4156
Simplified subject-based models for efficient electromagnetic simulations and evaluation of local SAR for 7 T abdominal MRI1SPMIC, Physics, University of Nottingham, Nottingham, United Kingdom, 2University of Nottingham, Nottingham, United Kingdom
Synopsis
We investigated the required detail of human body models for Fdtd simulations of a multi-transmit eight-channel body array used for abdominal imaging at UHF. The effect of reducing the number of tissue types on local 10 g averaged SAR (SAR10g,av), B1+ and coil scattering matrices (S-matrices) was investigated on subject-based manually segmented models. Models that differentiate between the lungs, fat, muscle and skin tissue were found to be sufficient to recreate results produced in fully segmented models. This finding was used to implement segmentations of 3 T mDIXON images of subjects to generate subject-specific models for Fdtd simulations efficiently.
Purpose
Current methods used for assessing safety limits of multi-transmit systems typically involve applying ‘worst case’ SAR values, which can severely limit the power available for abdominal scanning. Alternatively, individual subjects can be modelled to allow more accurate SAR predictions, but this can be very time consuming, requiring user intervention for tissue segmentation. There is a need to be able to rapidly create subject-specific models automatically. This may be achieved by using truncated models that only include the upper body of the subject, reducing the number of tissues that need to be distinguished [3] and using automatic segmentation of MRI data.Aim
To develop a pipeline for the automatic construction of individual subject-specific models required for performing EM simulations to study and further inform the safety of abdominal imaging on a 7 T multi-transmit system.Methods
One male and one female subject were scanned on a 3 T Philips Ingenia system to acquire mDIXON data. Images were manually segmented in Analyze software, labelled according to a tissue library and constructed into 3D body models in Matlab and imported into Remcom XFdtd software (v7.7.1.1) which run on a NVIDIA GPU (TITAN Xp). Optimised gridding was used with a minimum [maximum] cell size of 3.4x1.8x0.4 [7.8x7.9x22.8] mm3. An 8 TX/32 RX fractionated dipole array (MRCoils) was simulated using a wire-based model [4]. Simulations were run to a convergence of -30 dB, taking around 20 minutes per transmit element. Broadband excitation was used and each simulation was scaled to 1 W input power per transmit channel for SAR calculation.
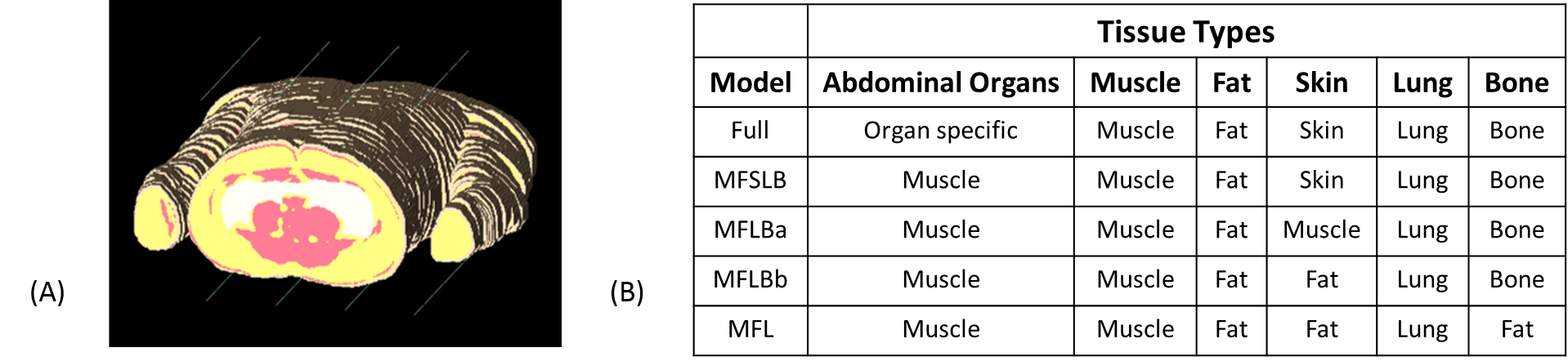
A further four versions of each model were created with reduced tissue complexity (Figure 1), and the simulations were repeated for each of these models in the same geometry. The EM fields and S-parameters were exported and analysed in Matlab to calculate SAR10g,av, B1+ profiles and the S-matrices for the body array.
