4152
Feasibility of personalized RF safety monitoring in pTx MRI using linear registration versus non-linear registration1Wellcome Centre for Integrative Neuroimaging, FMRIB Division, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Oxford Centre for Clinical Magnetic Resonance Research, Department of Cardiovascular Medicine, University of Oxford, Oxford, United Kingdom
Synopsis
In this study, we demonstrate the feasibility of personalised RF safety monitoring in pTx MRI using linear registration versus non-linear registration. We evaluate this by using two well-characterised models, Duke, and MIDA. An 8-channel dipole array was used to evaluate maps of 10g averaged SAR across a range of B1+ shims, showing potential utility of linear registration (rotation, scaling, skew, translation). Our study shows that both linear registration and non-linear registration can be used to monitor SAR in pTx MRI to reduce the safety margin arising from differences in patient head position, shape and size.
Introduction
Parallel transmit (pTx) MRI has been utilized in ultra-high-field MRI,1 and has shown numerous benefits over single-channel transmission.2–5 The approach of combining multiple transmit sources demands extensive electromagnetic (EM) simulation, and thus advanced RF safety monitoring techniques have been developed, such as virtual-observation-points (VOPs)6 and Q-matrices.7 However, morphometric differences between subjects require a safety margin to be incorporated in order to allow for adequate RF safety monitoring across the population.8 Additionally, the position of the subject could change the RF deposition.9 To address this, personalised RF safety modelling methods have been introduced to reduce the required safety factor.7,10–12 In this study, we investigated the potential benefits of using a simple (and robust) linear-registration13 of brain-only data (representing a simple personalized model), and compared this with the use of full non-linear registration. Methods
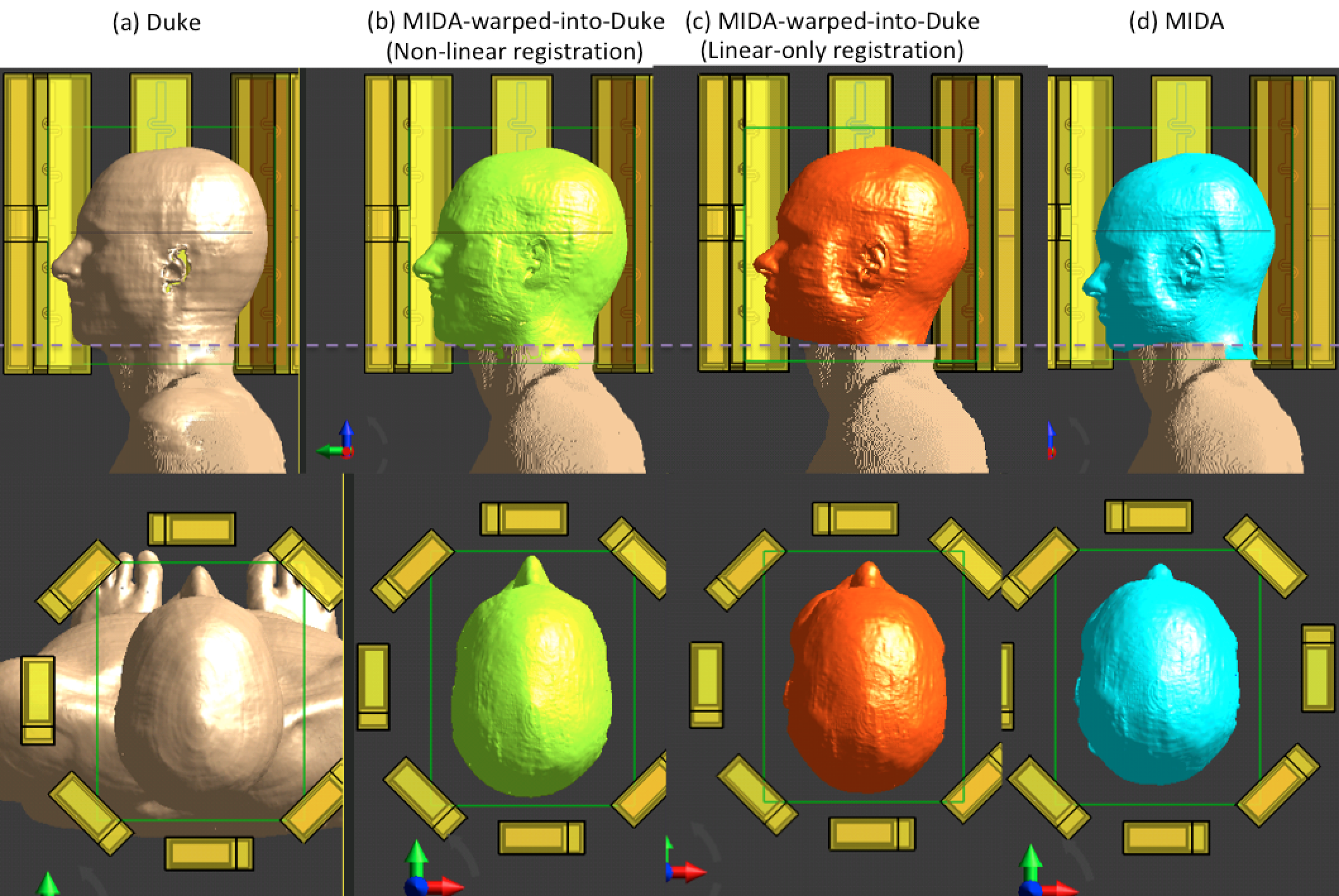
An 8-channel fractionated dipole array coil (MR Coils, The Netherlands) with an octagonal geometry of 280 mm diameter, surrounding voxel EM models of the head, was simulated at 297.2 MHz to assess specific absorption rate (SAR). To account for coupling, two capacitors were placed at the edge of each element with values set to the true coil capacitor values. The gradient coil was not included in the simulation model. The Duke model14 (Figure 1a, representing the subject in the magnet) and MIDA model15 (Figure 1d, representing