4304
Differentiating Radiation Necrosis from Brain Tumor Using Hyperpolarized Carbon-13 Metabolic MRI1Radiology, Chonnam National University Hwasun Hospital, Hwasun, Korea, Republic of, 2Radiology, Chonnam National University Medical School and Hospital, Gwangju, Korea, Republic of, 3Radiation Oncology, University of California San Francisco, San Francisco, CA, United States, 4Quantitative Medical Imaging Section, National Institute of Biomedical Imaging and Bioengineering, Bethesda, MD, United States, 5Neurosurgery, Chonnam National University Hwasun Hospital, Hwasun, Korea, Republic of
Synopsis
The differentiation of recurrent tumor from radiation necrosis after radiation therapy remains often challenging in patients with brain tumor despite various advanced MR imaging techniques. The purpose of this study was to explore the feasibility of hyperpolarized 13C metabolic imaging in differentiating brain tumor from radiation necrosis. The lactate signal in radiation necrosis model was significantly lower than that in glioma and lung cancer metastasis. This suggests that the non-invasive characterization of real-time metabolism using this new neuroimaging method may be helpful for differentiating radiation-induced necrosis from recurrent brain tumors.
Introduction
The differentiation of recurrent tumor from radiation necrosis after radiation therapy remains often challenging in patients with brain tumor despite various advanced MR imaging techniques. Hyperpolarized (HP) carbon-13 (13C) MR metabolic imaging is a promising new technology that provides a sensitive imaging approach for the noninvasive assessment of real-time in vivo metabolism. The purpose of this study was to explore the feasibility of HP 13C metabolic imaging in differentiating brain tumor from radiation necrosis.Methods and Materials
