4227
Retrospective Phase-Based Gating for Cardiac Proton Spectroscopy with Fixed Scan Time1Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland, 2Department of Cardiology, University Heart Center, University Hospital Zurich, Zurich, Switzerland, 3Department of Cardiology, Pneumology and Angiology, Heinrich Heine University Düsseldorf, Düsseldorf, Germany, 4Department for Cardiology, Pneumology and Angiology, Heinriche Heine University Düsseldorf, Düsseldorf, Germany, 5Institute of Diagnostic and Interventional Radiology, University Hospital Zurich, Zurich, Switzerland
Synopsis
Respiratory motion is a major limiting factor for the application of cardiac proton MR spectroscopy (MRS) in clinical settings. Prospective navigator gating is frequently applied to minimize respiratory motion effects. However, scan durations are subject-dependent and hence difficult to predict. The present work describes cardiac proton MRS with fixed scan time employing retrospective phase-based gating. It is demonstrated that, relative to prospective navigator gating, the phase-based gating approach provides comparable triglyceride-to-water ratios with predictable scan time.
Introduction
Proton MRS has shown promise of detecting changes of triglycerides (TG) and creatine in the in vivo heart for various cardiovascular diseases1.So far, however, cardiac 1H-MRS has not found its way into the clinical setting, primarily due to the time-consuming acquisition and technical demands. One of the major factors for signal degradation is respiratory motion. Previous studies have shown that double triggering on the ECG and on respiratory motion using prospective navigator gating on the hemidiaphragm is superior to other motion compensation techniques2. However, the efficiency of respiratory gating depends on the breathing pattern, which in turn results in unpredictable scan durations. The objectives of the present work were to implement cardiac proton MRS with fixed scan time by employing retrospective phase-based gating and to compare the proposed method to conventional navigator gating in healthy subjects.Methods
