4293
Quadrature Transmit and Receive Array 13C RF Coil for Clinical Cardiac and Hepatic Imaging with Hyperpolarized 13C-Substrates1Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2Radiology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 3Electrical and Computer Engineering, University of Texas Dallas, Richardson, TX, United States, 4Clinical MR Solutions, Brookfield, WI, United States, 5GE Healthcare, Dallas, TX, United States, 6GE Healthcare, Toronto, ON, Canada, 7Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
A flexible torso 13C RF coil with quadrature transmit and 8-channel receive array that is designed for imaging cardiac and hepatic metabolism in humans was evaluated. B1+ field homogeneity and SNR were measured using phantoms. The torso coil had improved SNR and larger spatial coverage as compared to the conventional clamshell/paddle array coils.
Background
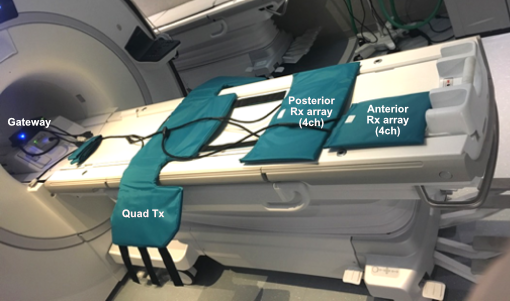
Combination of a clamshell transmit coil and two paddle-shaped receive array coils (GE Healthcare, 4 channel per paddle) has been used for imaging heart[1], liver and brain[2], [3] with hyperpolarized 13C MR. Although the transmit coil has a reasonably homogeneous excitation profile and the receive arrays provides decent sensitivities, application of the coils are often limited by multiple factors such as subject size and positioning, location of the target organs and patient discomfort, which are primarily due to the rigid design of the coils, fixed position of the clamshell coil, and limited receive depth of the paddle arrays. To improve sensitivity for 13C detection in the thorax and abdomen, a new torso coil (Clinical MR Solutions, LLC) has been developed to have a flexible design with larger receive coils. In particular, the receive arrays are divided to two separate pieces with different sizes (four 3”x7.2” arrays for anterior position, four 6”x8.5” arrays for posterior position), which has multiple possible configuration for optimal heart and/or liver imaging (Fig.1). In this work, we tested the torso coil performance with phantoms and a healthy volunteer.Methods
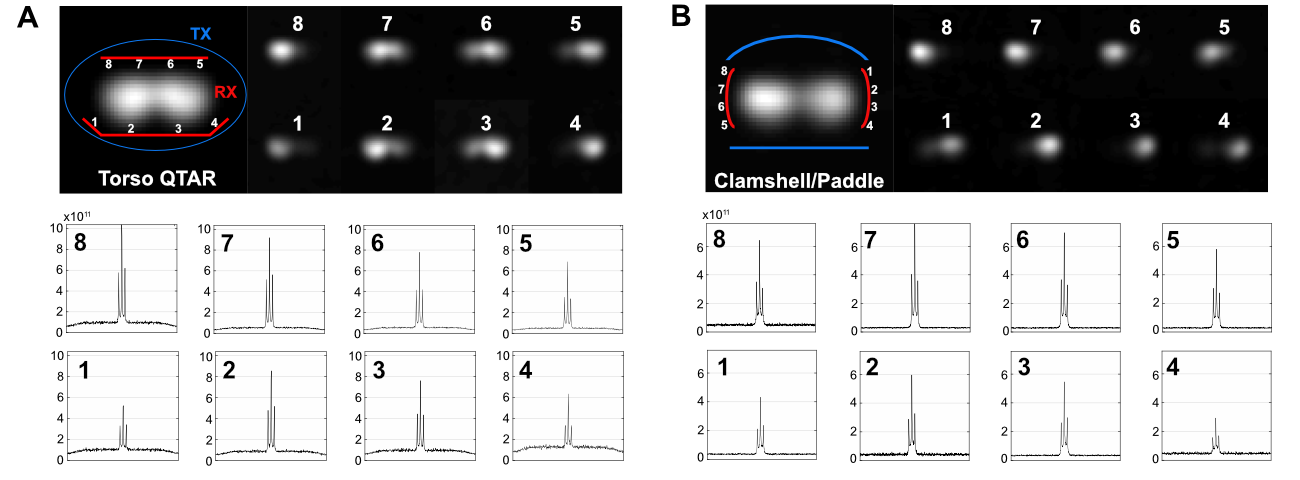
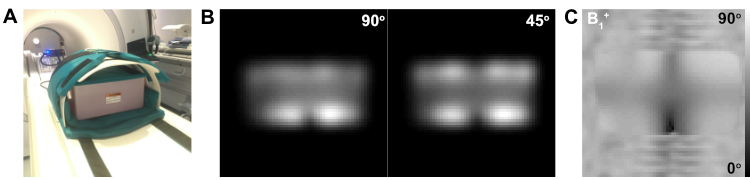
Two types of phantoms were used for coil tests: two cylindrical bottles that contain non-labeled pure ethylene glycol (35M, diameter = 13cm) and a non-labeled rectangular dimethyl silicon (GE Healthcare, size = 33 x 23 x 16 cm3, Gd-doped)[4]. First, the coil performance was tested with ethylene glycol phantoms at a clinical 3T MR scanner (GE healthcare, 750w) using two-dimensional free induction decay chemical shift imaging (FID CSI; flip angle = 90o, repetition time = 5s, matrix size = 16x16, field of view = 48x48cm2), and was compared with the results from the clamshell/paddle coils. In a separate test, B1+ profile was also measured using the dimethyl silicon phantom and the 2D FID CSI sequence and a double-angle method. Finally, the coil was tested with a healthy subject without any injection of hyperpolarized solution. All the data were processed using MATLAB. Magnitude images were reconstructed from integrated 13C peaks with baseline subtraction.Results and Discussion
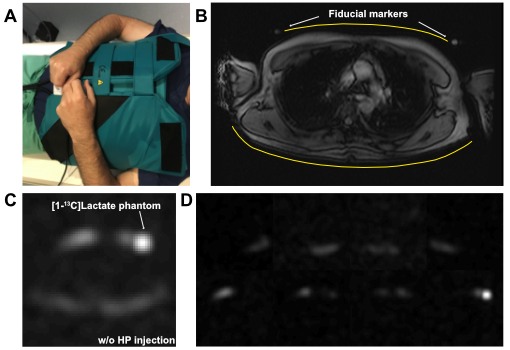