Radiation necrosis model was created by an 80-Gy single-dose irradiation of a half of the cerebrum in female F1 hybrid (C57BL/6+129Sv) mice (n=7) using a small animal irradiation system (Xstrahl, UK). Two brain tumor models were created by intracranial injections of 2 cells into the brains of female C57BL/6 mice: 1) glioma model with GL261 cell line (n=6) and 2) Lewis Lung carcinoma (LLC) metastasis model with LLC cells (n=7). The mice with radiation necrosis model developed contrast enhancing lesion approximately 2-3 months after irradiation and the 13C metabolic imaging data were obtained from them at 89±16 days after irradiation. The mice with brain tumor models were imaged at 14±2 days after tumor implantation. All experiments were performed using a GE clinical 3T scanner with a 13C/1H dual mouse coil (RAPID biomedical, Rimpar, Germany). 18µL of [1-13C]pyruvate (with 1.5mM gadolinium) was polarized using a HyperSense DNP polarizer (Oxford Instruments, Abingdon, UK)1. Compressed sensing 13C 3D MR spectroscopic imaging (MRSI) data2 were acquired from mice presenting either radiation necrosis or brain tumors at 20s from the start of the injection of 300µL HP 13C1-pyruvate through tail vein. The final dissolved solution had a concentration of 100 mM pyruvate and pH of 7.5. The lactate and pyruvate were normalized by the maximum total carbon signal in vasculatures (nLac and nPyr, respectively) and the ratio of lactate to pyruvate (Lac/Pyr) was evaluated. 13C parameters in contrast enhancing lesion were compared between the radiation necrosis and the two brain tumor models using an unpaired t-test.Results and Discussion
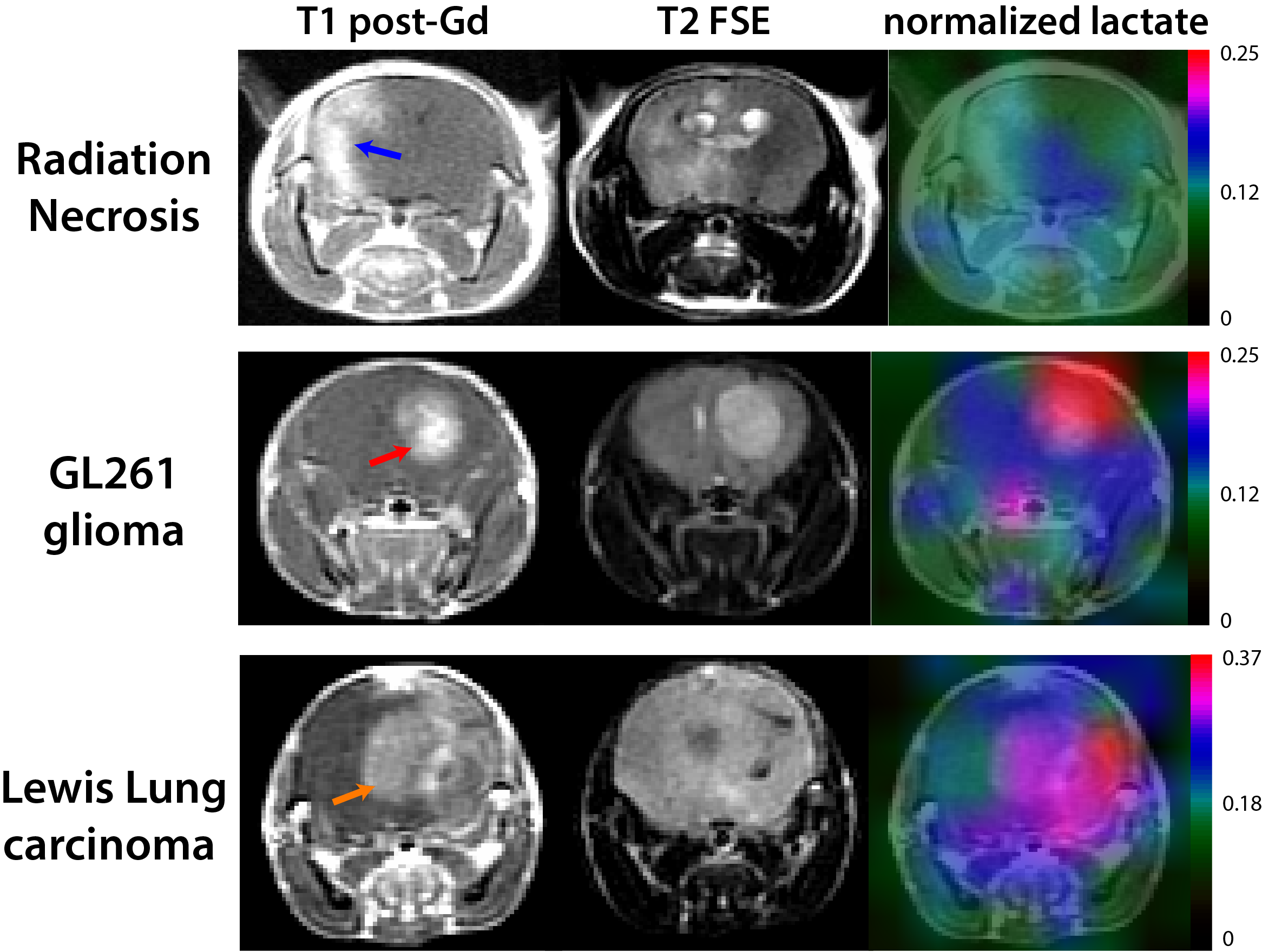
Conventional MRI exhibited typical radiographic features of radiation necrosis and brain tumor: MRI characteristics on conventional T2-weighted and Gd-enhanced T1-weighted images demonstrated typical radiographic findings from radiation necrosis and brain tumor models. The irradiated mice developed large lesions that had high Gd enhancement on post-contrast T1-weighted images and were heterogeneous on the T2-weighted images (top row in Fig 1). Similarly, the GL261 glioma exhibited Gd-enhancement on the T1-images and hyperintensity on T2-images (middle row in Fig 1). The LLC metastasis models showed relatively heterogeneous levels of enhancing and hyperintense lesions (bottom row in Fig 1).
