4278
Investigating Pre-Saturation of Inflowing Lactate for Improving Human Hyperpolarized 13C-Pyruvate Brain Studies1UCSF, San Francisco, CA, United States
Synopsis
Dissolution dynamic nuclear polarization has enabled real-time metabolic imaging in both pre-clinical and clinical research applications. However, pre-clinical studies have provided evidence that inflowing metabolites can bias measurements in a number of organs. In this work, we explored the impact of inflowing lactate spins on quantitative hyperpolarized pyruvate 13C MRI of the human brain in a healthy volunteer. We provide evidence in a healthy volunteer that by pre-saturating inflowing lactate to address this confounding factor, kPL values in the brain were reduced by ~15%. Further studies will increase the sample size to better characterize this effect.
Introduction
Dissolution dynamic nuclear polarization1 has enabled real-time metabolic imaging in both pre-clinical and clinical research applications2-4. Towards the end stage of glycolysis, pyruvate has been shown to detect metabolic reprogramming in human cancers that demonstrate increased pyruvate-to-lactate conversion via up-regulated lactate dehydrogenase expression. The increased conversion of pyruvate to lactate, an outcome of the aberrant reliance on aerobic glycolysis, is a phenomenon known as the Warburg Effect and is a hallmark of advanced and malignant cancers.
