4162
The effect of tissue detail in pregnant body models on local SAR prediction accuracy at 3 T1Fetal-Neonatal Neuroimaging Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 2Department of Radiology, Harvard Medical School, Boston, MA, United States, 3Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 4Harvard-MIT Division of Health Sciences and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States, 5Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, United States, 6Institute for Medical Engineering and Science, Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Generating fully detailed electromagnetic body models requires acquisition and segmentation of high-resolution MR images which is particularly difficult in pregnancy due to motion and intolerance of long scan times. However, to explore fetal and maternal RF safety at 3 Tesla with both the standard mode and parallel RF transmission, a variety of pregnant body models are needed. We assess the effects of using simplified versions of 6 pregnant body models on predicting the maternal and fetal peak local SAR. We find that the simplified models under/over-estimate the peak local SAR of fully detailed models by at most 23%/16%.
Target Audience
MR physicists and clinicians interested in fetal and maternal RF safety at 3 T.Introduction
3 T MRI has been increasingly used to assess fetal/placental anatomy and physiology due to increased signal to noise ratio over 1.5 T. However, localized RF tissue heating concerns have been raised for the fetus at 3 T (1). Moreover, imaging speed is limited by SAR leading to increased motion artifacts, and transmit field nonuniformities lead to image shading. Although, parallel transmission (pTx) technology can decrease local SAR and mitigate transmit field uniformities (2,3), more individualized management of local SAR is required for an effective implementation of pTx.
Currently local SAR in pregnant body imaging is inferred from non-pregnant body models. Using more individualized (pregnant) body models will enable better understanding of fetal RF safety and can help balance appropriate safety margins and image quality. Due to the difficulty of generating fully detailed body models, especially for pregnant body imaging due to motion and intolerance to long scan times, simplified models which can be created from shorter scans are desirable. Previous studies on non-pregnant body models (4,5) reported up to 7.5% variation of peak local SAR with quadrature excitation when the body model was simplified. Another study reported that tissue detail in the fetus model had up to 10% effect on fetal SAR (6).
Here, we analyze the effect of simplifying the maternal tissue detail in 6 pregnant body models on local SAR prediction accuracy. We calculate maternal and fetal peak local SAR estimation errors for birdcage mode excitation, and random and realistic pTx excitations.
Methods
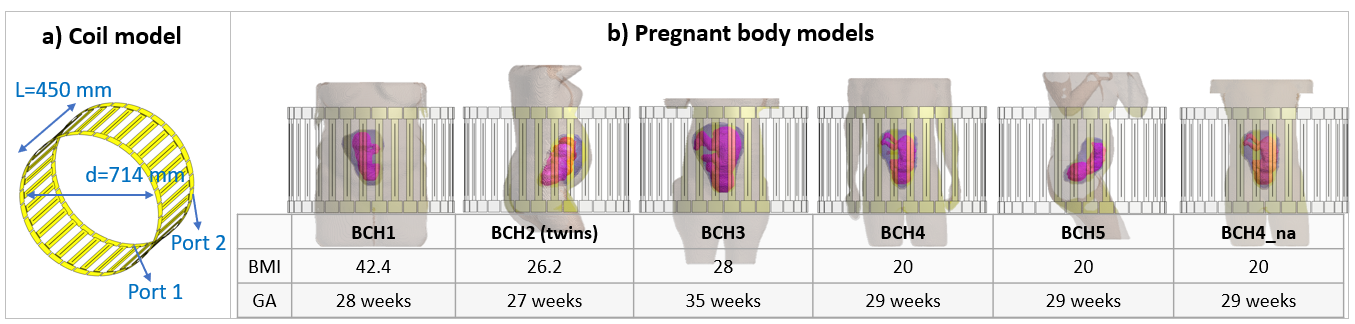
EM simulations: 6 truncated pregnant body models (7) were simulated inside a 2-channel 32-rung birdcage body coil model (Figure.1). Two versions of each body model were simulated: 1) fully detailed with ~25 tissues and 2) Muscle-Lung-Fat (MLF) version with 8 tissues obtained by assigning all maternal tissues to fat (fat and bones), lung (lung) and muscle (remainder). The 5 tissues inside the uterus (placenta, umbilical cord, amniotic fluid, fetus, fetal brain) were not changed.
