4186
Repeatability of measured RF transfer functions of IPG and lead based AIMD systems1Boston Scientific, Valencia, CA, United States
Synopsis
Lead heating and malfunction of implantable medical devices, such as Spinal Cord or Deep Brain Stimulators, due to MRI RF field exposure are patient safety concerns. The transfer function is a method used to calculate predictions of MRI-induced heating or injection voltages. This study investigated the repeatability of a measurement-based transfer function system. Results showed that the inherent variation of the system can be minimal, whereas lead positioning in the system has a higher impact on variation.
Introduction
The interaction of an active implantable medical device (AIMD) and the MRI RF field can cause patient harm due to RF-induced heating or RF-induced malfunction [1]. The transfer function is used for ISO/TS 10974 Tier 3 based modeling to predict the in-vivo lead temperature rise and injection voltage of a pulse generator with lead(s) system [1]. The transfer function can be measured in different ways, or simulated, depending on the complexity of the AIMD lead [2, 3]. We investigated the repeatability of a measurement-based system by repeating data acquisition with and without remounting the AIMD to assess the contribution of the overall system versus AIMD positioning in the test set-up to transfer function variation.Methods
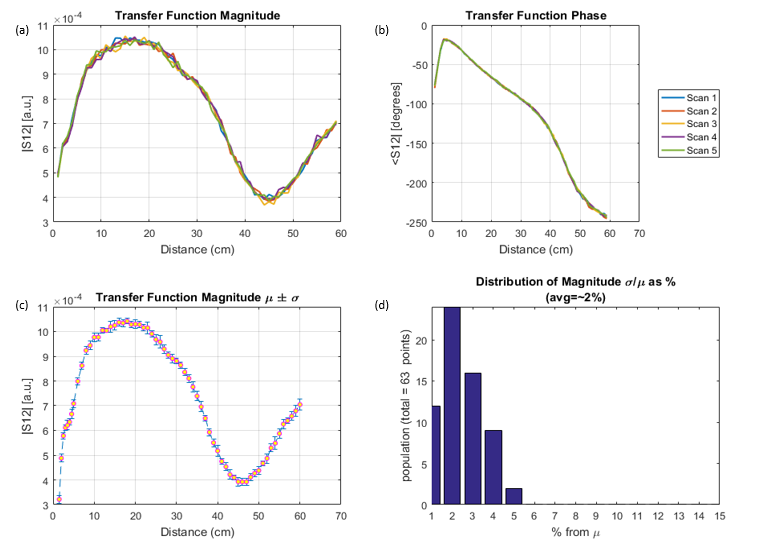
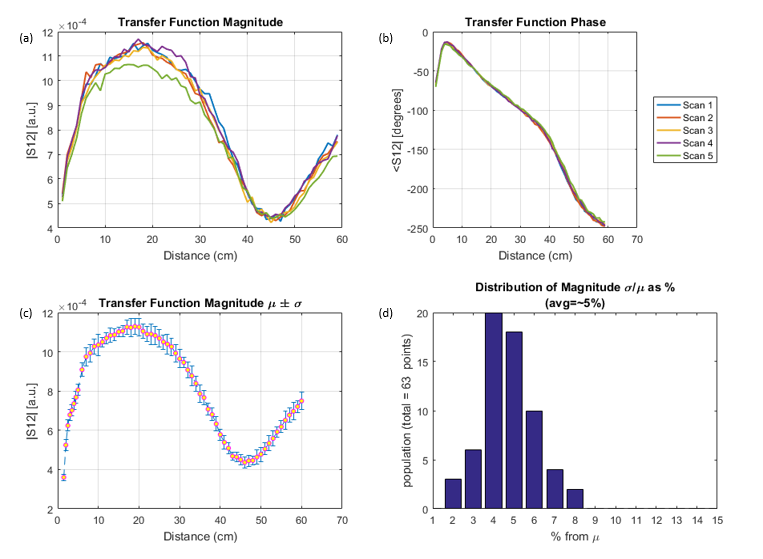
A transfer function system was developed that incrementally sources tangential RF electric fields at a specified frequency to discrete segments along the length of the lead while measuring the magnitude and phase response (S12) at the point of interest [2]. A single 70 cm, 8-electrode, straight-wire lead terminated with an implantable pulse generator (IPG) was used for this study. The entire implantable system was submerged in tissue simulating medium (conductivity = 0.47 S/m; permittivity = 78) [1]. A 64 MHz sinusoidal signal was sourced and measurements were made at the most distal electrode. In the first test case, the operator mounted the lead and IPG on the transfer function system and consecutively scanned the full length of the lead five times without touching the set-up. In the second test case, the same operator scanned the lead five times, but removed and remounted the AIMD system in between each scan. For each test case, the variation in transfer function magnitudes between scans was analyzed.Results
Figure 1 shows the results for the five consecutive scans without remounting and Figure 2 shows the results for the five scans with remounting. The mean (µ) and standard deviation (σ) of the transfer function magnitudes were calculated at 1 cm resolution for each test case and plotted in Figures 1c and 2c. The coefficient of variation (CV) of the magnitude was also calculated at 1 cm resolution. The CV distributions are depicted in Figures 1d and 2d. The variation in transfer function phase for both test cases was negligible as shown in Figures 1b and 2b. The transfer function measurements without remounting had minimal variation with an average CV of 2%. The measurement with remounting had higher variation with an average CV of 5%.Discussion and Conclusion
The study shows that the contribution of the transfer function system to the variation in magnitude and phase measurements is minimal. The data acquisition was highly repeatable for consecutive scans. The positioning of the AIMD in the test set-up has a greater impact and contributes additional variation to the transfer function measurements, with a potential magnitude CV of up to 8%. The average CV % for remounting the AIMD includes the system variation and could be carried forward in MRI RF-induced Tier 3 heating or malfunction modeling as uncertainty. This may lead to a more representative MRI RF safety assessment.Acknowledgements
The authors would like to acknowledge Patrick Untaran and Victor Limones of Boston Scientific for their assistance with data collection.References
[1] Assessment of the safety of magnetic resonance imaging for patients with an active implantable medical device. ISO/TS 10974: 2018(E).
[2] Park, S.-M., et al. Calculation of MRI-induced heating of an implanted medical lead wire with an electric field transfer function, J. Magn. Reson. Imag., Vol.26, 1278-1285, 2007.
[3] Piecewise eXcitation System for RF-Heating Evaluation of Medical Devices in MRI Environments, Zurich MedTech AG (Zurich, Switzerland). https://zmt.swiss/validation-hw/pix-system. Accessed October 30, 2018.
Figures