4212
Preliminary investigation into the effect of diuretic treatment on in vivo skin sodium using ultra-short echo time 23Na MRI at 3T with biopsy validation1Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 2Cancer Research UK Cambridge Institute, University of Cambridge, Cambridge, United Kingdom, 3Division of Experimental Medicine and Immunotherapeutics, University of Cambridge, Cambridge, United Kingdom, 4Department of Radiology, Addenbrooke's Hospital NHS Foundation Trust, Cambridge, United Kingdom, 5GE Healthcare, Munich, Germany
Synopsis
In this ongoing study, we investigate the changes in skin sodium concentration between controls and a group receiving a diuretic for seven days and present results from an interim analysis. Ultra-short echo time 23Na-MRI is performed at baseline and after seven days, at the end treatment. Results are correlated with measurements of sodium from biopsy samples.
Introduction
It has been postulated that the skin may serve as an extrarenal counter-current system.1 Previous studies investigating this have assessed changes in skin sodium due to haemodialysis1 ,diuretic treatment2, renal denervation3, chronic kidney disease4 and in systemic sclerosis patients5.These previous studies have used a gradient-echo sequence with echo times in the range of 2-3.5 ms1-9 which are sub-optimal to sample the short T2 component of tissue sodium (~0.5-5 ms).10 Here, we use a high resolution ultra-short echo time technique, which may provide a more accurate quantification of the total sodium concentration. Interim preliminary results are presented from an exploratory diuretic treatment study in healthy volunteers. 23Na-MRI quantification is being validated by comparing the results with biopsy measures.Methods
Participants subscribed to a randomised trial approved by the local ethics committee involving intake of either a placebo or thiazide-like diuretic (indapamide) for seven days. For the duration of the study, participants were self-managed on a medium salt diet (6 g per day). 23Na-MRI of the skin was performed on a subset (n=20) of these subjects at baseline and after treatment. Researchers were blinded to the trial randomisation. Skin sodium in the lower back was imaged on a clinical 3T system (GE MR750) using a bespoke 2cm diameter 23Na T/R coil. Imaging was performed with a 3D cones sequence11 and the following parameters: TE=0.46 ms, TR=100 ms, FOV=16x16x16 cm3, nominal resolution 1x1x10 mm3, 14730 total readouts, 250 kHz full receiver bandwidth, 24.5 minutes total acquisition duration. Coil sensitivity was corrected after image reconstruction.12 4% agar phantoms ranging from 7-160 mmol/l NaCl were used to construct a calibration curve for sodium quantification.13 Skin biopsies from the lower back (volume 5 mm3) were analysed using inductively coupled plasma-optical emission spectroscopy (ICP-OES) for comparison against 23Na-MRI measurements. At the time of the production of this abstract, the treatment randomisation un-blinding was unfortunately only available for the first eight subjects.Results
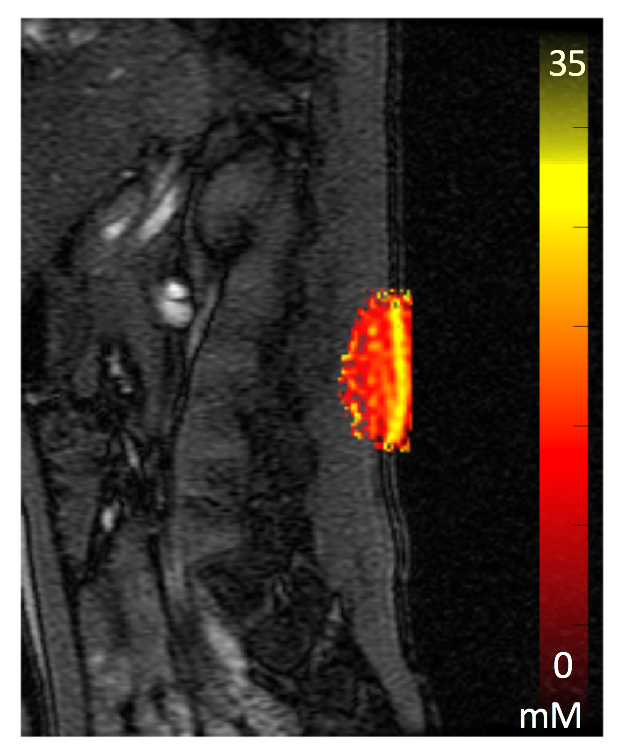
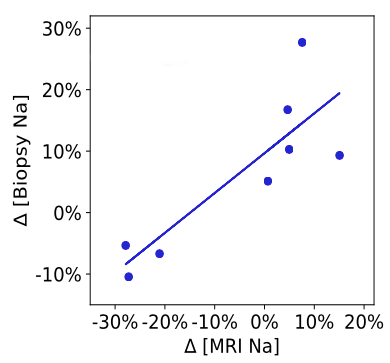
Figure 1 shows a 23Na image overlaid on a 1H T2-weighted image of the lower back from one of the subjects. Mean skin sodium concentration at baseline from all subjects (n=20) was 27.6 ± 2.7 mM. For the first eight subjects for which placebo vs. drug treatment was un-blinded, mean sodium concentration at the end of the study was 21.9 ± 4.0 mM for the diuretic group (n = 4) . Mean difference between the sodium at baseline and the end of study was 4 ± 7 % for the placebo group (n=4) and -24 ± 21 % for the diuretic group (p-value = 0.11, Wilcoxon). The percentage change difference observed on 23Na-MRI correlates well with the percentile difference obtained from biopsy (R2= 0.71), figure 2.Discussion and Conclusion