However, pre-clinical studies have provided evidence that inflowing metabolites, chiefly lactate, can bias measurements of cardiac5 and renal metabolism6. Inflowing lactate could potentially lead to similar bias in clinical studies of cerebral metabolism, resulting in reduced contrast and overestimation of lactate production, and could also obfuscate ADC measurements in diffusion weighted 13C experiments because of a surfeit of extracellular, extravascular lactate.
In this work, we explored the impact of inflowing lactate spins on quantitative hyperpolarized pyruvate 13C MRI of the human brain. By using a spectral-spatial saturation pulse centered on the carotid arteries, inflowing lactate spins can be selectively suppressed and the magnitude of this effect on measurements of apparent pyruvate-to-lactate conversion in the brain can be measured.
Methods
Studies were performed on a 3T scanner (MR750, GE Healthcare) with clinical performance gradients (5 G/cm max gradient, 20 G/cm/ms max slew-rate). [1-13C]pyruvate was polarized in a 5T SPINlab polarizer (GE Healthcare) for over two hours. Following rapid dissolution, the pH, radical and pyruvate concentrations, polarization, and temperature were measured prior to injection.
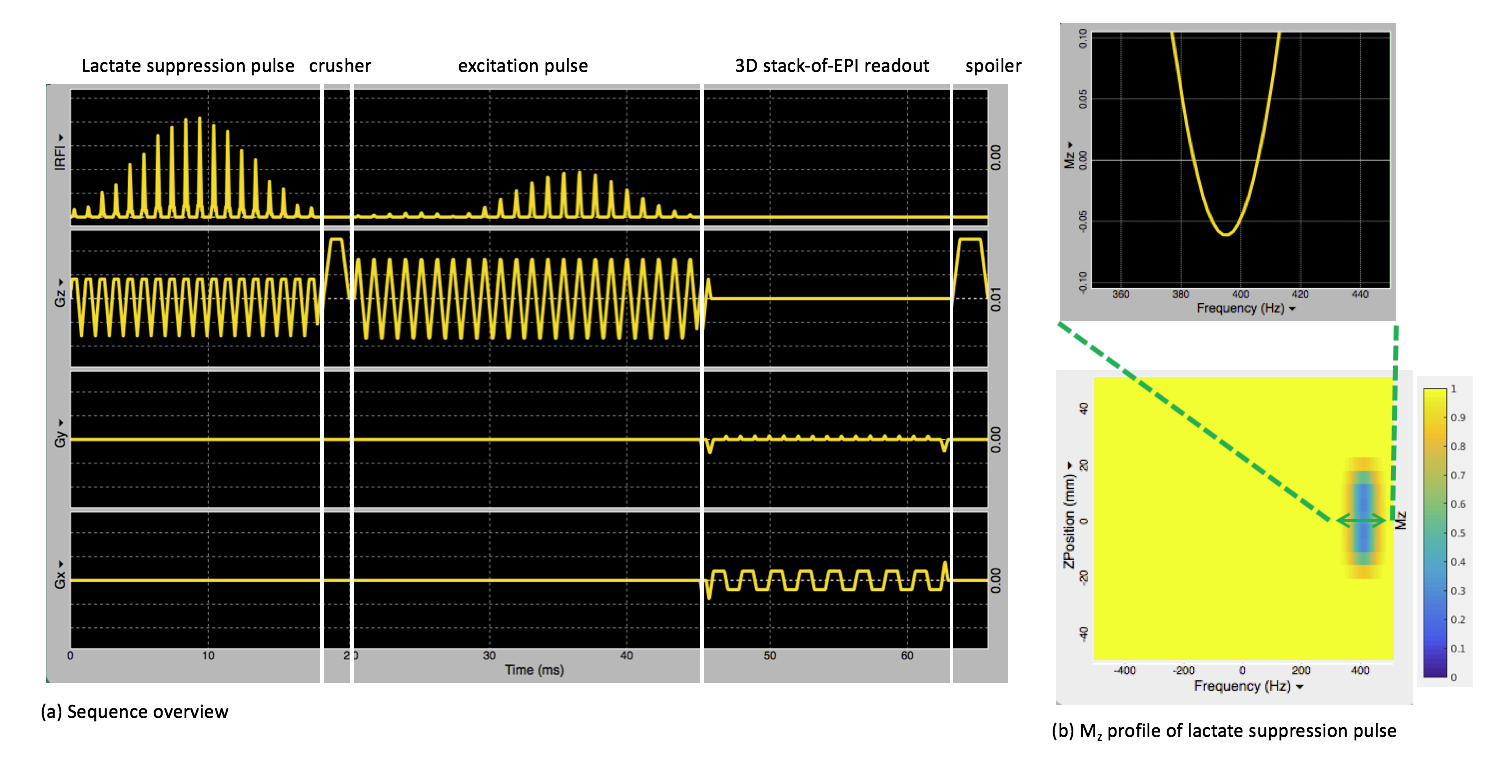
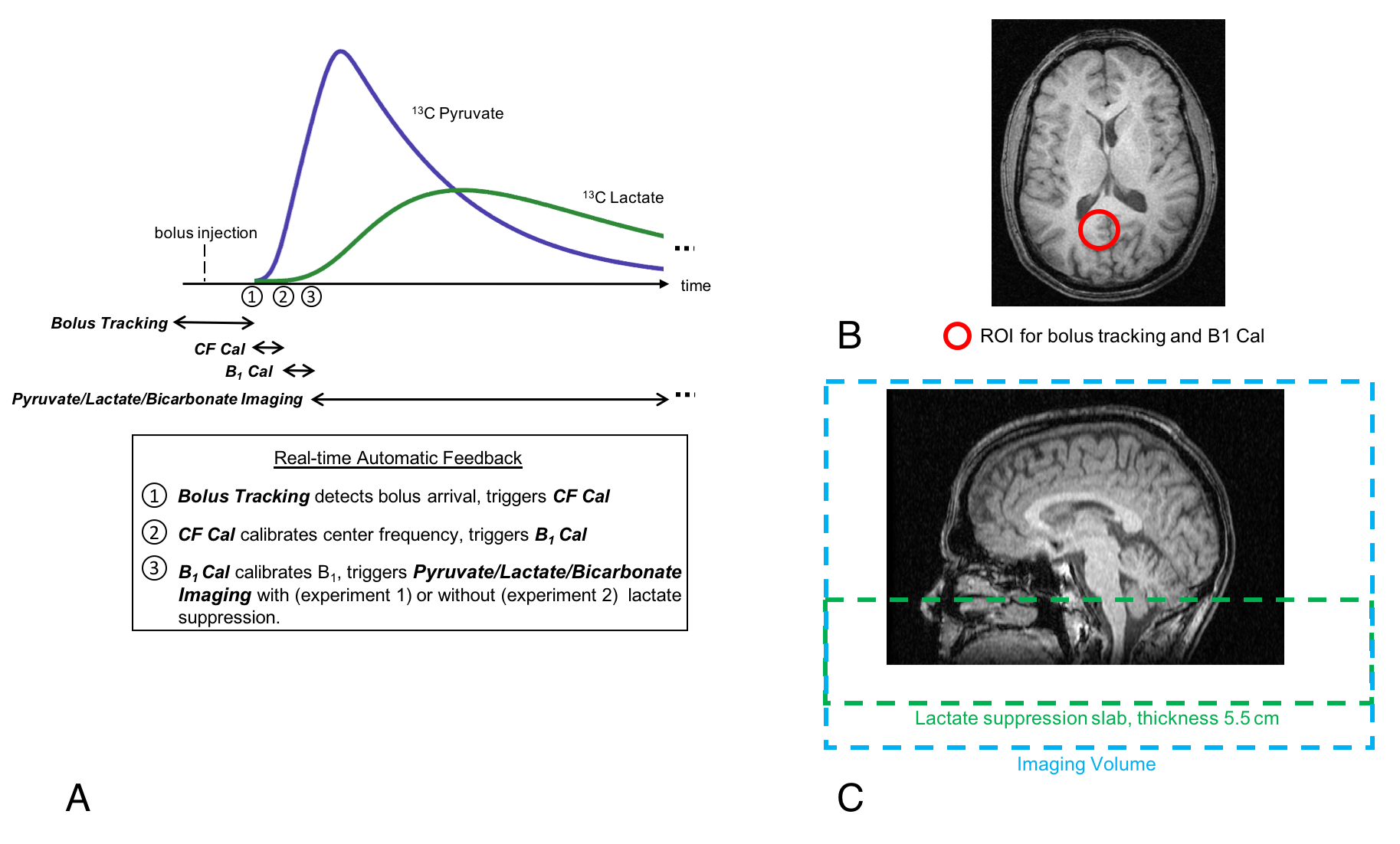
Two injections of hyperpolarized [1-13C]pyruvate were performed – the first used a spectral-spatial RF pulse to selectively saturate inflowing lactate spins, while the second did not. All other scan parameters remained identical. Data were acquired with a 3D metabolite-specific imaging sequence using a stack-of-EPI acquisition (Fig. 1). Bolus tracking during the injection was performed to calibrate the center frequency and RF power using the RT-Hawk