RF pulses: Birdcage mode excitation, 1000 random RF shim settings and two realistic RF shimming and two realistic 2-spoke pTx pulses were used to evaluate SAR estimation errors for each body model pair. Realistic pTx pulses were designed for each model using the algorithm described in (3) with the following specifications: target FA = 90ᵒ, TBW = 4, slice thickness: 3 mm, pulse duration: 2 ms RF shimming&birdcage, 4.8 ms 2-spokes).
SAR estimation error calculation: The 10g avg peak local SAR for each body model was approximately calculated by using virtual observation points (VOPs) (8) generated with a small (1-2%) overestimation limit. For each body model pair, peak local SAR estimation error percentage is calculated using:
$$ peak\:local\:SAR\: estimation\:error\:\% = \frac{peak\:local\:SAR_{MLF\:model}}{peak\:local\:SAR_{fully\:detailed\:model}} *100 - 100 $$
Hence positive values represent overestimation and negative values represent underestimation of SAR by the MLF models.
Results/Discussion
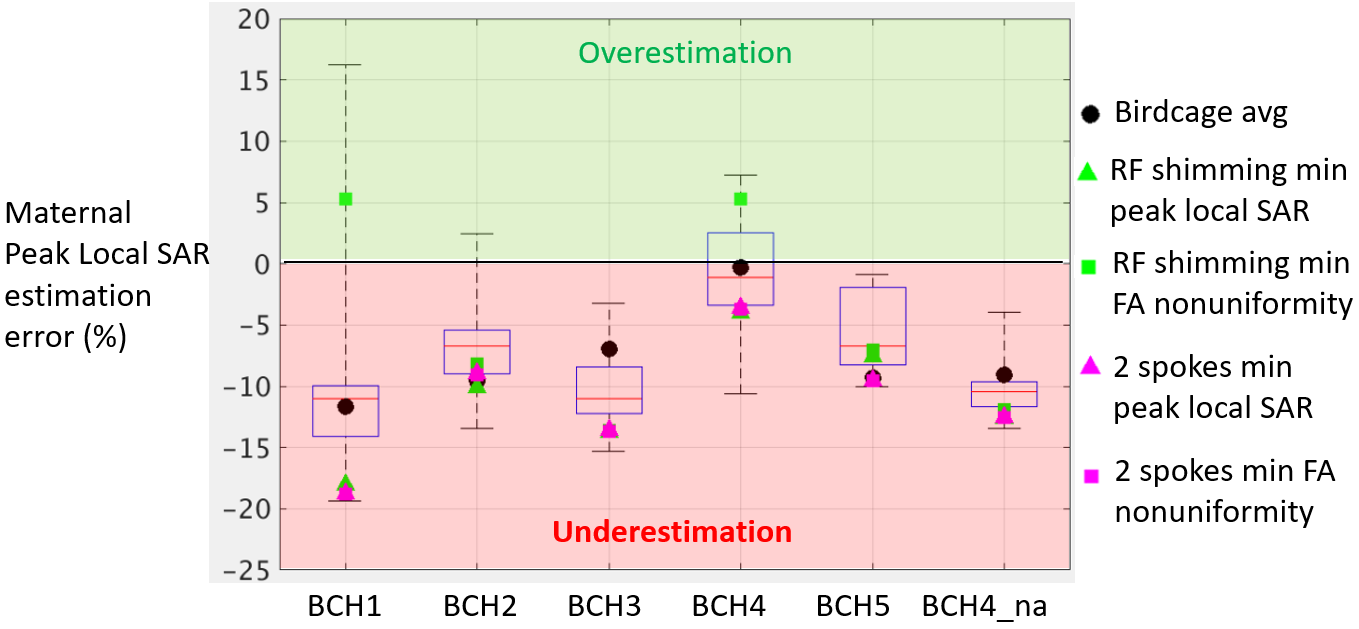
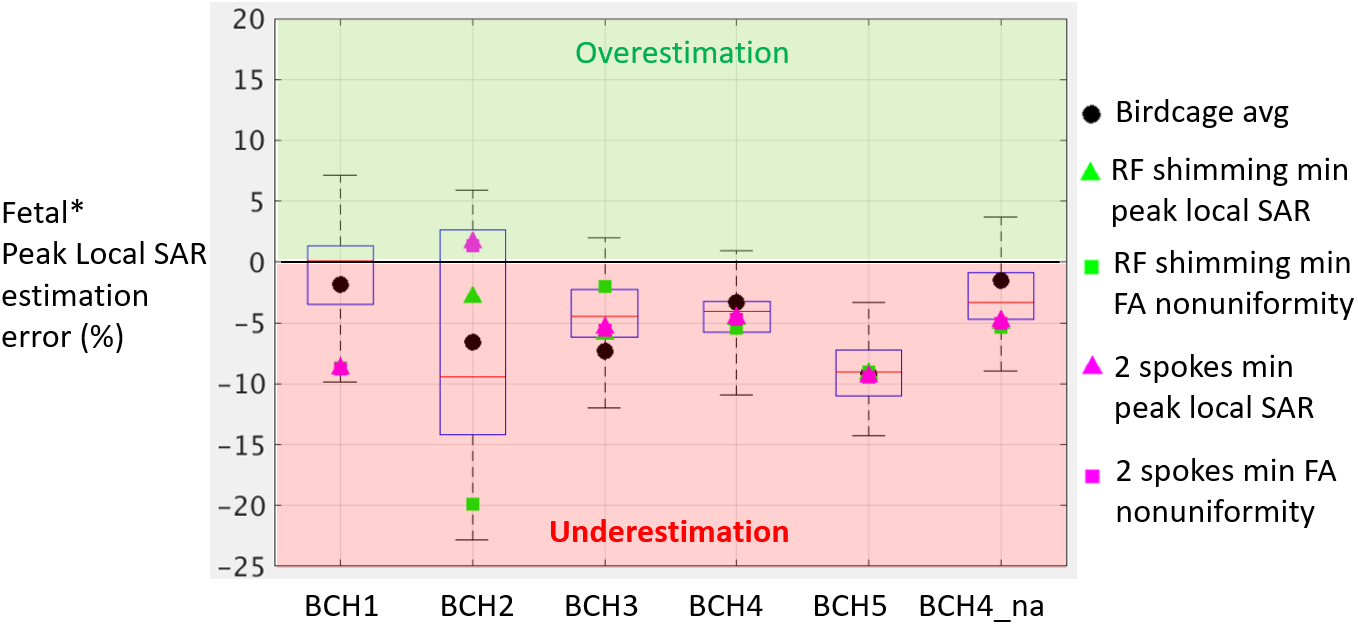
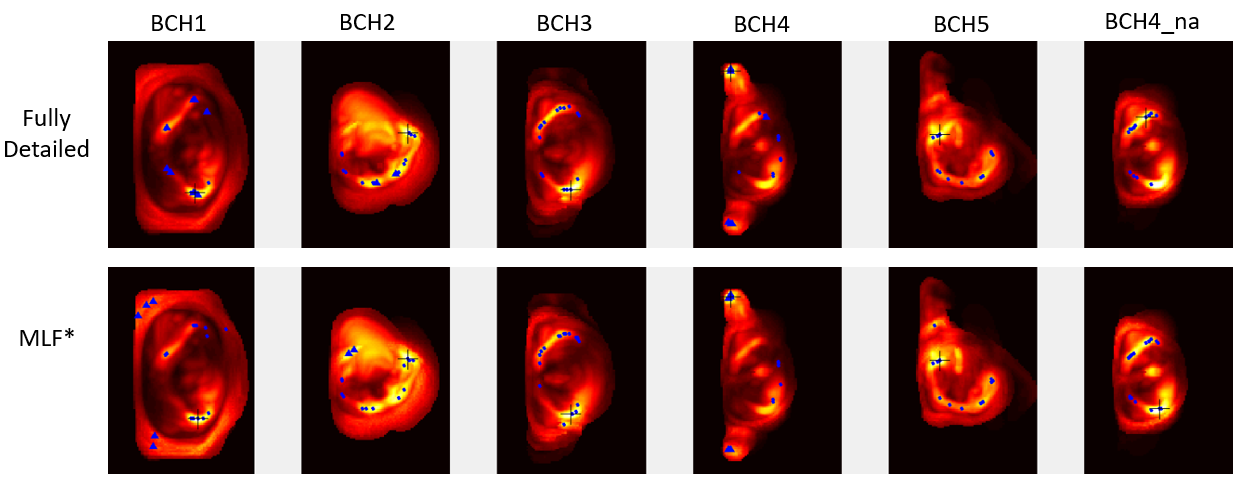
Figure 2 and Figure 3 show the maternal and fetal peak local SAR estimation errors for all RF excitations and body models. The maximum underestimation and overestimation of maternal/fetal peak local SAR are 19%/23% and 16%/7%. The largest variation for maternal, and fetal SAR estimation error is observed in BCH1 (highest maternal BMI), and BCH2 (twins) respectively. MLF version underestimates both