The concentration of sodium measured within the skin (mean = 27.6 ± 2.7 mM) is close to the range reported in previous studies (17 – 24.4 mM).1-9 Ultra-short echo time imaging generates results that are similar to those produced using gradient echo sequences with a longer TE. Further investigation into the actual T2* of skin is planned in the future, as well as short-term repeatability measurements. These results show a high repeatability of the skin sodium concentration in the placebo group, however there are a small number of outliers where the skin sodium measurement was increased by around 15%. The diuretic treatment group showed a marked reduction in the measured skin sodium, which provides evidence that the skin acts as a storage system for NaCl that can be perturbed by diuretics. However, this was not statistically significant with just 8 subjects for which treatment randomisation un-blinding was available at this time. Outliers may relate to dietary or treatment non-compliance that will be investigated. Indeed, one of the diuretic treatment subjects who did not show a reduction in skin sodium using MRI, did not show any reduction in the biopsy measure either. Full results with statistical analysis will be produced after the trial randomisation has been un-blinded for the remaining subjects (n = 12). This study demonstrates the feasibility to perform high-resolution 23Na-MRI of the skin at 3T. Compared to previous studies1-9 at 3T, voxel size was reduced by more than 25 times (1x1x10mm3 vs 3x3x30mm3). However, point spread function effects need to be considered, which do not affect gradient echo sequences used in the previous studies. Future analysis will correlate additional factors such as age, weight, sex and race, which have previously been shown to influence sodium measurements.8,9 23Na-MRI of the skin may offer a non-invasive test over skin biopsies that are both painful and carry the risk of infection. Assessing skin sodium may in general offer new insights and monitoring tools in renal and inflammatory diseases.Acknowledgements
FR is supported by the Engineering and Physical Sciences Research Council and Cancer Research UK. The project was supported by the Addenbrooke’s Charitable Trust, the NIHR comprehensive Biomedical Research Centre award to Cambridge University Hospitals NHS Foundation Trust in partnership with the University of Cambridge and the Cambridge Experimental Cancer Medicine Centre.References
1. Dahlmann A, Dörfelt K, Eicher F, et al. Magnetic resonance-determined sodium removal from tissue stores in hemodialysis patients. Kidney Int. 2015;87(2):434-441.
2. Hofmeister LH, Perisic S, Titze J. Tissue sodium storage: evidence for kidney-like extrarenal countercurrent systems? Pflugers Arch. 2015;467(3):551-558.
3. Hammon M, Grossmann S, Linz P, et al. 23Na Magnetic Resonance Imaging of the Lower Leg of Acute Heart Failure Patients during Diuretic Treatment. PLoS One. 2015;10(10):e0141336.
4. Ott C, Kopp C, Dahlmann A, et al. Impact of renal denervation on tissue Na+ content in treatment-resistand hypertension. Clin Res Cardiol. 2018;07(1):42-48.
5. Schneider MP, Raff U, Kopp C, et al. Skin Sodium Concentration Correlates with Left Ventricular Hypertrophy in CKD. J Am Soc Nephrol. 2017;28(6):1867-1876.
6. Kopp C, Beyer C, Linz P, et al. Na+ deposition in the fibrotic skin of systemic sclerosis patients detected by 23Na-magnetic resonance imaging. Rheumatology (Oxford). 2017;56(4):674.
7. Deger MS, Wang P, Fissell R, et al. Tissue sodium accumulation and peripheral insulin sensitivity in maintenance hemodialysis patients. J Cach Sarco Muscle. 2017;8(3):500-507.
8. Wang P, Deger MS, Kang H, et al. Sex differences in sodium deposition in human muscle and skin. Magn Reson Imaging. 2017;36:93-97.
9. Dyke JP, Meyring-Wösten A, Yhao Y, et al. Reliability and agreement of sodium (23Na) MRI in calf muscle and skin of healthy subjects from the US. Clin Imaging. 2018;52:100-105.
10. Madelin G, Regatte RR. Biomedical Applications of Sodium MRI In Vivo. J Magn Reson Imaging. 2013;38(3):511-529.
11. Gurney PT, Hargreaves BA, Nishimura DG. Design and Analysis of a Practical 3D Cones Trajectory. Magn Reson Med. 2006;55(3):575-582.
12. Axel L, Costantini J, Listerud J. Intensity correction surface-coil MR imaging. Am J Roentgenol. 1987;148:418-420.13. Christensen JD, Barrere BJ, Boada FE, et al. Quantitative tissue sodium concentration mapping of normal rat brain. Magn Reson Med.1996;36:83–89.
Figures