4148
129Xe Gas-Exchange MRI in Pediatrics with Lung Disease1Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States, 2Duke University, Durham, NC, United States, 3Philips, Cincinnati, OH, United States, 4University of Cincinnati, Cincinnati, OH, United States, 5Duke University Medical Center, Durham, NC, United States, 6University of Cincinnati Medical Center, Cincinnati, OH, United States
Synopsis
The solubility properties of hyperpolarized 129Xe have made it attractive in many translational pulmonary imaging studies; the large chemical-shift range can be exploited to obtain semi-quantitative ventilation, barrier-uptake, and RBC-transfer images. To date, the technique has demonstrated significant changes in gas exchange in adult lung disease, but has yet to be explored in children, where pulmonary function testing can be more challenging (or impossible). This pediatric gap caused us to pursue 129Xe gas-exchange MRI at the now-common field of 3T; here, we present the first demonstration of dissolved-phase xenon imaging in pediatrics (with cystic fibrosis and post-bone marrow transplant).
Purpose
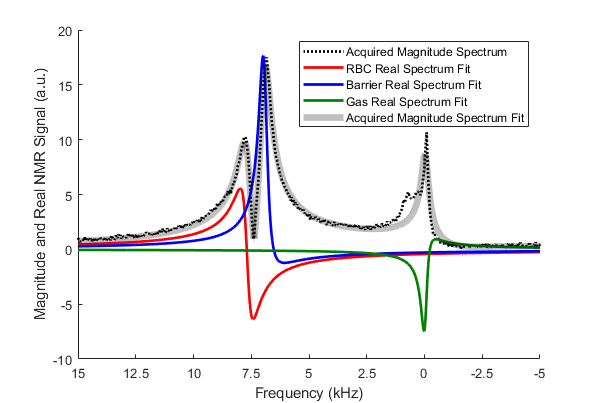
129Xe ventilation MRI correlates well with pulmonary function tests while being more sensitive to early disease, provides regional information, and been shown to be safe in pediatrics1–7. However, xenon also diffuses into the lung barrier (interstitium and pleura) and ultimately into red blood cells (RBCs), which can be measured directly as a proxy for gas exchange. Each environment provides a different chemical shift (Figure 1). With hyperpolarized 129Xe gas-exchange MRI, spatial mapping of barrier-uptake and RBC-transfer are possible and correlate with pulmonary diffusing capacity (DLCO) while providing regional information8–16. Here, we implement this technique for the first time in pediatric patients.Methods
A volume of 129Xe (86% enriched; ≈1/6 total lung capacity, capped at 1L) was hyperpolarized to 30-40% via a Polarean 9820 xenon polarizer; but decayed to 15-25% by the time of imaging. A sequence based on that reported for 3T was implemented on a Philips 3T Acheiva15. A 3D-radial sequence (643 matrix, (380mm)3 FOV, 0.6ms readout duration, middle-lobe-sinc excitation, pulse length=0.63ms, TR=6.5ms, 15s breath-hold, 770 radial views) was implemented with 10 interleaves (sweeps from +kz to -kz). TE was optimized before each scan to determine the TE90 (time for the barrier and RBC to be 90° out of phase, typically 0.48-0.52ms). Each k-space projection was repeated at three frequencies (each frequency with a different flip angle) before moving to the next trajectory; +7400Hz/15°, 0Hz/0.5°, and -7400Hz/15° (relative to gas-phase). Additionally, proton 3D-radial images (identical FOV/voxel, block pulse, 5° flip angle) were acquired for masking during an additional 15s breath-hold of air.
Five images (ventilation, gas phase, dissolved-phase, off-resonance, and proton) were reconstructed via Graphical Programming Interface into 1283 images17. Ventilation/proton images were reconstructed with a 1283-matrix kernel while the others used a 643-matrix kernel for higher SNR. In Matlab, the dissolved-phase image was separated into barrier and RBC images via the 1-point Dixon technique13. Ventilation images were normalized via their 99th percentile5. RBC and barrier images were normalized by the gas image, correcting for different flip angles, to obtain barrier-uptake and RBC-transfer images14. The ventilation, barrier-uptake, and RBC-transfer images were binned according to a previously-reported healthy mean and standard deviation5,14. Three subjects were imaged; 1) 12-year old female post-BMT without graft-vs-host (GVH) complications, 2) 15-year old male with cystic fibrosis, and 3) 25-year old female post-BMT with GVH complications of the lung.