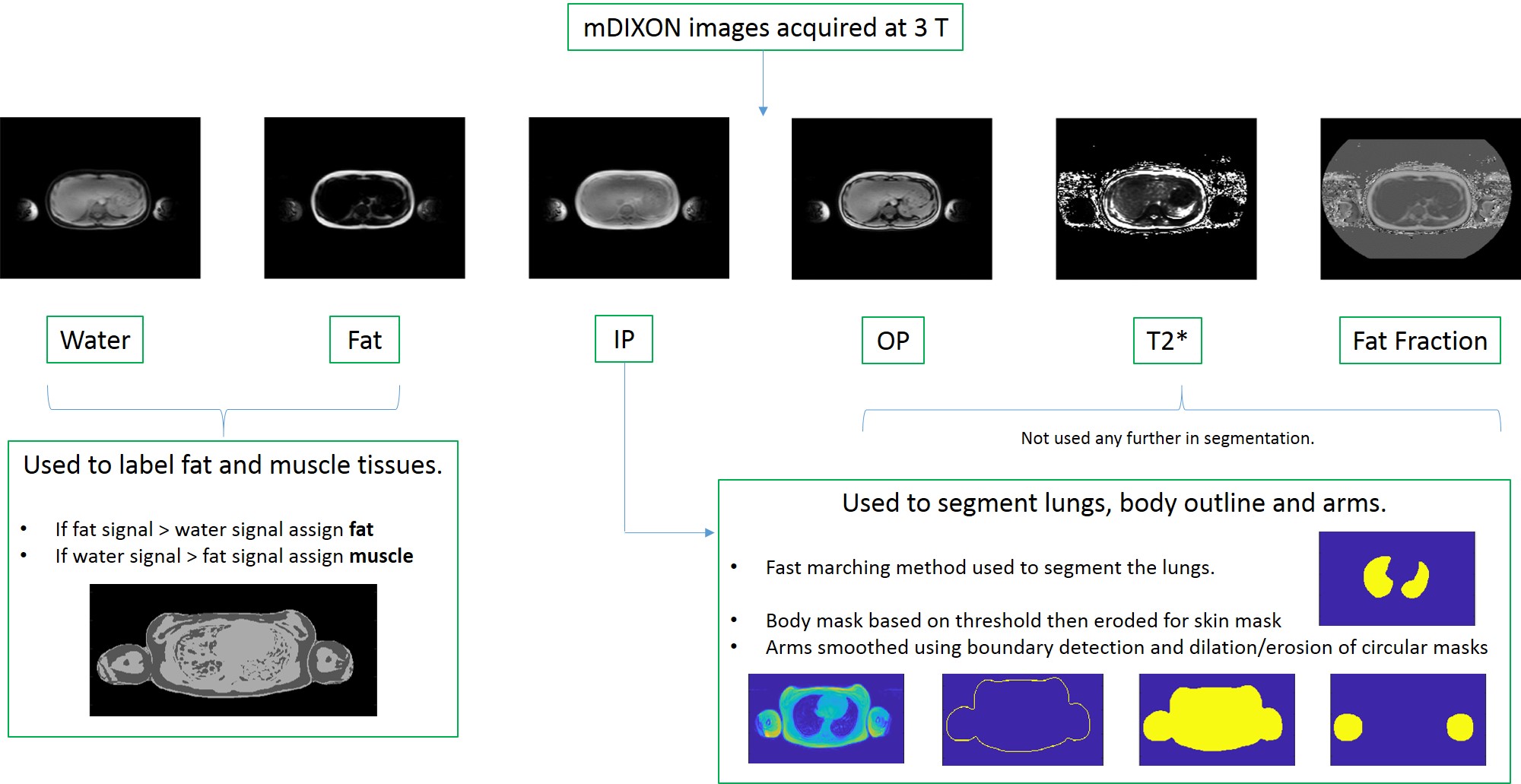
A method was then developed to create 3D models automatically from acquired 3 T mDIXON images (Figure 2). Simulations were then repeated with the automatically constructed models and results compared to manually segmented models.