Figure 1 shows four separate elements of the 13C torso coil: a wearable flexible quadrature birdcage transmit coil (vest design), 4-channel posterior receive arrays, 4-channel anterior receive arrays, and a gateway. Figure 2 summarizes the FID CSI data acquired from (A) the torso coil and (B) the clamshell/paddle coils, showing both coil-combined images and images from individual channels. From the coil combined images, significantly higher signals were detected from the torso coil compared to the clamshell/paddle coils but also higher noise levels were noted from the torso coil. The peak SNRs (near the receive coils) were comparable between the coils (1329 for torso and 1469 for paddles). However, the SNR at the center of each phantom was significantly higher from the torso (1172) than the clamshell/paddles (882). Note that the spectra of the torso coil data (Fig. 2A) are in different scale (0-10x1011) from those of clamshell/paddle coils data (Fig. 2B, 0-8x1011). The B1+ field was estimated from the magnitude images of the dimethyl silicon phantom acquired using FID CSI (90o vs. 45o), Figure 3. The transmit gain was calibrated using a separate scan using a 6-M [1-13C]lactate syringe (diameter = 1cm) positioned at the center of the torso coil. While the B1+ was approximately correct at the center of the phantom, elevated B1+ was observed near the edge of the phantom. The torso coil was tested with a healthy subject (Fig. 4) as a final safety check out. No discomfort was reported by the subject even with the relatively large body size (186 cm tall, 88 kg body weight). A 6-M lactate phantom was positioned under the anterior receive arrays for transmit gain calibration. With absence of hyperpolarized 13C signal, subcutaneous lipids peaks were detected (coil-combined – Fig.4C, individual coils – Fig.4D).Conclusion
We demonstrated that the new flexible torso 13C coil with quadrature transmit and 8-channel phased receive has a number of advantages. First, SNR is increased and the coil offers wider coverage than the conventional 13C clamshell transmit and 8-channel paddle array coils. Second, this torso coil is more comfortable and less bulky which will be advantageous for claustrophobic patients. Finally, it allows convenient positioning of the subject anywhere on the magnet axis.Acknowledgements
Funding: National Institutes of Health of the United States (P41 EB015908, S10 OD018468); The Mobility Foundation; The Texas Institute of Brain Injury and Repair.References
[1]. C. H. Cunningham, J. Y. Lau, A. P. Chen, B. J. Geraghty, W. J. Perks, I. Roifman, G. A. Wright, and K. A. Connelly, “Hyperpolarized 13C metabolic MRI of the human heart: initial experience.,” Circ. Res., vol. 119, no. 11, pp. 1177–1182, Sep. 2016.
[2]. I. Park, P. E. Z. Larson, J. W. Gordon, L. Carvajal, H.-Y. Chen, R. Bok, M. Van Criekinge, M. Ferrone, J. B. Slater, D. Xu, J. Kurhanewicz, D. B. Vigneron, S. Chang, and S. J. Nelson, “Development of methods and feasibility of using hyperpolarized carbon-13 imaging data for evaluating brain metabolism in patient studies.,” Magn Reson Med, Jan. 2018.
[3]. V. Z. Miloushev, K. L. Granlund, R. Boltyanskiy, S. K. Lyashchenko, L. M. DeAngelis, I. K. Mellinghoff, C. W. Brennan, V. Tabar, T. J. Yang, A. I. Holodny, R. E. Sosa, Y. W. Guo, A. P. Chen, J. Tropp, F. Robb, and K. R. Keshari, “Metabolic Imaging of the Human Brain with Hyperpolarized 13C Pyruvate Demonstrates 13C Lactate Production in Brain Tumor Patients.,” Cancer Res., p. canres.0221.2018, May 2018.
[4]. T. Skloss, “Phantom fluids for high field MR imaging.,” Intl Soc Magn Reson Med, #1635, 2004.
Figures