (PFS). However, PFS is inferred from a reduction in contrast-enhancement on T1-weighted MR imaging, which can be confounded by the anti-vascular effects of the drug (4). The failure to demonstrate efficacy may have been due to the use of an unselected patient group; if early responders could be identified then improved efficacy in this group might be demonstrable. We investigated, in animal models of GB, whether changes in tumor lactate labelling following injection of hyperpolarized [1-13C]pyruvate might detect response to treatment more effectively than contrast agent-enhanced MRI.
MATERIALS AND METHODS Rats implanted orthotopically with U87 cells received i.v. Bevacizumab when tumors were >0.1 cm3 (25 mg Kg -1). Imaging with hyperpolarised [1-13C]pyruvate was performed prior to Bevacizumab administration, at 24 hours following initial treatment and after 7 days, when a second dose of Bevacizumab was administered 24 hours prior to imaging. Two cohorts of patient-derived orthotopic xenografts (PDOX) were also used. In the first cohort, the protocol was similar to that described above. Several studies with Bevacizumab in GB have shown that treatment escape occurs through the promotion of an invasive phenotype (5,6). Therefore, in the second cohort of rats, when the tumors had reached >0.01 cm3, the animals were treated weekly with Bevacizumab. This was continued for 10 weeks, after which time the animals were imaged with hyperpolarised [1-13C]pyruvate.
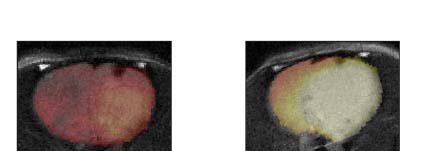
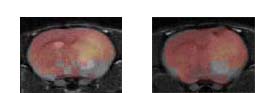
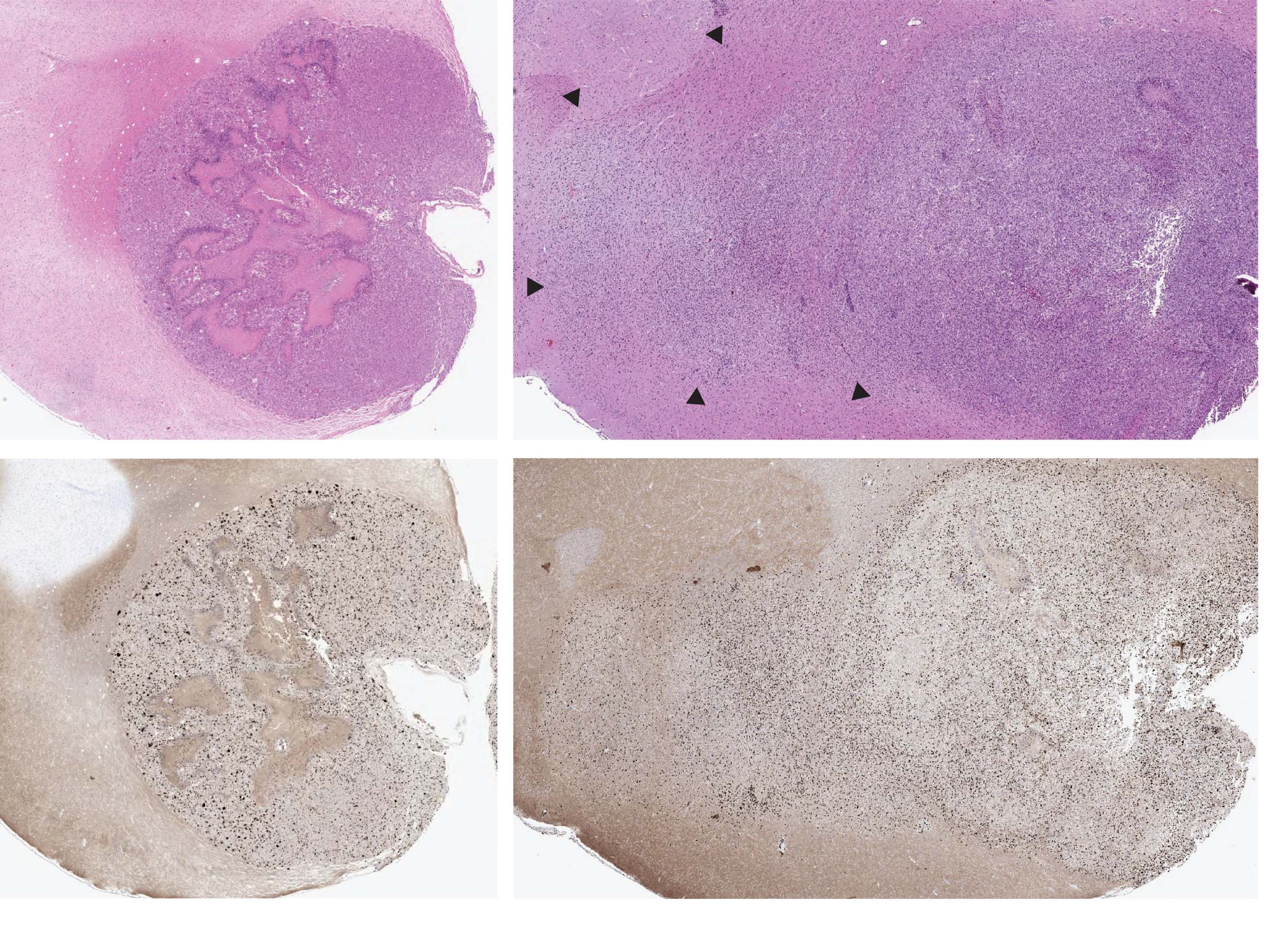
RESULTS 13C chemical shift images were acquired from U87 tumors (n=9), all of which demonstrated contrast enhancement on pre-Bevacizumab T1-weighted images. A significant increase in the hyperpolarized [1-13C]lactate/[1-13C]pyruvate ratio (LPR) was observed at 24 hours (n=5, p=0.003, mean LPR increase 0.12±0.07) and 7 days (n=9, p=0.0012, mean LPR increase 0.22±0.13) after treatment with Bevacizumab, which was associated with a slight decrease in contrast agent enhancement (Fig. 1). Next, we investigated the patient-derived orthotopic xenograft model. In contrast to what was observed in the U87 cell line model, a reduction in LPR was observed at both 24 hours and 7 days following treatment (ANOVA n=2, 2 time points, p=0.046, mean LPR decrease 0.05) (Fig. 2). In a second cohort of animals we started bevacizumab treatment when the tumours were >0.01cm3. This resulted in the development of an invasive phenotype (Fig. 3) (5) and again a statistically significant decrease in LPR following treatment (n=3, p=0.0006, Mean LPR in untreated tumors: 0.27±0.06, mean LPR in treated tumors: 0.09±0.03).