maternal and fetal SAR of the fully detailed version, for more than half of the random RF shim settings for each body model (median is at or below zero in all boxplots). Only for BCH5, both maternal and fetal SAR are underestimated by the MLF body models for all excitation modes. Figure 4 shows the locations of maternal peak local SAR in each model pair for random RF shim settings and birdcage mode excitation. For the birdcage mode excitation, peak local SAR location in the MLF model is the same as in the fully detailed model except for BCH4_na while the location changes significantly for several random RF shim settings. Even if the estimation error of the peak local SAR value is limited by 23%, the location change may result in more significant differences in temperature simulations.Conclusion
We showed that for subjects represented by body models in this study, simplifying the body models resulted in a maximum peak local SAR estimation error of 23%. We also observed that the location of maternal peak local SAR can vary significantly between the fully detailed and simplified models which can have a significant impact on the resulting temperature estimation. Further analysis will be conducted to understand the effect of the change in maternal and fetal peak local SAR location.Acknowledgements
R01 EB017337, U01 HD087211 and R01 EB006847.References
1. Hand JW, Li Y, Hajnal JV. Numerical study of RF exposure and the resulting temperature rise in the foetus during a magnetic resonance procedure. Phys. Med. Biol. 2010;55:913–930 doi: 10.1088/0031-9155/55/4/001.
