4151
Parallel transmit RF safety simulation: effects of differences in tissue compartmentsbetween different voxel models1Wellcome Centre for Integrative Neuroimaging, FMRIB Division, Nuffield Dept of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Oxford Centre for Clinical Magnetic Resonance Research, Department of Cardiovascular Medicine, University of Oxford, Oxford, United Kingdom
Synopsis
In this study, we demonstrate the effects on RF simulation from subtly different tissue compartments in the same morphometric space. We evaluate this by using two well-characterised electromagnetic models, Duke versions 1.0 and 3.0. Maps of 10g SAR across a range of B1+ shims were evaluated, showing uncertainties arising from segmentation differences. By using a dedicated voxel model, an increased confidence in electromagnetic simulation can be achieved.
Introduction
RF safety modelling in parallel transmit (pTx) MRI has been widely studied.1–3 In previous studies, morphometric differences between two models (a ‘subject-specific’ model, e.g. Duke or Ella, and a ‘standard’ model, e.g. MIDA) were minimized using non-linear registration, and SAR under- or over- estimation was evaluated in the metric of maximum 10g SAR.4 However, non-linear warping was observed to sometimes produce a higher overestimation than simulation results without warping, especially for the case of Ella being the ‘subject-specific’ model, which indicates that there could be effects coming from segmentation differences between the three models (MIDA, Duke, and Ella). In this study, the magnitude of effects coming from the specifics of tissue compartment characterisation was studied using two different versions of the same Duke model, which have subtly different compartmental descriptions, but otherwise contain identical morphometric information.Methods
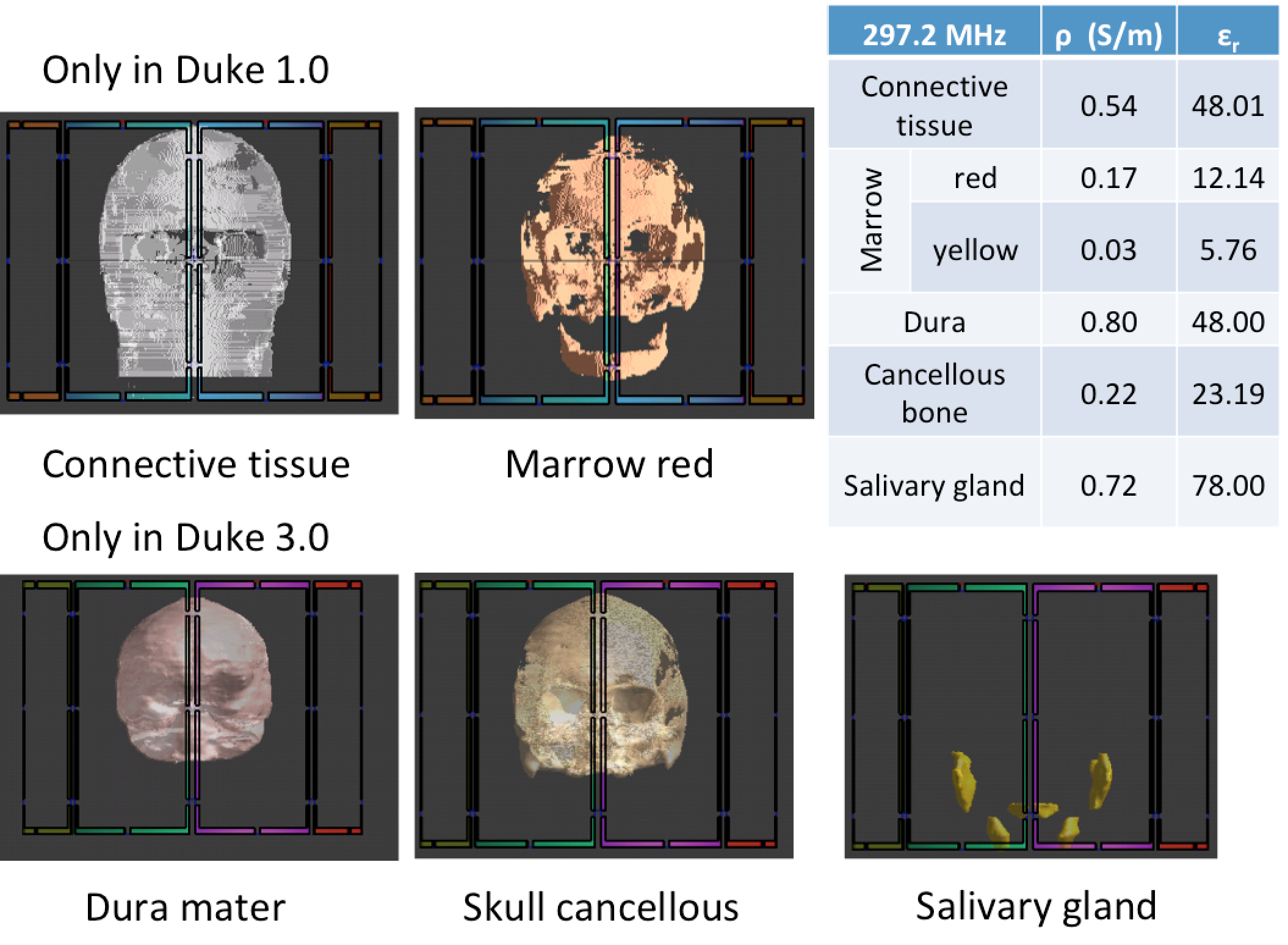
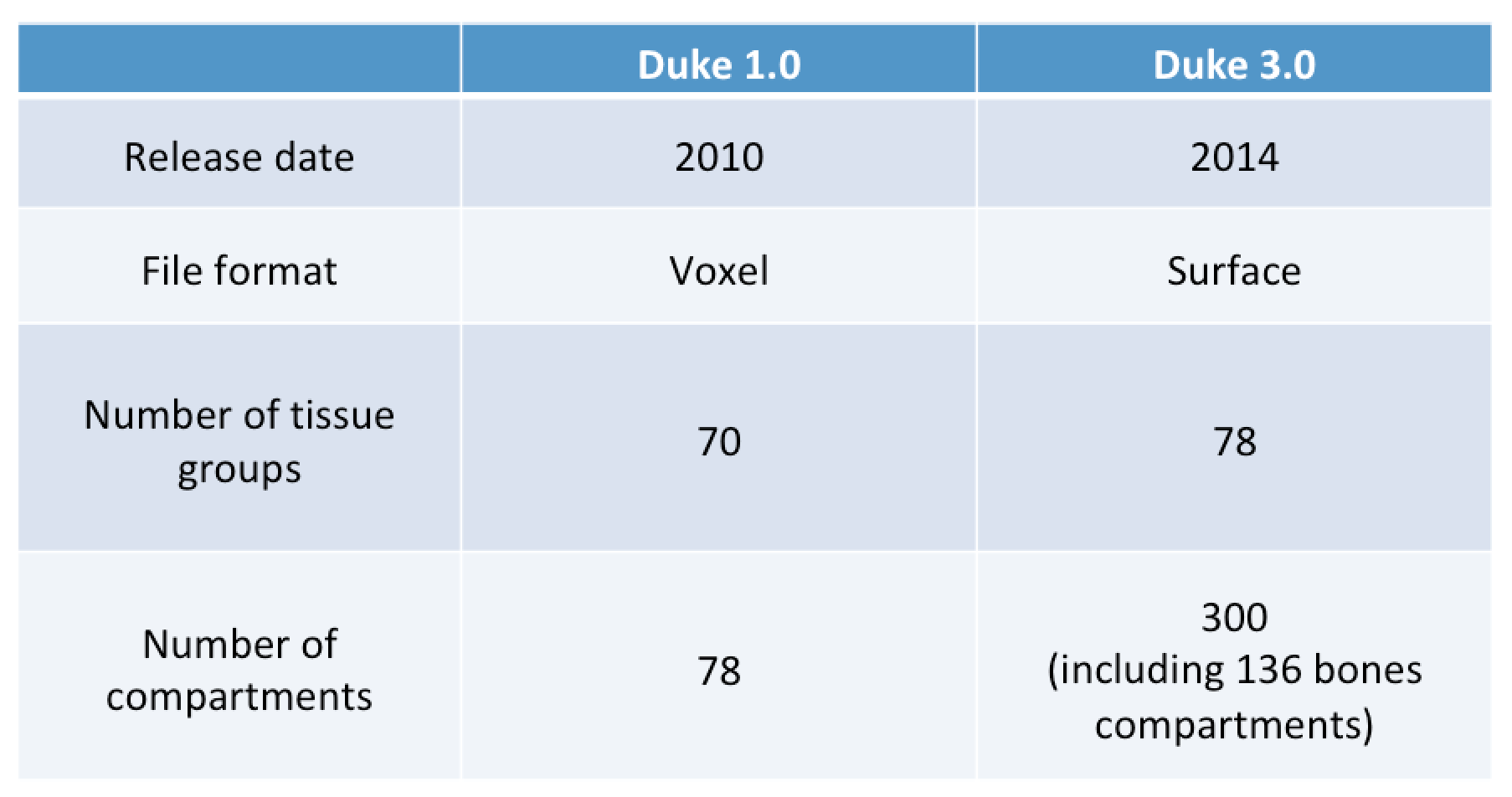
The two versions of the Duke model5 (v1.0, v3.0) that were used in this study are compared in Table 1. Duke version 1.0 is a voxel-based model that was introduced in 2010, with 78 tissue compartments in the whole body.6 Duke 3.0 was introduced in 2014 with a surface-based format5and a larger number of tissue and bone compartments, whereas the total number of tissue varieties used for electromagnetic (EM) simulation remained the same in the head region as for Duke v1.0. However, despite having the same overall number of tissue compartments, Duke v1.0 and v3.0 each have their own special tissue compartments, which are only available to the relevant