Results
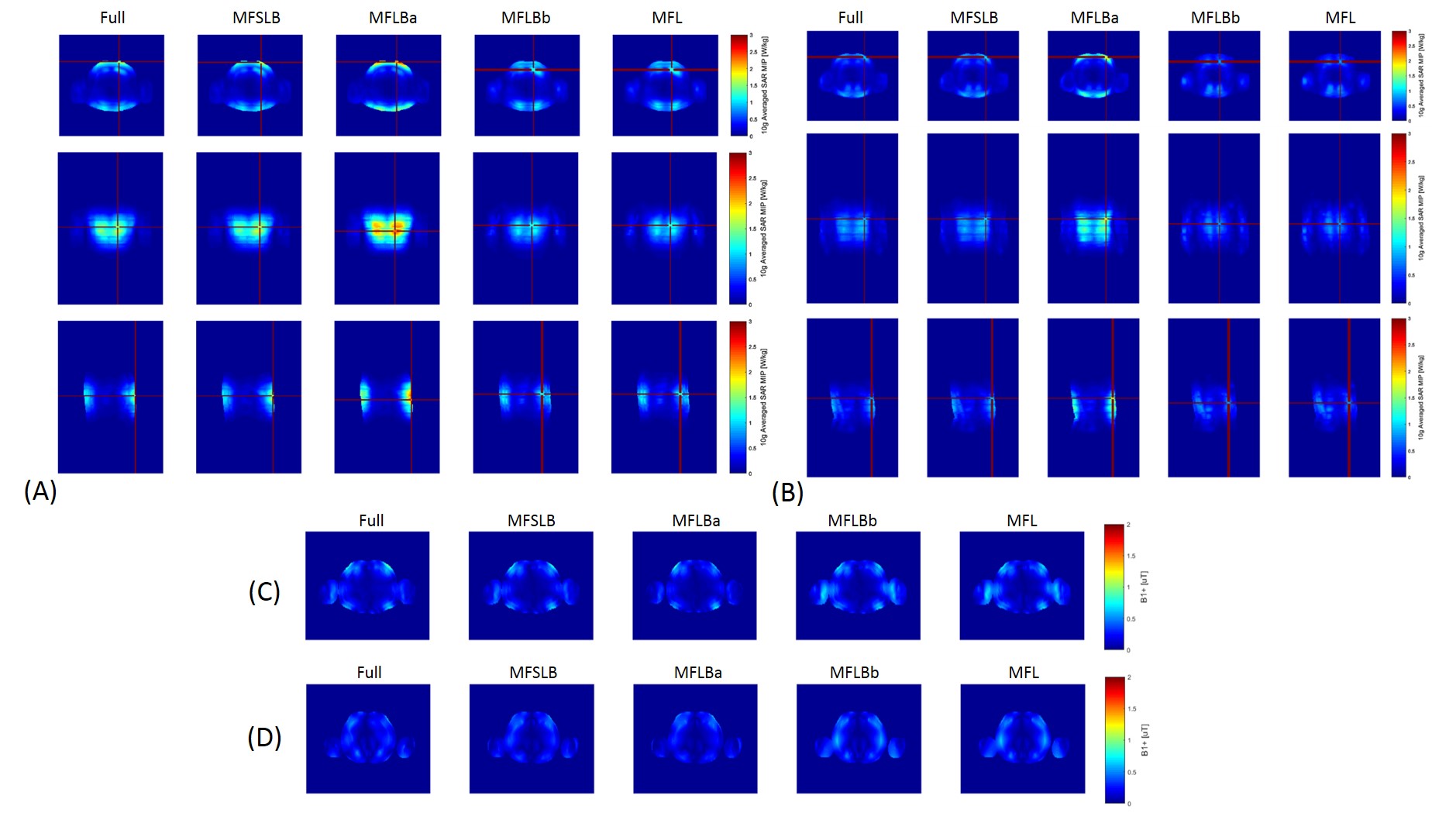
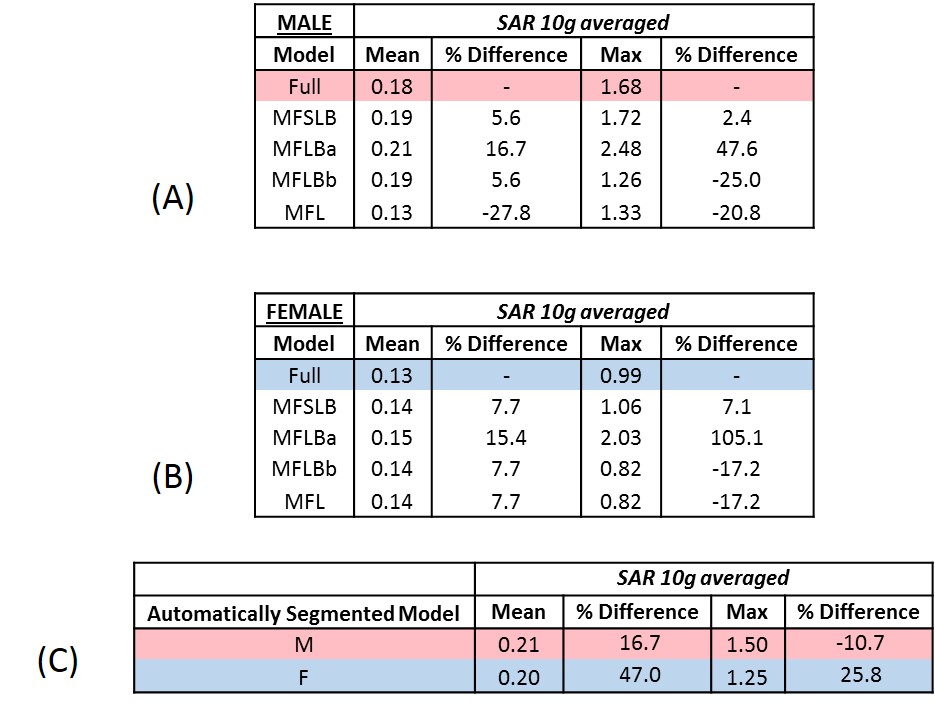
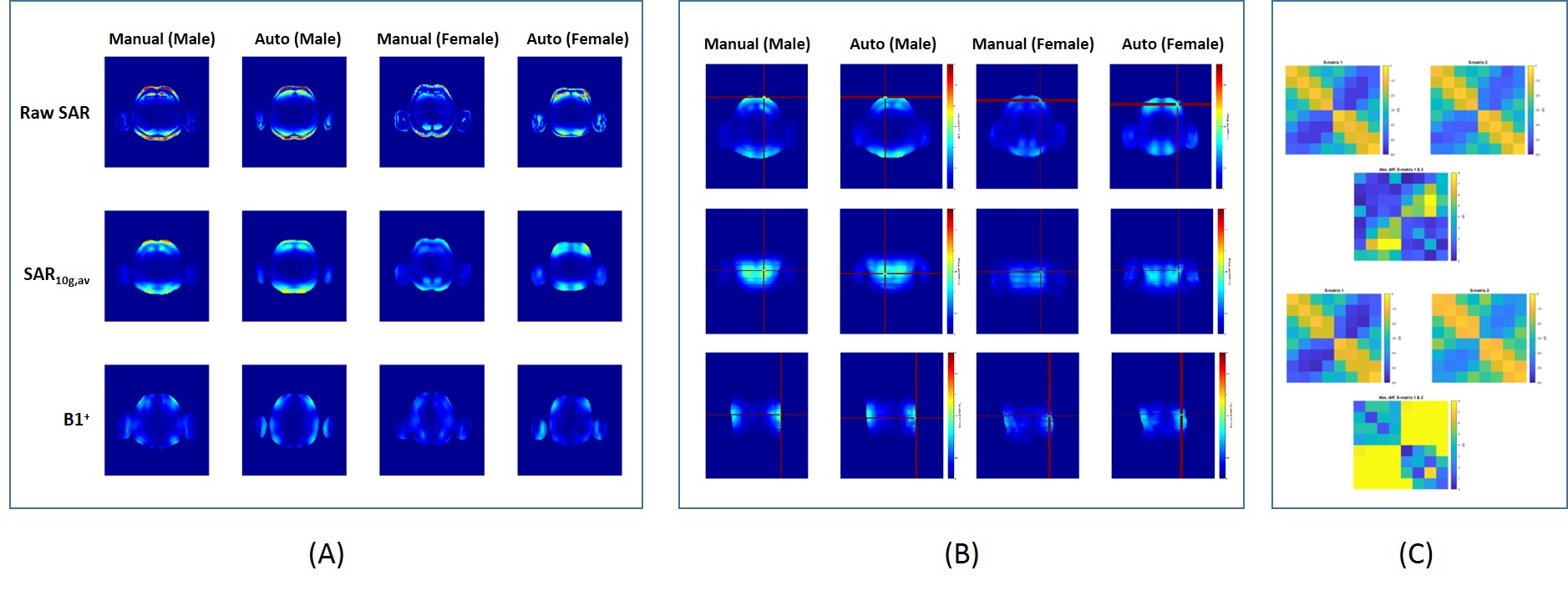
The effects from reducing the models’ tissue complexity on SAR10g,av and B1+ are shown in Figure 3 with quantitative results in Figure 4. The SAR10g,av distributions were similar for the full and MFSLB models however the maximum SAR10g,av increased by 2.4 and 7.1 % for male and female simulations respectively. SAR10g,av distributions begin to deviate more significantly in MFLBa, MFLBb and MFL models where the skin tissue is no longer labelled. MFLBb and MFL models return similar results suggesting that replacing bone with muscle had no significant impact. B1+ distributions and S-matrices were similar across all models. Based on these results, methods were developed to automatically segment fat, muscle, skin and lung tissues (Figure 2). Figures 5(A-C) shows the results from simulations with the automatically segmented M/F models. The SAR10g,av values obtained are outlined in Figure 4(C). The male model showed a 10 % decrease in the