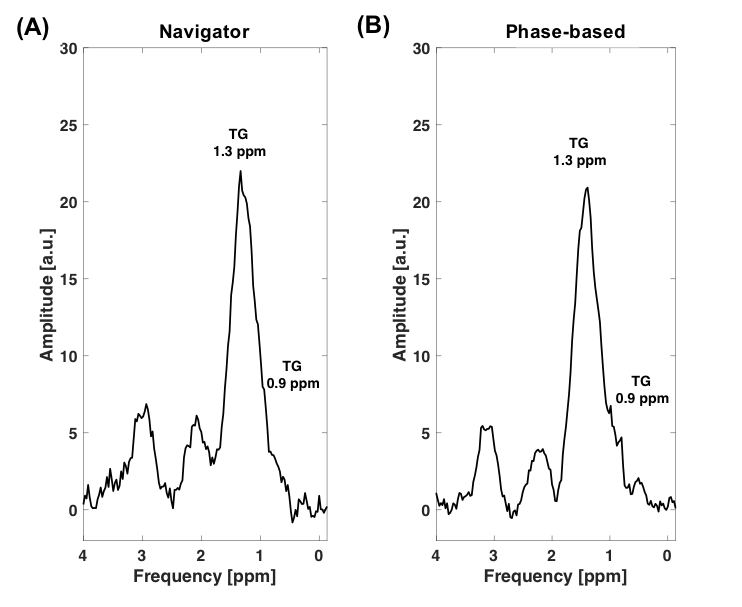
Cardiac proton MRS was performed on a 1.5T system (Achieva, Philips, Best, the Netherlands) using a 5-channel coil in 13 healthy subjects (6 male, mean age: 28.9±6.2 years). Cine steady-state free precession images in short-axis and 4-chamber view were obtained for planning purposes. After iterative volume shimming, voxels of 8 mL (4x2x1cm3) were placed in the interventricular septum. A PRESS (point-resolved spectroscopy) sequence (TE: 21 ms, TR: 2000 ms) was applied to acquire spectra in systole using (a) prospective navigator gating on the diaphragm (navigator window 4 mm) and (b) using free-breathing data collection without navigator gating and accepting all averages. In 5 subjects, the free-breathing scan was repeated to assess reproducibility. Data acquisitionwas ECG-triggered for all scans. A total of 96 averages with CHESS-based water suppression (WS) and 16 averages without WS were acquired for prospective gating whereas 304 averages with and 48 without WS were acquired for the phase-based gating approach. Data was post-processed in MATLAB using a customized reconstruction pipeline implemented in ReconFrame (GyroTools LLC, Zurich, Switzerland) (Fig.1). For phase-based gating, signal phases of the water and the main TG peak at 1.3ppm were extracted. These phases were preprocessed and normalized according to$$\phi^{*}_{i} = \frac{1}{N}\sum_{j=1}^{N}{\left\lvert\phi_{i}-\phi_{j}\right\rvert},\;\phi^{'}_{i}=\frac{\phi^{*}_{i}-min\left(\phi^{*}\right)}{max\left(\phi^{*}\right)}\;(1)$$with φi being the phase of a single water or TG average, i being a single average and N being the number of all averages. Afterwards, signals with normalized phases φ'i were selected according to different thresholds (phase thresholding, thresholds between 0.4-0.1) with higher thresholds indicating higher residual phase