DISCUSSION Bevacizumab is commonly used as second line ‘salvage’ therapy for recurrent GB (1-3). The results presented here demonstrate that response to Bevacizumab, detected using imaging with hyperpolarised [1-13C]pyruvate in animal models of the disease, depends upon the tumor model. U87 is fast growing and lacks many features of GB, including adequate vascularization. Following treatment with Bevacizumab U87 tumours showed a significant increase in lactate labelling. In a biologically more apposite model of GB, treated with the same Bevacizumab dose regime, the opposite was the case. In this model, with a 4-month latency from implantation to experiment, a reduction in lactate labeling was observed following treatment. This was also observed in animals treated with Bevacizumab, when treatment was started when the tumors first appeared (<0.01 cm3). These tumors developed a highly infiltrative tumors (5,6) that also showed a significant reduction in lactate labeling following Bevacizumab treatment. A previous study of the effects of VEGF blockade in colorectal xenografts showed a decrease in lactate labeling in tumors that were sensitive to the drug, which correlated with decreased perfusion, and an increase in tumors that were less sensitive, which was attributed to vascular normalization and improved delivery of hyperpolarized [1-13C]pyruvate (7). Further studies using contrast agent-enhanced MRI are needed to determine whether this explanation also applies to the GB models used here.
CONCLUSION The response of GB tumor models to Bevacizumab treatment, detected using imaging with hyperpolarized [1-13C]pyruvate, varied depending on the tumor model. In tumors that more accurately model the human disease there was a decrease in lactate labeling that may reflect decreased perfusion. Imaging with hyperpolarized [1-13C]pyruvate may be no better therefore than contrast agent-enhanced MRI in detecting PFS.
Acknowledgements
The authors acknowledge the support of the Cancer Research UK Cambridge Institute core facilities, in particular the biological resources unit. The work was supported by a Cancer Research UK Programme grant (17242) and by the CRUK-EPSRC Imaging Centre in Cambridge and Manchester (16465) awarded to K.M. Brindle. R. Mair was supported by Addenbrooke's Charitable Trust and a CRUK Cambridge Centre Fellowship.References
1. Herrlinger, U. et al. Bevacizumab Plus Irinotecan Versus Temozolomide in Newly Diagnosed O6-Methylguanine-DNA Methyltransferase Nonmethylated Glioblastoma: The Randomized GLARIUS Trial. Journal of Clinical Oncology 34, 1611–1619 (2016).
2. Chinot, O. L. et al. Bevacizumab plus Radiotherapy–Temozolomide for Newly Diagnosed Glioblastoma. N Engl J Med 370, 709–722 (2014).
3. Gilbert, M. R. et al. A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma. N Engl J Med 370, 699–708 (2014).
4. Jain R.K. et al. Lessons from phase III clinical trials on anti-VEGF therapy for cancer. Nat Clin Pract Oncol. 3(1):24-40 (2006)
5. Keunen, O. et al. Anti-VEGF treatment reduces blood supply and increases tumor cell invasion in glioblastoma. Proc. Natl. Acad. Sci. U.S.A. 108, 3749–3754 (2011).
6. de Groot, J. F. et al. Tumor invasion after treatment of glioblastoma with bevacizumab: radiographic and pathologic correlation in humans and mice. Neuro-Oncology 12, 233–242 (2010).
7. Bohndiek, S. E., et al. Hyperpolarized (13)C spectroscopy detects early changes in tumor vasculature and metabolism after VEGF neutralization. Cancer Research 72, 854–864 (2012).
Figures