platform7 (HeartVista). Prior to the human experiment, phantom studies were performed to ensure the lactate suppression pulse would not affect signal outside of the suppression slab. The relative power between the center of the brain coil and the suppression slice was calculated based on a B1 map acquired on the phantom to account for B1 drop-off at the edge of the coil. For the lactate suppression experiment, a 5.5cm slab covering the carotid arteries was placed 10cm inferior to the brain and was employed every TR to ensure sufficient saturation8 (Fig. 2). Scan parameters were 24ⅹ24ⅹ28 cm3 FOV, 16ⅹ16ⅹ14 matrix size, 71.4ms TR, 19.3ms TE, 3s temporal resolution, 5°/8°/8° flip angle for pyruvate, lactate and bicarbonate, respectively. Pyruvate-to-lactate conversion rate (kPL) was quantified based on a two-site exchange model using non-linear least-squares fitting9.
Results & Discussion
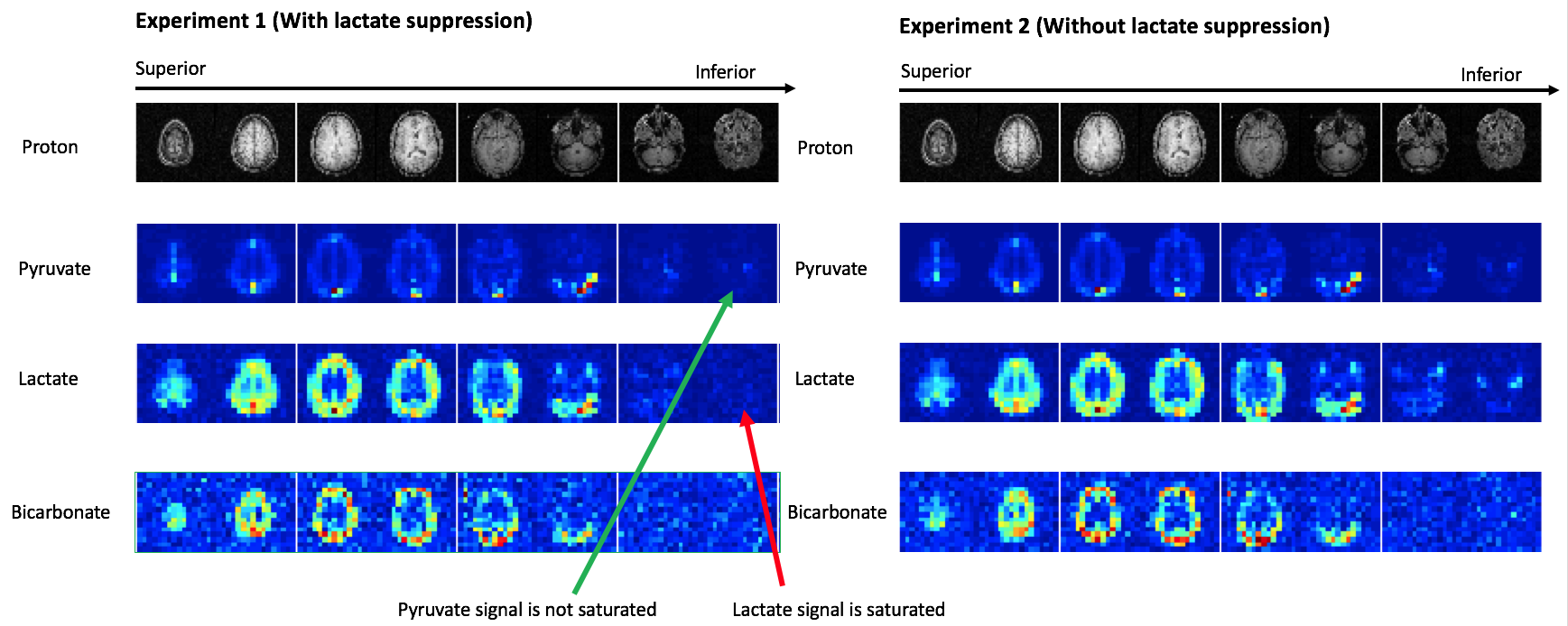
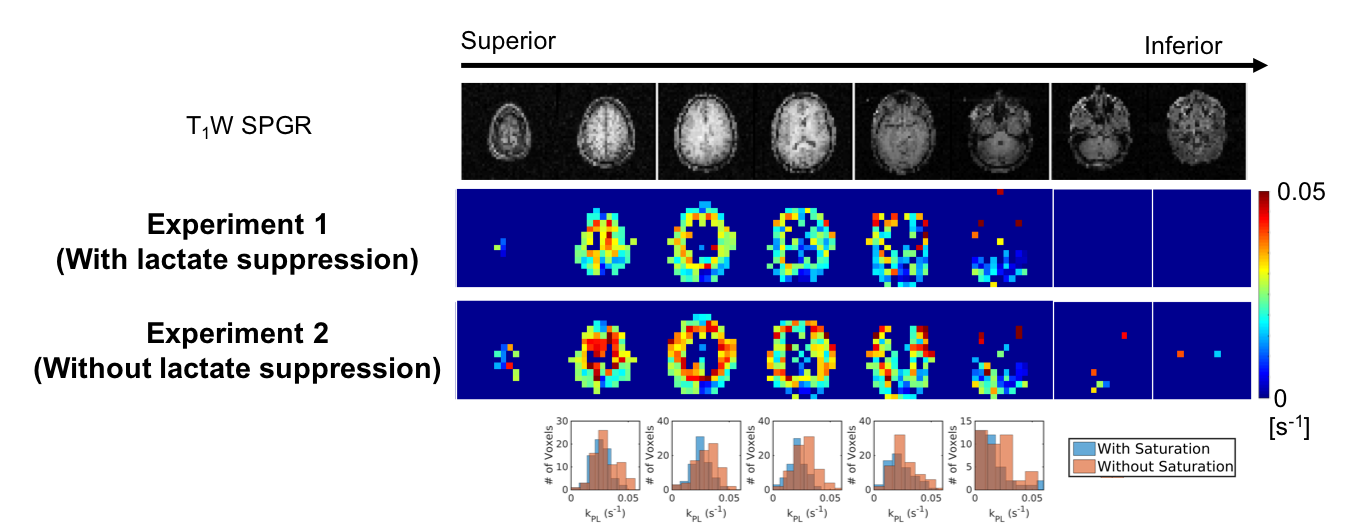
Sum-over-time 13C brain images were presented in Fig. 3. Lactate signal in the inferior slices were suppressed in the first experiment as expected due to overlap with the lactate suppression slab. Lactate signal in the superior slices, along with pyruvate and bicarbonate signals are not saturated by the lactate suppression pulse. Fig. 4 shows the apparent kPL of the two experiments. A mean 14.2% increase in kPL values were observed in the absence of lactate suppression (kPL = 0.0226 s-1 and 0.0258 s-1 with and without lactate suppression, respectively), particularly in interior, predominantly white matter