Results
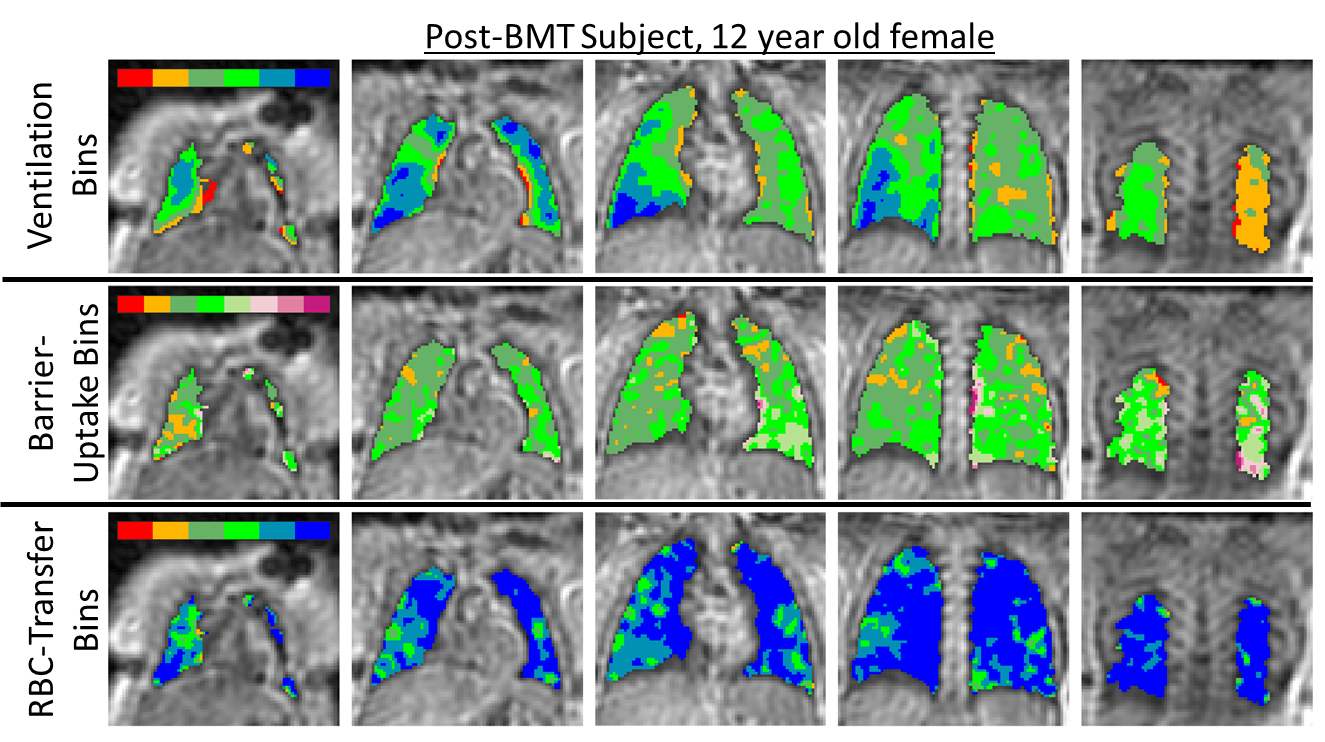
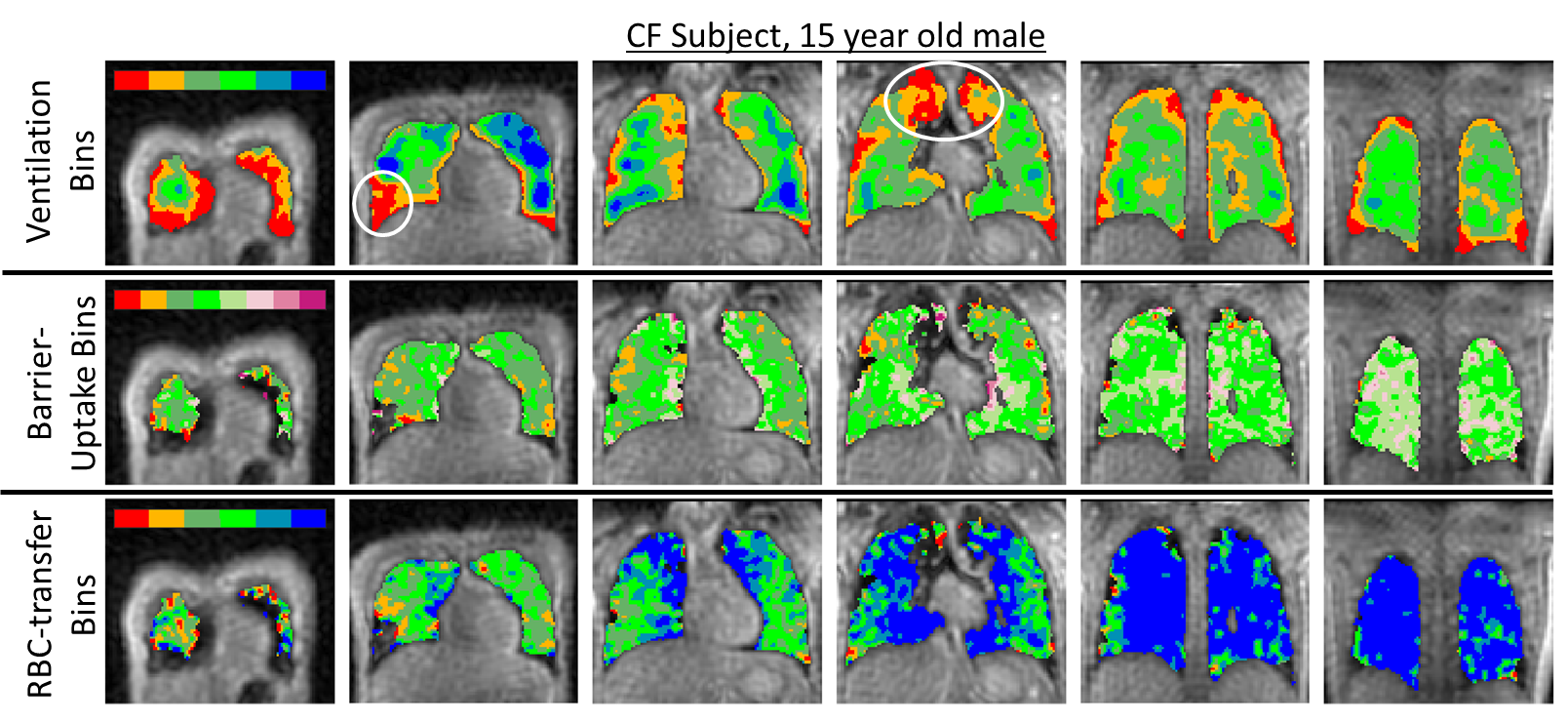
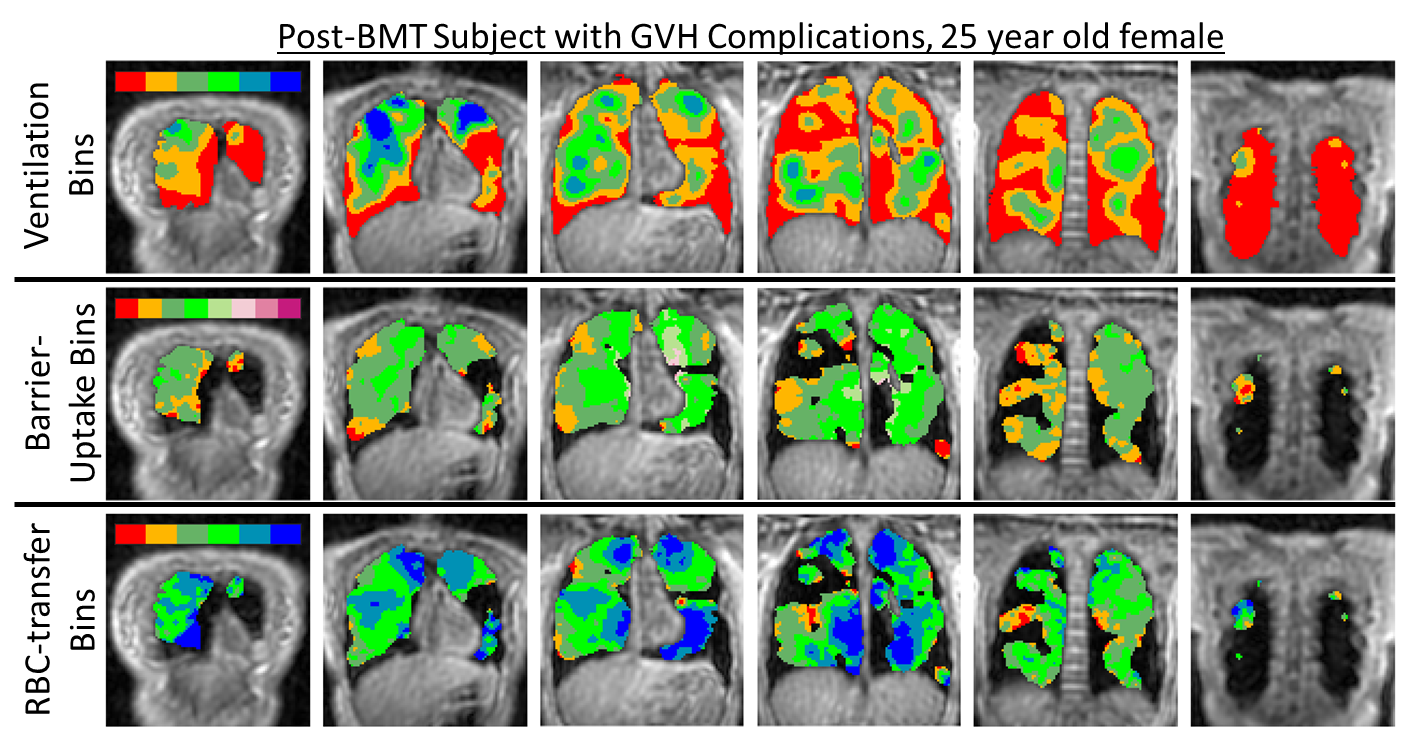
The resulting images had mean SNRs of 7.6±1.8, 27.6±6.9, 5.6±3.0, and 4.6±1.6 for high-resolution ventilation, low-resolution gas, barrier-uptake, and RBC-transfer, respectively. Binned maps are shown for the subjects (Figures 2, 3, and 4)14.
The post-BMT subject without GVH exhibited normal ventilation (1% complete-defect, 9% low-ventilation), a barrier-uptake of 0.0050±0.0013, an RBC-transfer of 0.0052±0.0014, and an RBC/barrier ratio of 1.1. The subject exhibits relatively homogeneous ventilation with few to no obstructive defects, indicative of healthy lungs.
The CF subject had impaired ventilation (11% complete-defect, 23% low-ventilation), a barrier-uptake of 0.0056±0.0017, an RBC-transfer of 0.0047±0.0021, and an RBC/barrier ratio of 1.0. The ventilation images exhibit defects in the right-lower lobe and apex of both lungs. The gas-exchange images have only minor deficit regions, indicative of minor gas-exchange impairment in ventilating regions (slightly increased barrier signal, decreased RBC signal, and corresponding decreased RBC/barrier ratio).