2. Murbach M, Neufeld E, Samaras T, et al. Pregnant women models analyzed for RF exposure and temperature increase in 3T RF shimmed birdcages. Magn. Reson. Med. 2017;77:2048–2056.
3. Yetisir F, Turk EA, Guerin B, Grant EP, Wald LL, Adalsteinsson E. Potential of parallel transmission for fetal imaging in reducing SAR and mitigating ip angle inhomogeneities: a simulation study at 3T. In: Proceedings of the 25th Annual Meeting of ISMRM. Honolulu, Hawai’i; 2017. p. 4823.
4. Homann H, Börnert P, Eggers H, Nehrke K, Dössel O, Graesslin I. Toward individualized SAR models and in vivo validation. Magn. Reson. Med. 2011;66:1767–1776 doi: 10.1002/mrm.22948.
5. van den Bergen B, Van den Berg CAT, Bartels LW, Lagendijk JJW. 7 T body MRI: B1 shimming with simultaneous SAR reduction. Phys. Med. Biol. 2007;52:5429–5441 doi: 10.1088/0031-9155/52/17/022.
6. Malik SJ, Hand JW, Hajnal JV. The effect of variable amniotic fluid conductivity and fetal tissues properties on B1+ and local SAR for fetal imaging at 3T. In: Proceedings of the 25th Annual Meeting of ISMRM. Honolulu, Hawai’i; 2017. p. 5578. doi: 10.13099/vip21000-03-0.
7. Abaci Turk E, Yetisir F, Gagoski BA, et al. Safety of 3T MRI Scan for pregnant women: Effect of Maternal Size, Maternal Position and Twin Pregnancy. In: Proceedings of the 25th Annual Meeting of ISMRM. Honolulu, Hawai’i; 2017. p. 4810.
8. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn. Reson. Med. 2011;66:1468–1476 doi: 10.1002/mrm.22927.
Figures