maximum SAR10g,av and the female model showed an increase of 25 %. The location of these maximum SAR10g,av values did not change significantly (Figure 5(B) - the displacement of the male SAR10g,av hotspot in the negative x direction is not surprising considering the body array was adjusted to encompass slightly altered geometry of the auto model and therefore the distribution of E fields will be subtly different).Discussion
Simplifying the full model to the MFSLB model caused an overestimation of SAR10g,av, which makes the SAR calculations more conservative and contributes an additional safety factor to final SAR results. Skin tissue was found to be essential for accurate SAR calculation at the surface of the models, but bone could be removed with no effect. Automatic segmentation worked reasonably well in the man. It did not produce similar results in the female model as this was smaller after automatic segmentation probably due to the effects of small changes in the amount of subcutaneous fat on signal thresh-holding. This indicates the acute sensitivity of the simulation results to the exact distribution of fat. The effects of variability in segmentation on SAR models is now being investigated.Conclusion
Simplified models can be used to assess SAR10g,av for UHF abdominal MRI applications. This will allow for quicker subject-specific SAR modelling which can help to set more appropriate upper limits on power input.Acknowledgements
We gratefully acknowledge the support of NVIDIA Corporation with the donation of the Titan Xp GPU used for this research.References
1. Homann et al. Toward Individualized SAR Models and In Vivo Validation, MRM. 2011;66:1767-1776
2. Le Garrec et al. Probabilistic Analysis of the Specific Absorption Rate Intersubject Variability Safety Factor in Parallel Transmission MRI, MRM. 2017;78:1217-1223
3. Wolf et al. SAR Simulations for High-Field MRI: How Much Detail, Effort, and Accuracy Is Needed?, MRM. 2013;69:1157-1168
4. Bawden et al. Electrical lengthening to improve electromagnetic simulations and SAR calculations of meandered body dipole elements at 7 T, In Proc. ISMRM (Paris). 2018
Figures