version, as seen in Figure 1. Duke v1.0 contains a large volume of connective tissue around the bone regions, which is eliminated in Duke v3.0. Instead of connective tissue, Duke v3.0 newly segmented dura mater from bone which has different electrical properties (also available in MIDA7). Marrow red in Duke v1.0 was replaced with marrow yellow (for an adult) and skull (bone) is further segmented to cancellous and cortical skull. The salivary gland regions are segmented in v3.0.5 Sim4Life (ZMT, Switzerland) was used to calculate the SAR distribution, and a model of an 8-channel transceiver array coil (Affinity Imaging GmbH, Juelich, Germany) was incorporated. To simulate arbitrary pTx modes, a multiport simulation was performed, which calculates multiple identical simulations except for the appropriate excitation of each of the eight channels: each source is excited separately by adding 50 ohms resistances to the non-activated channels. The material properties of cancellous skull in Duke v3.0 were assigned as cortical bone to simplify it more closely to match Duke v1.0 as skull. For each of the three different models the SAR results were averaged to 10g mass voxels according to the IEEE/IEC 62704-1 standard using the dosimetry tool provided in Sim4Life, which are then converted in turn to 10g averaged Q-matrices.8 5,000 random B1+shim sets with random normalized amplitude (0-1) and phase (0-2p) were used to assess RF safety in pTx mode; all data were then averaged to 1 W total input power.Results
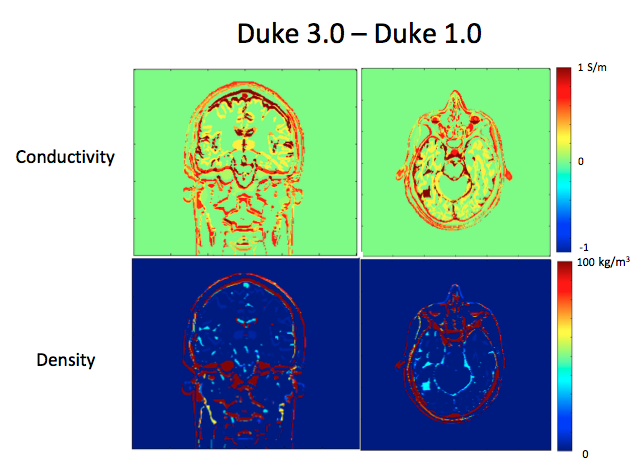
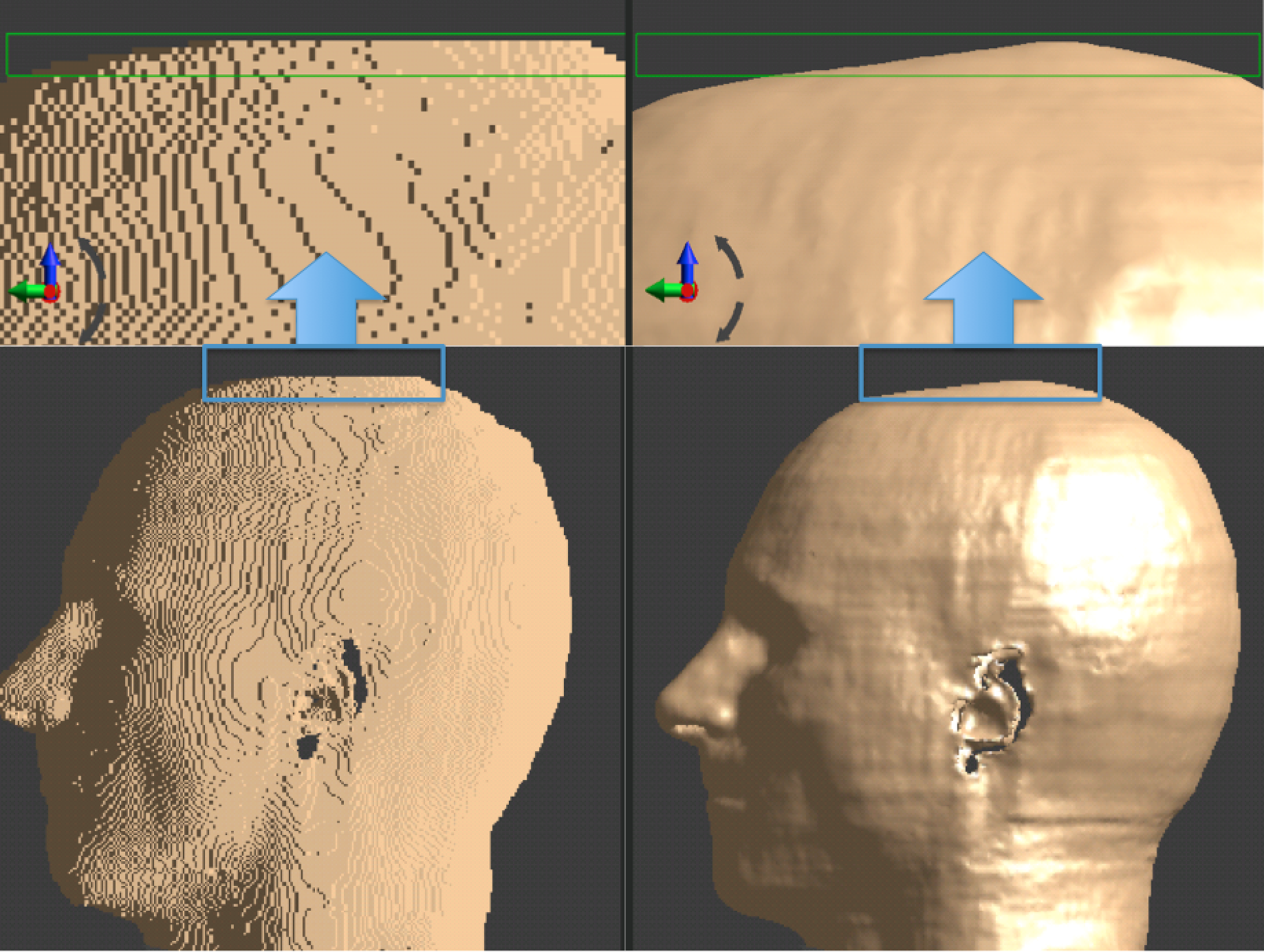
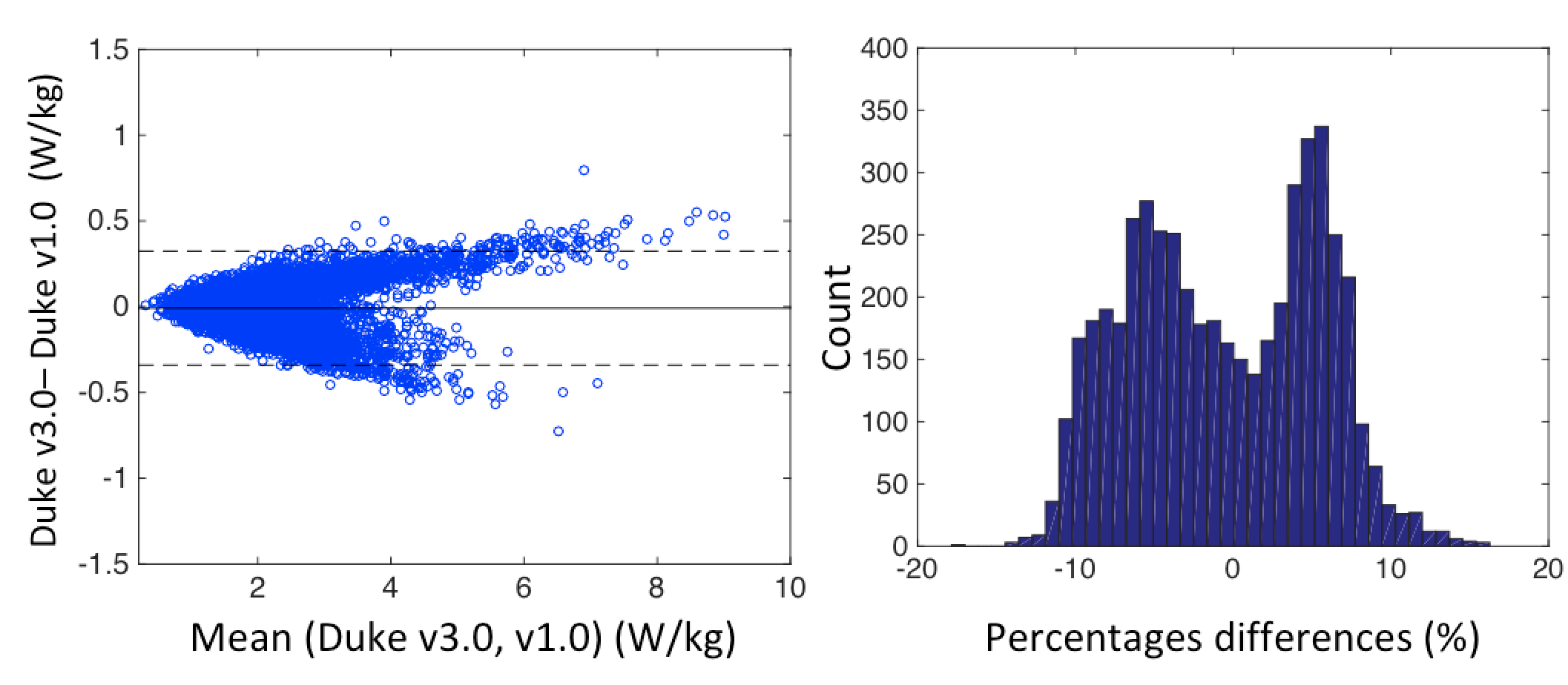
Figure 2 shows the differences in conductivity and density between Duke v1.0 and v3.0. Further detailed differences were found in brain grey-matter and white-matter regions, as well as differences at the edges that could potentially arise from model modification, or from differences coming from the voxel-based model versus the surface-based model. Figure 3 shows the differences between the voxel-based model and surface-based model, especially at the edge of the model. Figure 4. shows the results of the differences in maximum 10g SAR between the v1.0 and v3.0 Duke models, expressed as a Bland-Altman plot and as a histogram.Discussion
The results of EM simulation between Duke v1.0 and v3.0 were assessed in the context of pTx MRI. These models share identical morphometry, but have slightly different tissue segmentation. It is reported that improved SAR assessment is available using Duke version 3.0.5 The results of our