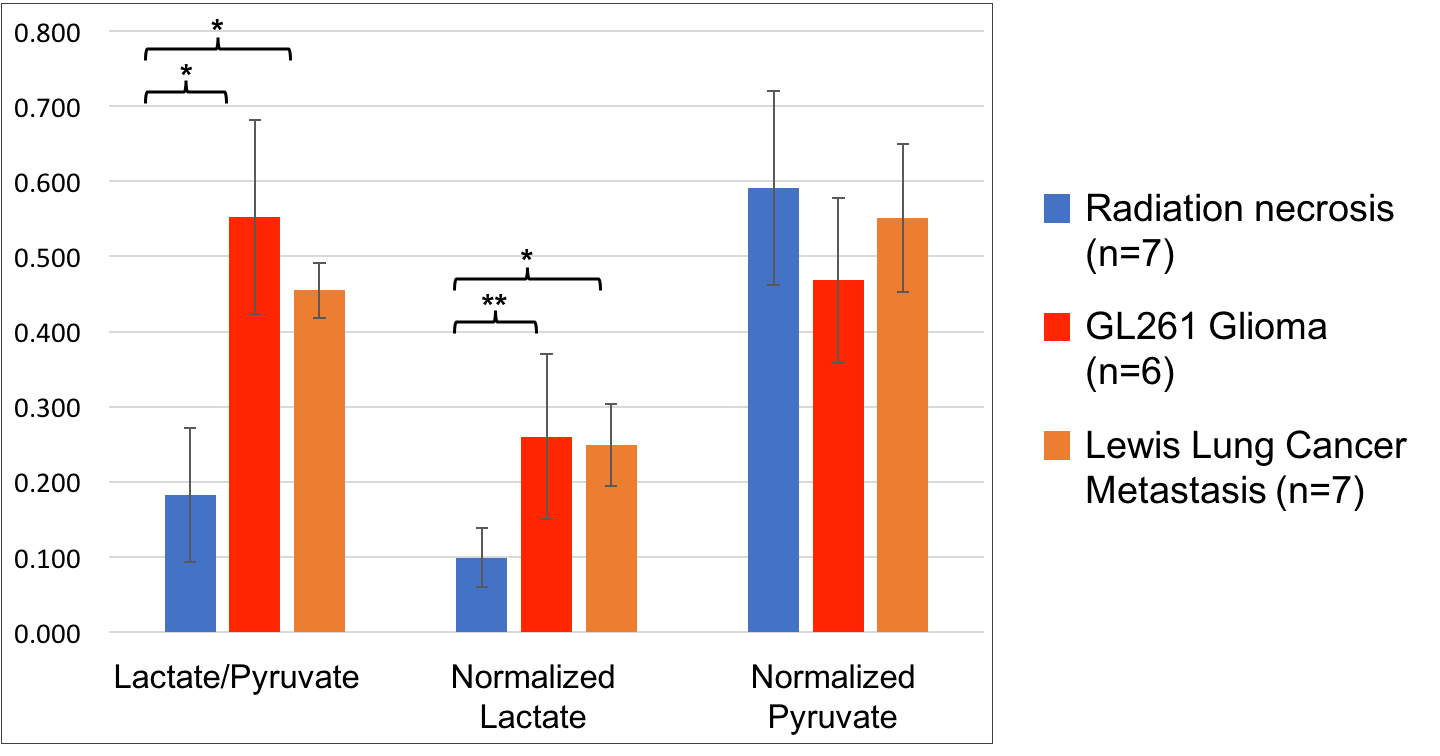
HP 13C MRSI indicated that radiation-induced necrotic tissue and brain tumors had distinct metabolic characteristics: The last columns in Figure 1 show the map of lactate normalized by vascular total carbon signal for the radiation necrosis, GL261 glioma and LLC metastasis models. They revealed a distinctive metabolic profile between radiation-induced and brain tumor tissue. The blue, red and orange arrows in Figure 1 indicate contrast-enhancing lesions for the radiation injury, GL261 glioma and LLC metastasis models, respectively. HP 13C MR metabolic imaging date showed that Lac/Pyr in radiation-induced injury was significantly lower than that in mouse glioma (0.18 versus 0.55, p<0.0001) and LLC metastatic tissue (0.18 versus 0.46, p<0.00001) (Fig 2). nLac in radiation necrosis models was also significantly lower than that in GL261 glioma (0.10 versus 0.26, p<0.01) and LLC metastasis model (0.10 versus 0.25, p<0.0001). There was no significant difference in nPyr between the radiation-induced injury and either GL261 glioma or LLC metastasis models (p>0.05), implying that the amount of pyruvate taken up by the three types of tissue were similar (Fig.2).