The post-BMT subject with GVH exhibited severely impaired ventilation (39% complete-defect, 28% low-ventilation), a barrier-uptake of 0.0043±0.0012, an RBC-transfer of 0.0034±0.0011, and an RBC/barrier ratio of 0.9. The ventilation defects affected most of the lung, barrier-uptake was moderately impaired, and RBC-transfer was severely diminished.
Discussion
The mean RBC-transfer is larger for all subjects when compared to previously-reported means at 1.5T14, though recently-published methods for 3T gas-exchange imaging also showed larger RBC-transfer15. Modifications of many parameters at 3T, including the use of smaller flip angles and longer TRs, would result in larger steady-state magnetization due to the decreased saturation of the dissolved-phase signals and longer time for the signals to diffuse from the gas and build-up in the barrier and RBCs. Thus, a distribution of gas-exchange MRI healthy subjects is necessary at 3T for quantitative comparison to those with gas-exchange-related lung disease.Conclusion
Gas-exchange MRI with HP 129Xe is possible in pediatrics with and without lung disease and provides additional regional measurements of pulmonary function. These results correspond well with previously-reported values in young adults. Additionally, the information provided via 129Xe gas-exchange MRI allows for functional imaging of interstitial or RBC-abnormalities that may not have ventilation deficits. Lastly, the technique provides means to asses regional lung function in pediatrics where standard clinical pulmonary function tests can be challenging or impossible.
Acknowledgements
The authors thank the following sources for research funding and support: NIH R01 HL131012 and NIH R44 HL123299.References
1. Driehuys B, Martinez-Jimenez S, Cleveland ZI, et al. Chronic obstructive pulmonary disease: safety and tolerability of hyperpolarized 129Xe MR imaging in healthy volunteers and patients. Radiology. 2012;262(1):279-289. doi:10.1148/radiol.11102172.