voxels, indicating that inflowing lactate from the vasculature could lead to overestimated kPL. It is unclear if this is a difference in gray/white matter lactate metabolism or partial-volume effects with vascular lactate in cerebral arteries and will be explored in future studies. Future work will also focus on validating the reproducibility of this study and optimizing sequence parameters to improve bicarbonate SNR and calculate pyruvate-to-bicarbonate conversion rate (kPB).Conclusion
We provide evidence in a healthy volunteer that inflowing lactate spins can lead to ~15% higher kPL values in the brain. Further studies will increase the sample size to better characterize this effect.Acknowledgements
R01EB016741, P41EB013598, and American Cancer Society Research Scholar Grant 131715‐RSG‐18‐005‐01‐CCE.References
1. Ardenkjær-Larsen JH, Fridlund B, Gram A, Hansson G, Hansson L, Lerche MH, Servin R, Thaning M, Golman K. Increase in signal-to-noise ratio of > 10,000 times in liquid-state NMR. Proc Natl Acad Sci USA 2003;100(18):10158-10163.
2. Albers MJ, Bok R, Chen AP, Cunningham CH, Zierhut ML, Zhang VY, Kohler SJ, Tropp J, Hurd RE, Yen Y-F, Nelson SJ, Vigneron DB, Kurhanewicz J. Hyperpolarized 13C Lactate, Pyruvate, and Alanine: Noninvasive Biomarkers for Prostate Cancer Detection and Grading. Cancer Res 2008;68(20):8607-8615. 3. Cunningham CH, Lau JY, Chen AP, Geraghty BJ, Perks WJ, Roifman I, Wright GA, Connelly KA. Hyperpolarized 13C Metabolic MRI of the Human Heart: Initial Experience. Circulation Research 2016.