the EM model) were positioned at the centre of the coil, and all models were shifted 24mm in the z-direction to avoid the shoulders being in physical contact with the dipole array. The MIDA model was then warped into Duke space (denoted MIKE) using both non-linear registration (Figure 1b),12 and a linear registration applied using brain-only information (Figure 1c). The body of the Duke voxel model was added to account for loading and energy absorption in the neck and shoulders. In data analysis, SAR results were averaged to 10g mass using the IEEE/IEC 62704-1 standard,16 and the region of the Duke body model (below the dotted line in Figure 1) was excluded in post-processing to minimize effects from mis-matched regions. 5,000 RF shim sets with random phase and magnitude were generated, including circularly polarised (CP) mode, and were applied again in flipped-element order (including anti-CP mode) providing 10,000 total RF shim sets. The data were normalised to 1W input power.Results
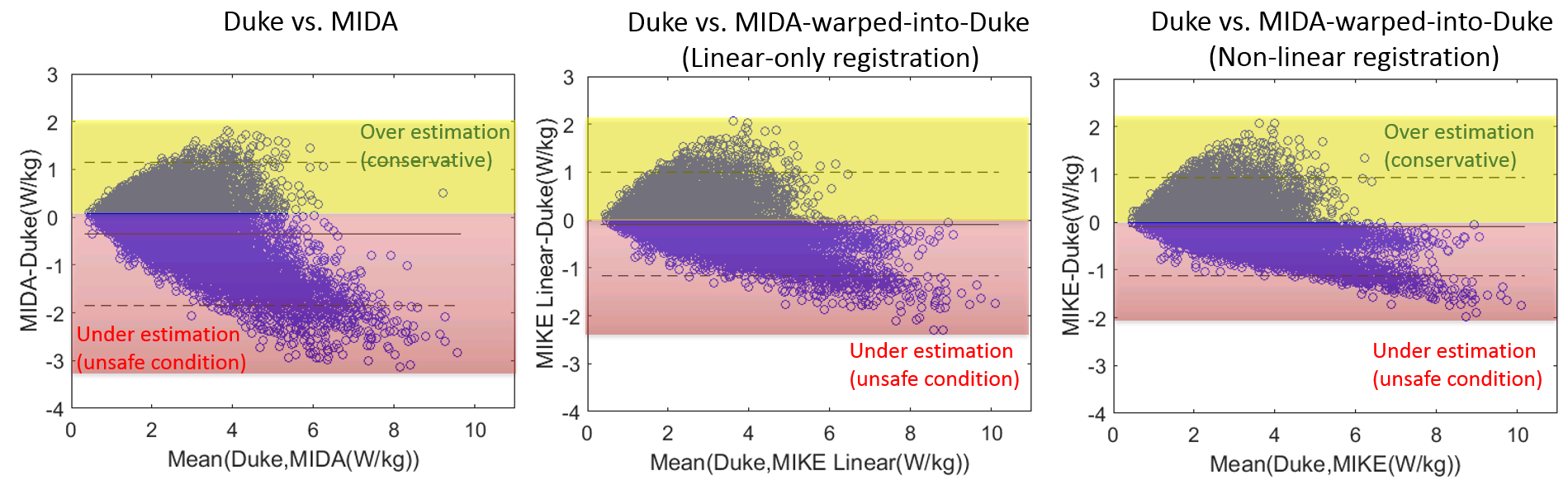
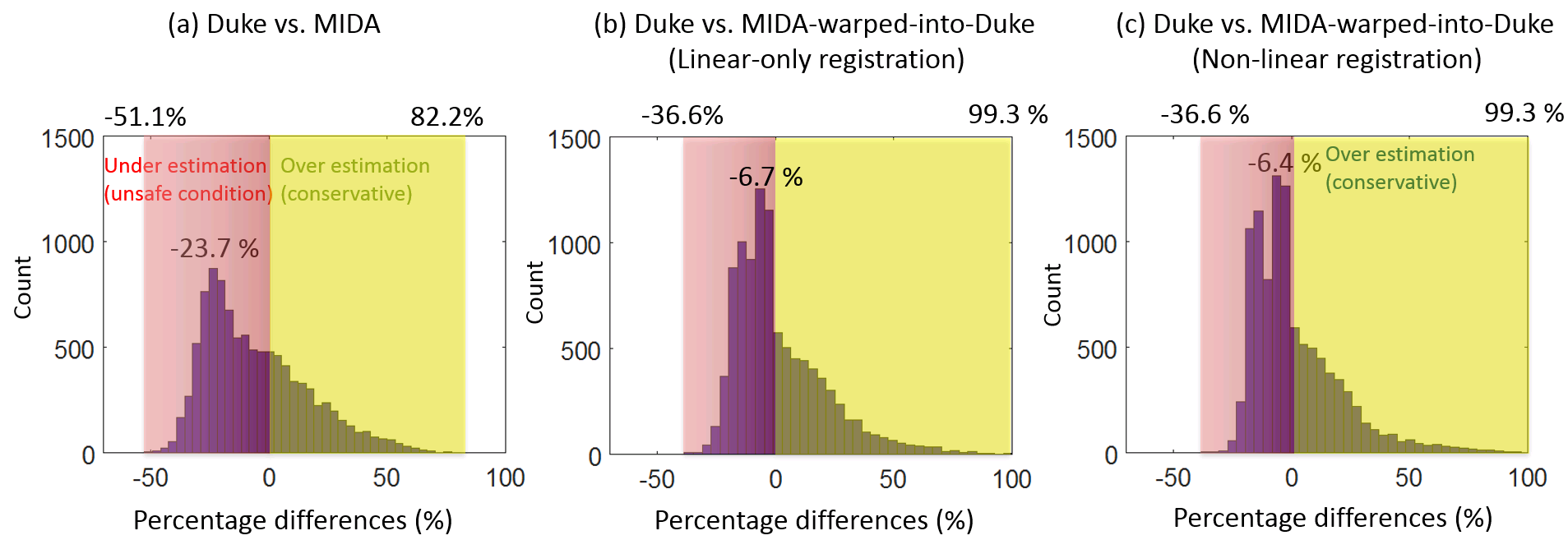
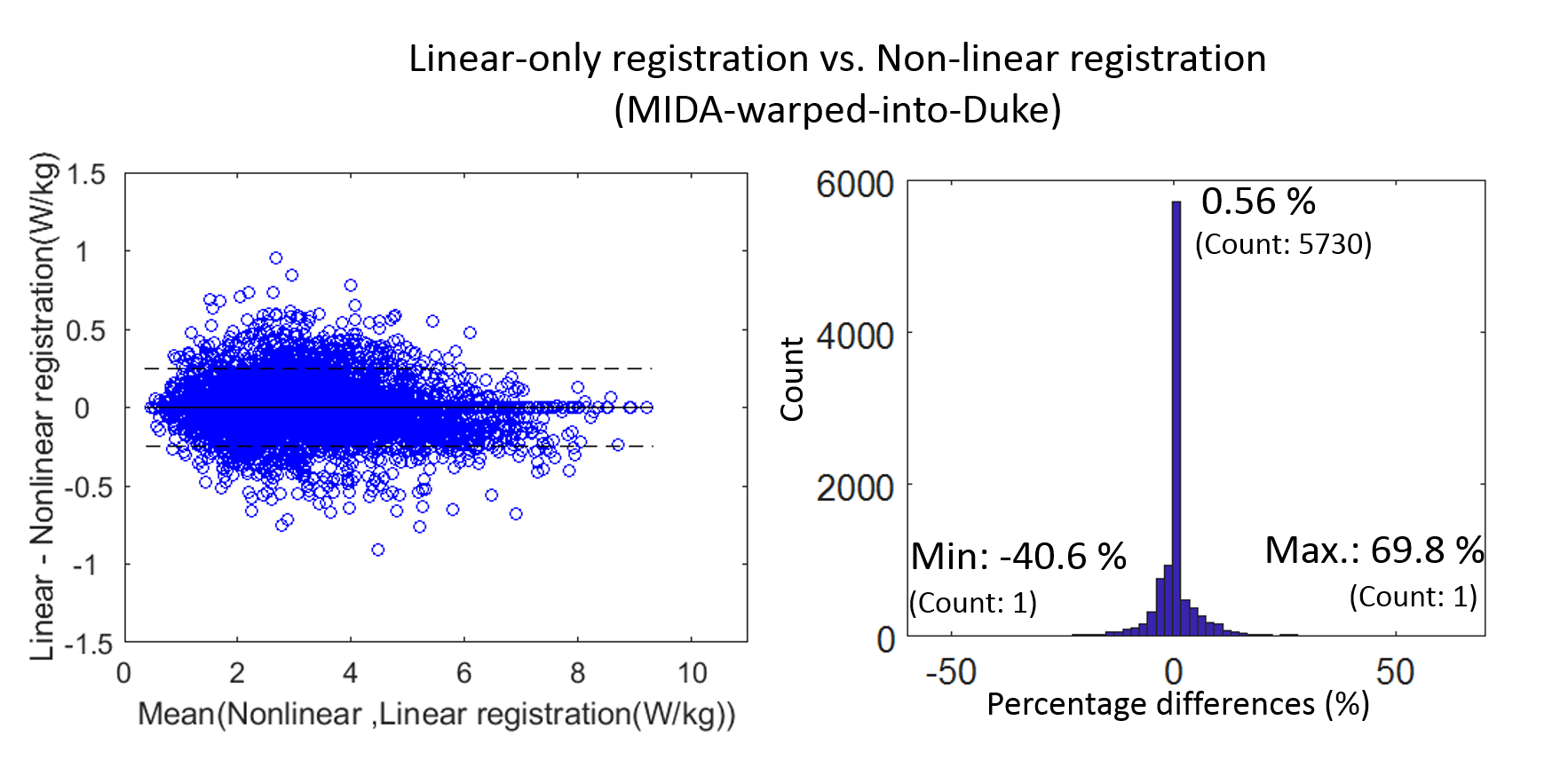
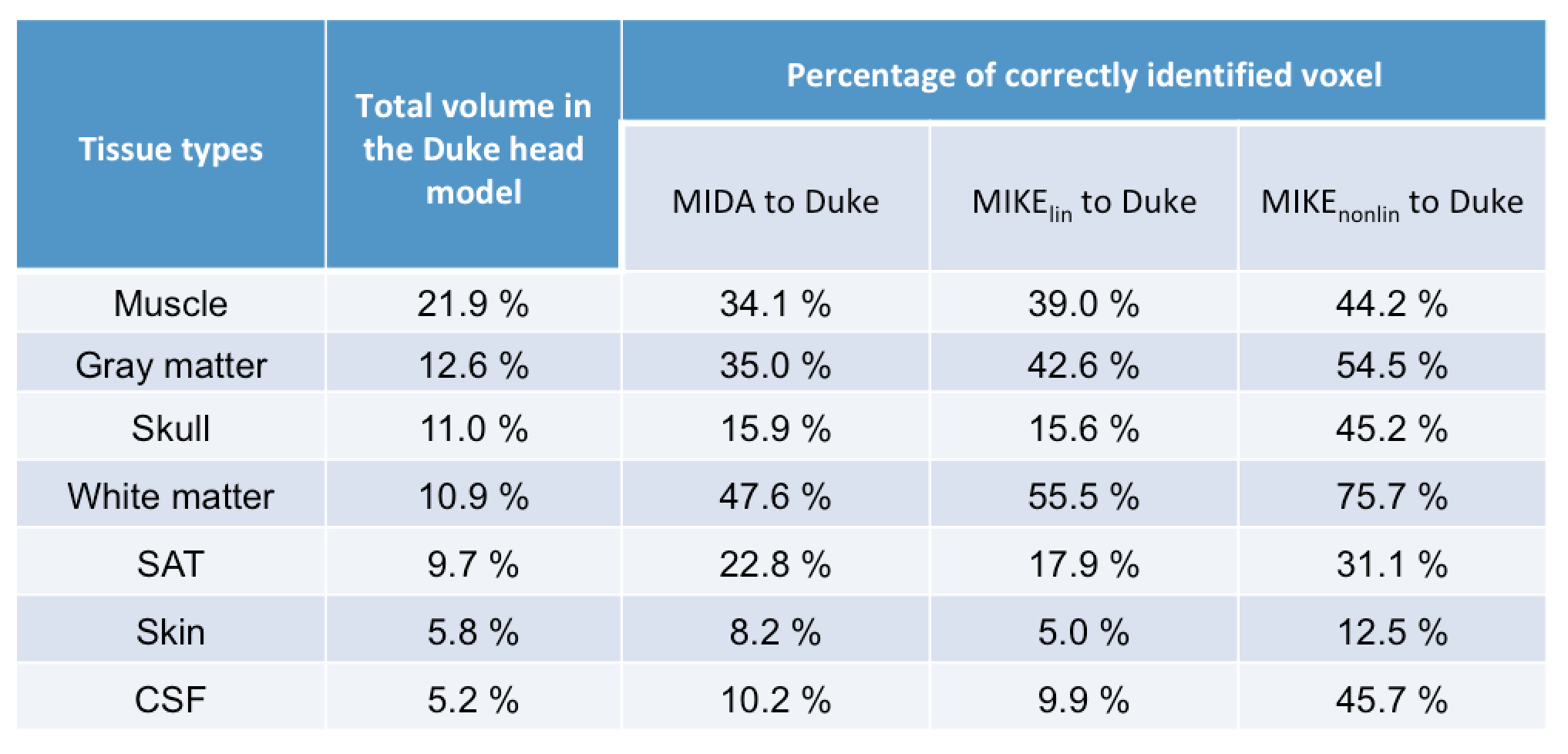