2. Virgincar RS, Cleveland ZI, Sivaram Kaushik S, et al. Quantitative analysis of hyperpolarized 129Xe ventilation imaging in healthy volunteers and subjects with chronic obstructive pulmonary disease. NMR Biomed. 2013;26(4):424-435. doi:10.1002/nbm.2880.
3. Horn FC, Tahir BA, Stewart NJ, et al. Lung ventilation volumetry with same-breath acquisition of hyperpolarized gas and proton MRI. NMR Biomed. 2014;27(12):1461-1467. doi:10.1002/nbm.3187.
4. He M, Robertson SH, Kaushik SS, et al. Dose and pulse sequence considerations for hyperpolarized 129Xe ventilation MRI. Magn Reson Imaging. 2015;33(7):877-885. doi:10.1016/j.mri.2015.04.005.
5. He M, Driehuys B, Que LG, Huang YCT. Using Hyperpolarized 129Xe MRI to Quantify the Pulmonary Ventilation Distribution. Acad Radiol. 2016;23(12):1521-1531. doi:10.1016/j.acra.2016.07.014.
6. Thomen RP, Walkup LL, Roach DJ, Cleveland ZI, Clancy JP, Woods JC. Hyperpolarized 129Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros. 2016. doi:http://dx.doi.org/10.1016/j.jcf.2016.07.008.
7. Walkup LL, Thomen RP, Akinyi TG, et al. Feasibility, tolerability and safety of pediatric hyperpolarized 129Xe magnetic resonance imaging in healthy volunteers and children with cystic fibrosis. Pediatr Radiol. 2016;46(12):1651-1662. doi:10.1007/s00247-016-3672-1.
8. Cleveland ZI, Cofer GP, Metz GM, et al. Hyperpolarized 129Xe MR imaging of alveolar gas uptake in humans. PLoS One. 2010;5(8):1-8. doi:10.1371/journal.pone.0012192.
9. Mugler JP, Altes TA, Ruset IC, et al. Simultaneous magnetic resonance imaging of ventilation distribution and gas uptake in the human lung using hyperpolarized xenon-129. Proc Natl Acad Sci. 2010;107(50):21707-21712. doi:10.1073/pnas.1011912107.
10. Kaushik SS, Freeman MS, Cleveland ZI, et al. Probing the regional distribution of pulmonary gas exchange through single-breath gas- and dissolved-phase 129 Xe MR imaging. J Appl Physiol. 2013;115(24):850-860. doi:10.1152/japplphysiol.00092.2013.
11. Qing K, Ruppert K, Jiang Y, et al. Regional Mapping of Gas Uptake by Blood and Tissue in the Human Lung using Hyperpolarized Xenon-129 MRI. J Magn Reson Imaging. 2014;39(2):346-359. doi:10.1002/jmri.24181.Regional.
12. Wang JM, Robertson SH, Wang Z, et al. Using Hyperpolarized 129 Xe MRI to Quantify Regional Gas Transfer in Idiopathic Pulmonary Fibrosis. 2015;162(3):561-567. doi:10.1016/j.jconrel.2012.07.004.Enhanced.
13. Kaushik SS, Robertson SH, Freeman MS, et al. Single-breath clinical imaging of hyperpolarized 129xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med. 2016;75(4):1434-1443. doi:10.1002/mrm.25675.
14. Wang Z, Robertson SH, Wang J, et al. Quantitative analysis of hyperpolarized 129 Xe gas transfer MRI. Med Phys. 2017;44(6):2415-2428. doi:10.1002/mp.12264.
15. Wang Z, Mu H, Bier EA, et al. Hyperpolarized 129Xe Gas Transfer MRI: The Transition from 1.5 to 3 Tesla. Magn Reson Med. 2017;0(0):1-23. doi:10.1002/mrm.27377.
16. Hahn AD, Kammerman J, Fain SB. Removal of hyperpolarized Xe gas-phase contamination in spectroscopic imaging of the lungs. Magn Reson Med. 2018. doi:10.1002/mrm.27349.
17. Zwart NR, Pipe JG. Graphical programming interface: A development environment for MRI methods. Magn Reson Med. 2015;74(5):1449-1460. doi:10.1002/mrm.25528.
Figures