fluctuations. Subsets of averages for different thresholds as well as the best 16 averages without WS and 96 averages with WS were considered as separate data sets and entered into the post-processing pipeline (Fig.1).Signal intensities of all scans were obtained by fitting the spectra in the time-domain in jMRUI/AMARES3. TG resonances were fitted at 0.9 and 1.3 ppm, the unsuppressed water at 4.7 ppm (Fig.1). Data were corrected for T1- and T2-relaxation effects and the triglyceride-to-water ratio (TG/W) was calculated.
Results
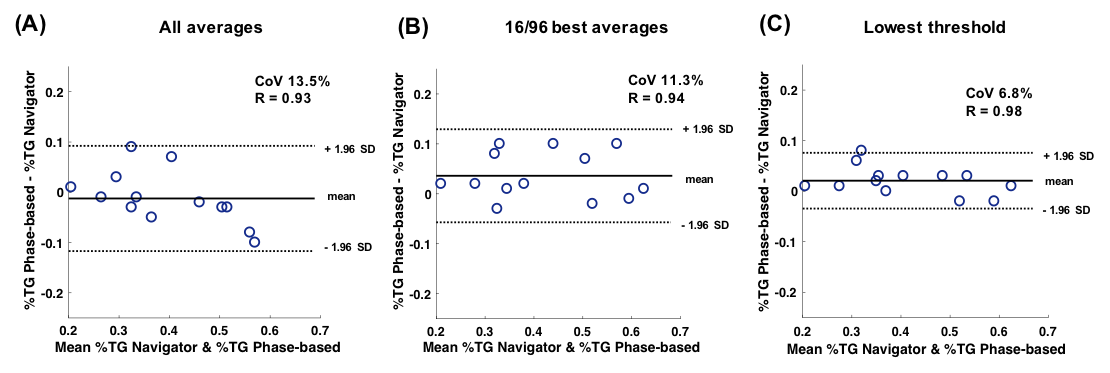
The duration of the prospective navigator-gated scans ranged from 381 to 1357s (mean gating efficiency 39±11%), while data acquisition for retrospective phase-based gating had a fixed scan time of 714s. At the lowest individual threshold for each subject (between 0.2&0.1), the average number of accepted signal averages without WS was 22.3±9.8 (47±20% efficiency) and the average number of accepted signal averages with WS 159.6±43.8 (53±14% efficiency). Residual water phase fluctuations of the lowest thresholds and the 16/96 best averages in each subject were significantly lower compared to water phase fluctuations obtained with prospective navigator gating (p<0.01 and p=0.02, Fig.2). The same observations were made regarding TG phase fluctuations. Standard deviation of the water amplitude decreased with lower thresholds as expected (Fig.3). The 16/96 best averages showed a coefficient of variance (CoV) of 11.3% whereas taking the lowest thresholds for each subject showed a CoV of 6.8% (Fig.4&5). In repeated TG measurements, CoV was 8.2% for the lowest threshold and 12.6% for the 16/96 best averages.Discussion
Using a fixed scan time and phase-based gating, good measurement reproducibility compared to prospective navigator gating could be achieved for cardiac proton MRS. The retrospective gating efficiency of the phase-based gating approach was higher when compared to the gating efficiency of the prospective navigator