Table 1 shows the degree of overlap (tissue matching score) for six major tissue compartments, showing that non-linear registration provides the closest matching to Duke, with linear-only registration showing a lower matching, as expected. Figure 2 shows a Bland-Altman SAR plot, indicating improved under-estimation in worst-case SAR when non-linear registration was applied to the entire head. We find the underestimation is similar when using linear-only registration, being only slightly worse than when using full non-linear registration. Figure 3 shows histograms of differences in worst-case SAR for all four models, showing that the underestimation between Duke and MIDA models was reduced when both linear and non-linear registration are applied. Finally, Figure 4 compares the worst-case SAR difference between linear and non-linear registration, showing that only marginal differences were found.Discussion
Our study showed that linear registration of the brain in personalized RF safety modelling offers potential utility, and specific benefits for real-time monitoring. Using 12 degrees-of-freedom affine registration, the size and relative position of the subject in the RF coil can be roughly estimated, albeit with limited capability to estimate worst-case SAR of -40.6% to 69.8% differences from non-linear registration (-21.9%/+26.8% within 99.0% confidence). The main challenge of using linear registration is defining the relative subject position inside the RF coil. Note that the potential scenario of over-estimation could be encountered when the transmit coils are tightly fitted to the subject, which should be monitored carefully and may require an altered scaling factor. The localisation scan data can potentially be used for linear registration, and results of the potential location and size of the subject can be pre-calculated and compressed using the VOPs method. Non-linear registration offers further benefits of reducing the degree of underestimation of worst-case SAR in pTx MRI. Further studies are needed to assess the relative position of subjects inside the coil and create a better connection between head-only models and the loading caused by the presence of the body.Conclusions
The potential benefits of using linear-only registration for pTx RF safety are that it offers a simpler application to reduce the safety margin used to account for inter-subject variability and in real-time SAR monitoring.Acknowledgements
Oxford-Radcliffe Graduate Scholarship (University College Oxford) and Clarendon Fund.References
1. Katscher U, Börnert P, Leussler C, Van den Brink JS. Transmit SENSE. Magn Reson Med. 2003;49(1):144-150. doi:10.1002/mrm.10353.