study showed that up to 18% differences in worst-case SAR can be ascribed to having different tissue segmentations. This observation highlights that the use of Duke v1.0 (and v2.0 - a simplified version of Duke v1.0 and v3.0) or other voxel models with a limited number of tissue segmentation compartments can cause uncertainties in RF safety assessment in pTx MRI, even with no morphometric warping effect. Further studies are needed to understand the precise cause of these differences and the impact that the segmentation of different tissue compartments has on the calculated fields.Conclussion
We have demonstrated the effects and uncertainties caused by subtly different compositions of tissue compartments, even in the same morphological space. Choosing a dedicated voxel model with sufficient tissue compartments is as important as considering morphometric factors in RF safety modelling in pTx MRI.Acknowledgements
Oxford-Radcliffe Graduate Scholarship (University College Oxford) and Clarendon Fund.References
1. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: Sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952-962. doi:10.1002/(SICI)1522-2594(199911)42:5.
2. De Greef M, Ipek O, Raaijmakers AJE, Crezee J, Van Den Berg CAT. Specific absorption rate intersubject variability in 7T parallel transmit MRI of the head. Magn Reson Med. 2013;69(5):1476-1485. doi:10.1002/mrm.24378.
3. Seifert F, Wubbeler G, Junge S, Ittermann B, Rinneberg H. Patient safety concept for multichannel transmit coils. J Magn Reson Imaging. 2007;26(5):1315-1321. doi:10.1002/jmri.21149.
4. Jeong H, Andersson JLR, Hess AT, Jezzard P. A personalised SAR model for subject-specific RF safety. In: Proc. Intl. Soc. Mag. Reson. Med.; 2017.
5. Christ A, Kainz W, Hahn EG, et al. The Virtual Family - Development of surface-based anatomical models of two adults and two children for dosimetric simulations. Phys Med Biol. 2010;55(2). doi:10.1088/0031-9155/55/2/N01.
6. Gosselin MC, Neufeld E, Moser H, et al. Development of a new generation of high-resolution anatomical models for medical device evaluation: The Virtual Population 3.0. Phys Med Biol. 2014;59(18):5287-5303. doi:10.1088/0031-9155/59/18/5287.
7. Iacono MI, Neufeld E, Akinnagbe E, et al. MIDA: A multimodal imaging-based detailed anatomical model of the human head and neck. PLoS One. 2015;10(4). doi:10.1371/journal.pone.0124126.
8. Graesslin I, Homann H, Biederer S, et al. A specific absorption rate prediction concept for parallel transmission MR. Magn Reson Med. 2012;68(5):1664-1674. doi:10.1002/mrm.24138.
Figures