approach (53±14% vs. 39±11%). This finding may be explained by the indirect measurement of motion on the diaphragm using the pencil-beam navigator as opposed to direct detection of motion-induced signal distortions using the phase-thresholding approach. Of note, the three-dimensional nature of respiratory-induced motion of the heart may only be incompletely captured from one-dimensional navigator measurements4,5.Conclusion
Cardiac proton MRS employing retrospective phase-based gating is feasible and provides reproducible assessment of TG in a fixed scan time.Acknowledgements
References
1. Ewijk PA van, Schrauwen-Hinderling VB, Bekkers SCAM, Glatz JFC, Wildberger JE, Kooi ME. MRS: a noninvasive window into cardiac metabolism. NMR Biomed 2015;28(7):747–766.
2. Meer RW van der, Doornbos J, Kozerke S, Schär M, Bax JJ, Hammer S, Smit JWA, Romijn JA, Diamant M, Rijzewijk LJ, Roos A de, Lamb HJ. Metabolic imaging of myocardial triglyceride content: reproducibility of 1H MR spectroscopy with respiratory navigator gating in volunteers. Radiology 2007;245(1):251–257.
3. Vanhamme, Boogaart A van den, Huffel S Van. Improved method for accurate and efficient quantification of MRS data with use of prior knowledge. J Magn Reson 1997;129(1):35–43.
4. Heeswijk RB van, Bonanno G, Coppo S, Coristine A, Kober T, Stuber M. Motion compensation strategies in magnetic resonance imaging. Crit Rev Biomed Eng 2012;40(2):99–119.
5. Manke D, Nehrke K, Börnert P. Novel prospective respiratory motion correction approach for free-breathing coronary MR angiography using a patient-adapted affine motion model. Magn Reson Med2003; 50(1):122–131.
Figures
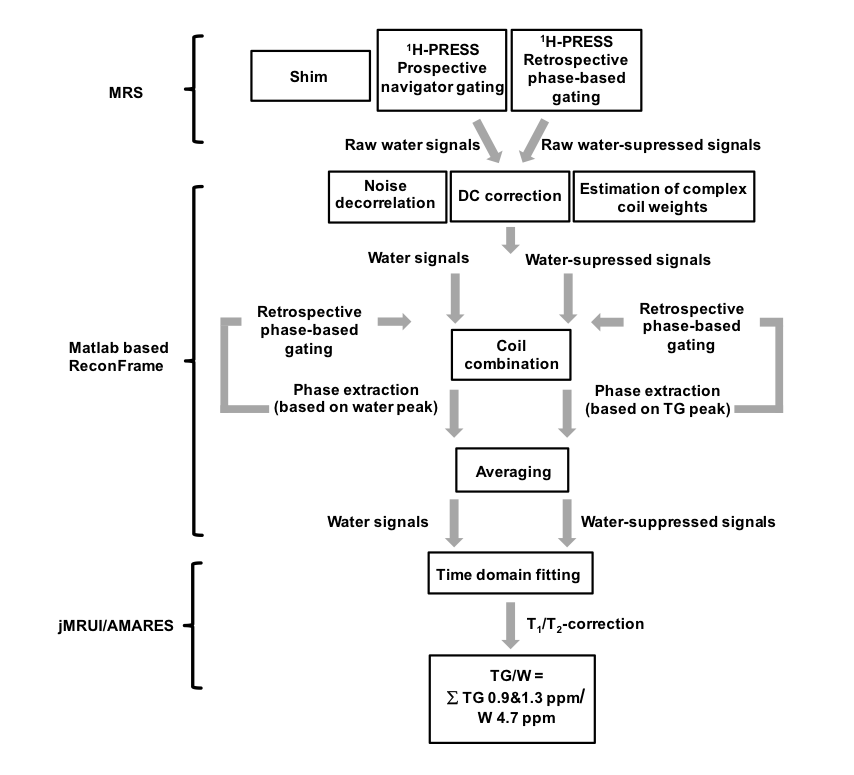
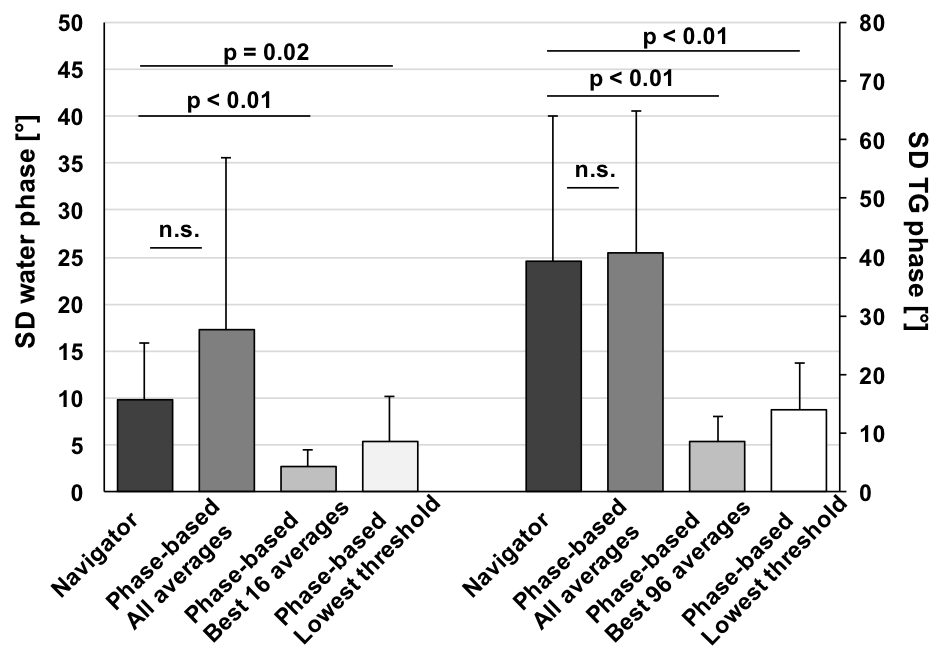
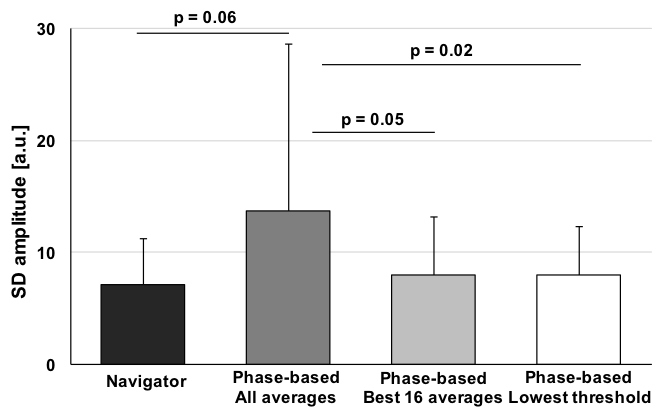
Figure 3: Standard deviation (SD) of water amplitude fluctuations for prospective navigator gating and retrospective phase-based gating accepting all averages, the best 16/96 averages or using the lowest threshold for each subject.