4. Nelson SJ, Kurhanewicz J, Vigneron DB, Larson PEZ, Harzstark AL, Ferrone M, van Criekinge M, Chang JW, Bok R, Park I, Reed G, Carvajal L, Small EJ, Munster P, Weinberg VK, Ardenkjaer-Larsen JH, Chen AP, Hurd RE, Odegardstuen L-I, Robb FJ, Tropp J, Murray JA. Metabolic Imaging of Patients with Prostate Cancer Using Hyperpolarized [1-13C]Pyruvate. Science Translational Medicine 2013;5(198):198ra108.
5. Wespi P, Steinhauser J, Kwiatkowski G, Kozerke S. Overestimation of cardiac lactate production caused by liver metabolism of hyperpolarized [1‐13C]pyruvate. Magn Reson Med. 2018;80:1882–1890.
6. Xu T, Mayer D, Gu M, Yen Y-F, Josan S, Tropp J, Pfefferbaum A, Hurd R, Spielman D. Quantification of in vivo metabolic kinetics of hyperpolarized pyruvate in rat kidneys using dynamic 13C MRSI. NMR in Biomedicine 2011;24(8):997-1005.
7. Tang S, Milshteyn E, Reed G, Gordon J, Bok R, Zhu X, Zhu Z, Vigneron DB, Larson PEZ. A regional bolus tracking and real-time B1 calibration method for hyperpolarized 13C MRI. Magnetic Resonance in Medicine 2018; https://doi.org/10.1002/mrm.27391
8. Harloff A, Zech T, Wegent F, Strecker C, Weiller C, Markl M. Comparison of Blood Flow Velocity Quantification by 4D Flow MR Imaging with Ultrasound at the Carotid Bifurcation. American Journal of Neuroradiology 2013;34(7):1407.
9. Larson PEZ, Chen H-Y, Gordon JW, Korn N, Maidens J, Arcak M, Tang S, Criekinge M, Carvajal L, Mammoli D, Bok R, Aggarwal R, Ferrone M, Slater JB, Nelson SJ, Kurhanewicz J, Vigneron DB. Investigation of analysis methods for hyperpolarized 13C-pyruvate metabolic MRI in prostate cancer patients. NMR in Biomedicine 2018;0(0):e3997.
Figures