2. Orzada S, Maderwald S, Poser BA, Bitz AK, Quick HH, Ladd ME. RF excitation using Time Interleaved Acquisition of Modes (TIAMO) to address B1 inhomogeneity in high-field MRI. Magn Reson Med. 2010;64(2):327-333. doi:10.1002/mrm.22527.
3. Cloos MA, Boulant N, Luong M, et al. kT-points: Short three-dimensional tailored RF pulses for flip-angle homogenization over an extended volume. Magn Reson Med. 2012;67(1):72-80. doi:10.1002/mrm.22978.
4. Gras V, Vignaud A, Amadon A, Le Bihan D, Boulant N. Universal pulses: A new concept for calibration-free parallel transmission. Magn Reson Med. 2017;77(2):635-643. doi:10.1002/mrm.26148.
5. Lee J, Gebhardt M, Wald LL, Adalsteinsson E. Local SAR in parallel transmission pulse design. Magn Reson Med. 2012;67(6):1566-1578. doi:10.1002/mrm.23140.
6. Eichfelder G, Gebhardt M. Local specific absorption rate control for parallel transmission by virtual observation points. Magn Reson Med. 2011;66(5):1468-1476. doi:10.1002/mrm.22927.
7. Graesslin I, Homann H, Biederer S, et al. A specific absorption rate prediction concept for parallel transmission MR. Magn Reson Med. 2012;68(5):1664-1674. doi:10.1002/mrm.24138.
8. Le Garrec M, Gras V, Hang M-F, Ferrand G, Luong M, Boulant N. Probabilistic Analysis of the Specific Absorption Rate Intersubject Variability Safety Factor in Parallel Transmission MRI. Magenetic Reson Med. 2017;78:1217-1223. doi:10.1002/mrm.26468.
9. Wolf S, Diehl D, Gebhardt M, Mallow J, Speck O. SAR simulations for high-field MRI: How much detail, effort, and accuracy is needed? Magn Reson Med. 2013;69(4):1157-1168. doi:10.1002/mrm.24329.
10. Jin J, Liu F, Weber E, Crozier S. Improving SAR estimations in MRI using subject-specific models. Phys Med Biol. 2012;57(24):8153-8171. doi:10.1088/0031-9155/57/24/8153.
11. Ipek O, De Greef M, Raaijmakers AJE, Luijten PR, Lagendijk JJW, Van Den Berg CAT. Patient-specific SAR estimation for the 8-channel radiative antenna array at 7 T prostate MRI. In: Proc. Intl. Soc. Mag. Reson. Med.; 2012.
12. Jeong H, Andersson JLR, Hess AT, Jezzard P. A personalised SAR model for subject-specific RF safety. In: Proc. Intl. Soc. Mag. Reson. Med.; 2017.
13. Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17(2):825-841. doi:10.1016/S1053-8119(02)91132-8.
14. Gosselin MC, Neufeld E, Moser H, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: The Virtual Population 3.0. Phys Med Biol. 2014;59(18):5287-5303. doi:10.1088/0031-9155/59/18/5287.
15. Iacono MI, Neufeld E, Akinnagbe E, et al. MIDA: A multimodal imaging-based detailed anatomical model of the human head and neck. PLoS One. 2015;10(4). doi:10.1371/journal.pone.0124126.
16. IEC Committee. IEEE 62704-1-2017 - IEC/IEEE International Standard for Determining the Peak Spatial Average Specific Absorption Rate (SAR) in the Human Body from Wireless Communications Devices, 30 MHz - 6 GHz. Part 1: General Requirements for using the Finite Difference. 2017.
Figures