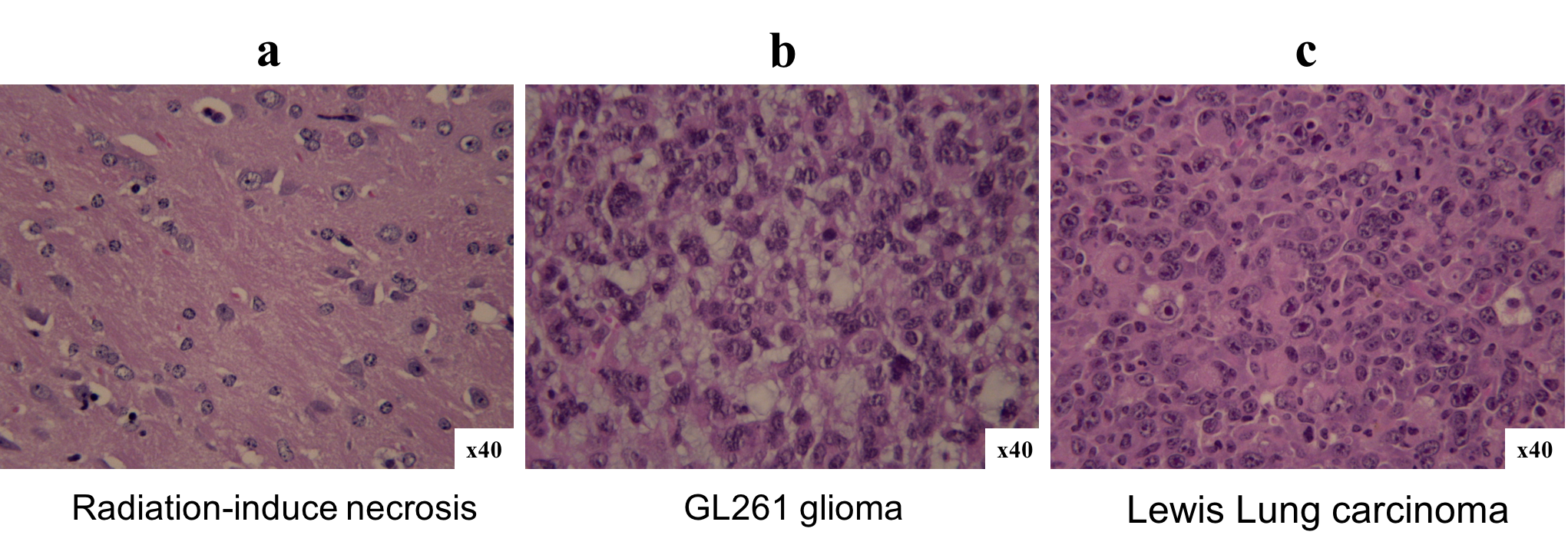
Histological analysis demonstrated distinct characteristics between the radiation-induced necrosis and brain tumors: Figure 3 is examples of H&E slides from radiation necrosis (Fig 3a), GL261 glioma (Fig 3b) and LLC (Fig 3c) models. In contrast to the radiation-induced necrotic tissue, both tumor models showed a high cell density, which is one of the characteristics of cancer. The increased level of cellularity in these tumors were consistent with the high level of Lac/Pyr and nLac observed in hyperpolarized 13C metabolic imaging data (Fig 2).
Conclusion
The results from this study suggest that hyperpolarized 13C metabolic imaging may provide a unique and noninvasive imaging biomarker for distinguishing recurrent glioblastoma from radiation necrosis.Acknowledgements
Support for the research came from a Discovery Grant from the American Brain Tumor Association, National Research Foundation (NRF) of Korea grant funded by Ministry of Science and ICT (No.2018R1C1B5018396), and grants from Chonnam National University Hospital Biomedical Research Institute (CRI18019-1 and CRI18094-2).References
1. Ardenkjaer-Larsen JH, Fridlund B, Gram A, et al. Increase in signal-to-noise ratio of > 10,000 times in liquid-state NMR. Proc Natl Acad Sci USA. 2003;100(18):10158-63.
2. Park I, Hu S, Bok R, et al. Evaluation of heterogeneous metabolic profile in an orthotopic human glioblastoma xenograft model using compressed sensing hyperpolarized 3D 13C magnetic resonance spectroscopic imaging. Magn Reson Med. 2012;70(1):33-9.
Figures