4137
129Xe ventilation and 1H anatomical MRI to detect functional and structural abnormalities in sub-clinical cystic fibrosis lung disease1POLARIS, Academic Radiology, University of Sheffield, Sheffield, United Kingdom, 2Sheffield Children's Hospital NHS Foundation Trust, Sheffield, United Kingdom, 3Departments of Radiology and Medical Physics, University of Wisconsin, Madison, WI, United States, 4Cardiff University, Cardiff, United Kingdom, 5Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom, 6Respiratory research group, Division of infection, immunity and respiratory medicine, University of Manchester, Manchester, United Kingdom, 7Radiology and Nuclear Medicine department, Erasmus Medical Centre, Rotterdam, Netherlands, 8Paediatric Pulmonology Department, Sophia Children's hospital, Erasmus Medical Centre, Rotterdam, Netherlands
Synopsis
Lung MRI in cystic fibrosis (CF) has the potential to measure both structure and function during the same session. Here we assessed 14 patients with CF and normal spirometry for lung abnormalities using 129Xe ventilation and 1H 3D SPGR and UTE anatomical MRI. 129Xe ventilation defects were evident in all subjects assessed, whilst gas trapping was evident on expiratory 3D SPGR in 71% of patients. Further anatomical abnormalities were evident on UTE in 57% of patients. Ventilation and anatomical abnormalities are therefore present in sub-clinical CF and highlights the potential of MRI in routine CF lung imaging.
Introduction
Assessing lung disease early is key to maintaining lung health in cystic fibrosis (CF). There is great interest in lung MRI in CF, with the advantage over CT of being radiation free and capable of measuring both function and structure. Hyperpolarised gas ventilation MRI has been shown to be highly sensitive to early lung disease1,2 and 1H morphological MRI sequences such as ultra-short echo (UTE) have promising sensitivity to detect the lung pathology of interest in CF3. In combination, ventilation and anatomical MRI performed at the same visit may provide additional information that CT cannot achieve.
In this study, we retrospectively assessed a cohort of patients with CF and normal spirometry, and healthy controls to assess the ability of different MRI sequences to detect CF-related lung abnormalities. In particular, we aimed to assess the sensitivity of short duration breath-hold, 1H 3D spoiled gradient echo (SPGR) imaging performed at inspiration and expiration to detect gas trapping (a key feature in early CF lung disease) in CF when compared to controls.
Methods
14 children and adults with CF and normal FEV1 (>-1.64 z-scores) and five healthy control children were assessed. All MR imaging was performed on a 1.5T HDx GE scanner. All subjects performed 129Xe ventilation MR imaging using a 3D steady-state free precession (SSFP) sequence at end-inspiratory tidal volume by inhaling a pre-determined volume of gas (129Xe and N2) from functional residual capacity. 129Xe voxel size=3.3*3.3*10mm3, bandwidth=16kHz, TE/TR=2.2/6.7ms, flip angle=10°. The volume of 129Xe and the total volume inhaled was scaled based on standing height (129Xe volume=0.4-0.67L, bag volume=0.4-1.0L). At the same visit, all subjects underwent 3D SPGR and UTE 1H MRI using an 8-element cardiac array. 3D SPGR was acquired at both total lung capacity (TLC) and residual volume (RV) (breath-hold ~10seconds, 3mm isotropic voxel size, TE=0.7ms, TR=1.8ms, FA=3°); while 3D radial UTE was acquired during free-breathing with prospective respiratory bellows gating as previously described4 (images were reconstructed to 1.36mm isotropic voxel size). During the same visit, subjects with CF also performed multiple-breath washout to calculate lung clearance index (LCI)5 and spirometry to calculate FEV16. 129Xe MRI was segmented using a semi-automated method7 to calculate the ventilation defect percentage (VDP). 129Xe and 1H MRI were reviewed by an experienced chest radiologist, using a binary method for the presence or absence of; ventilation defects, bronchial wall abnormalities, mucus plugging, sacculations or abscesses, collapse or consolidation and gas trapping.Results
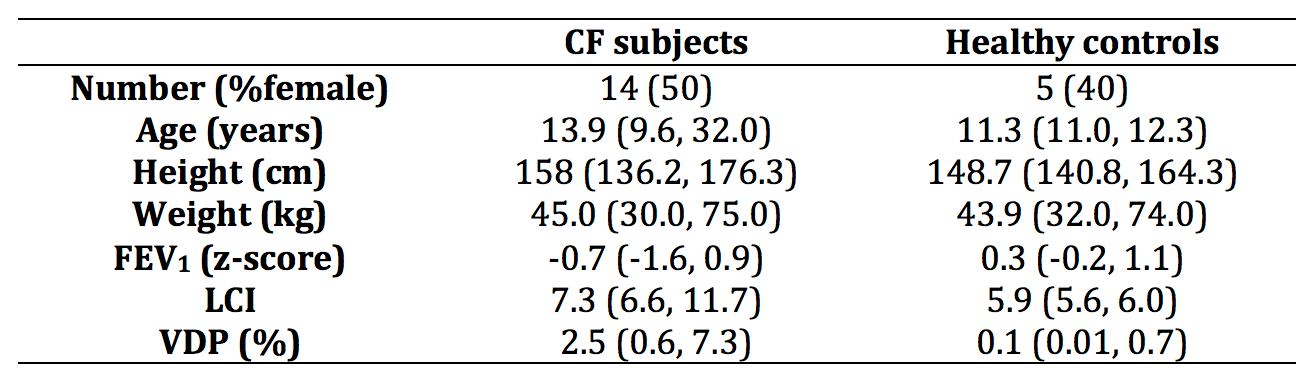
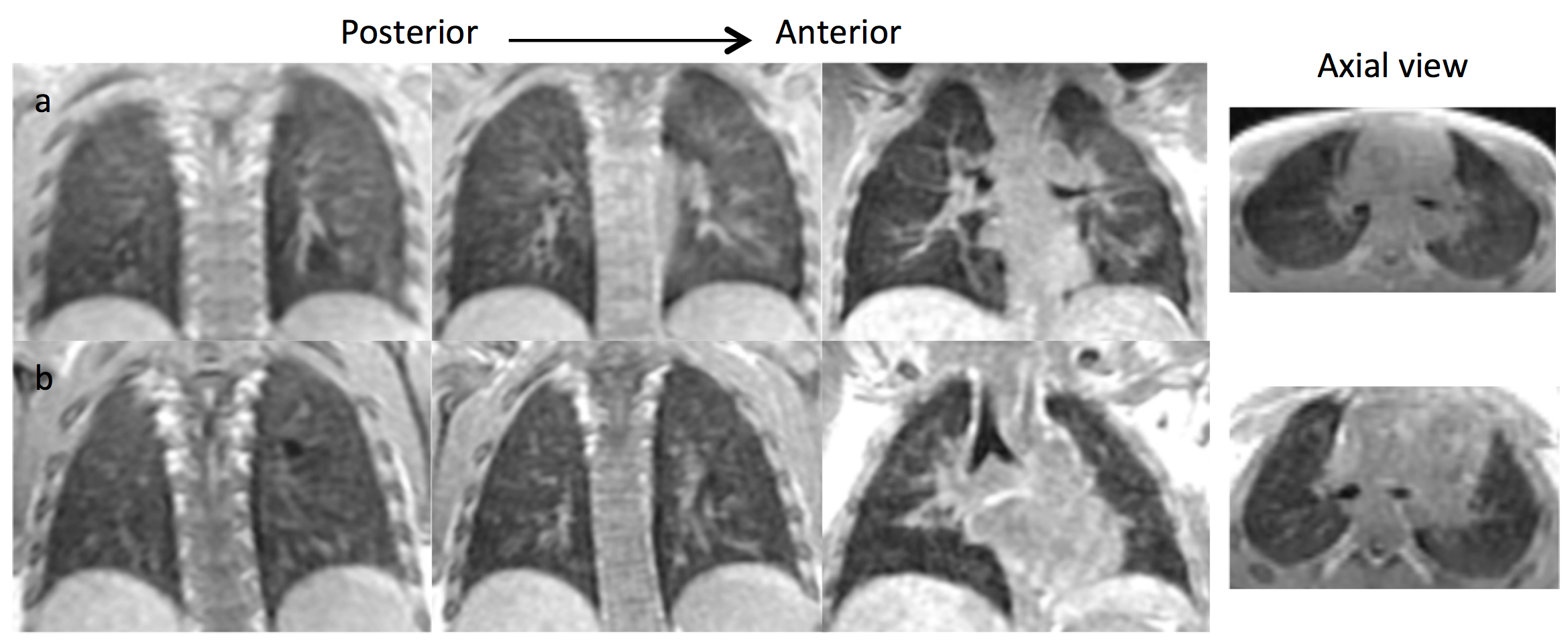
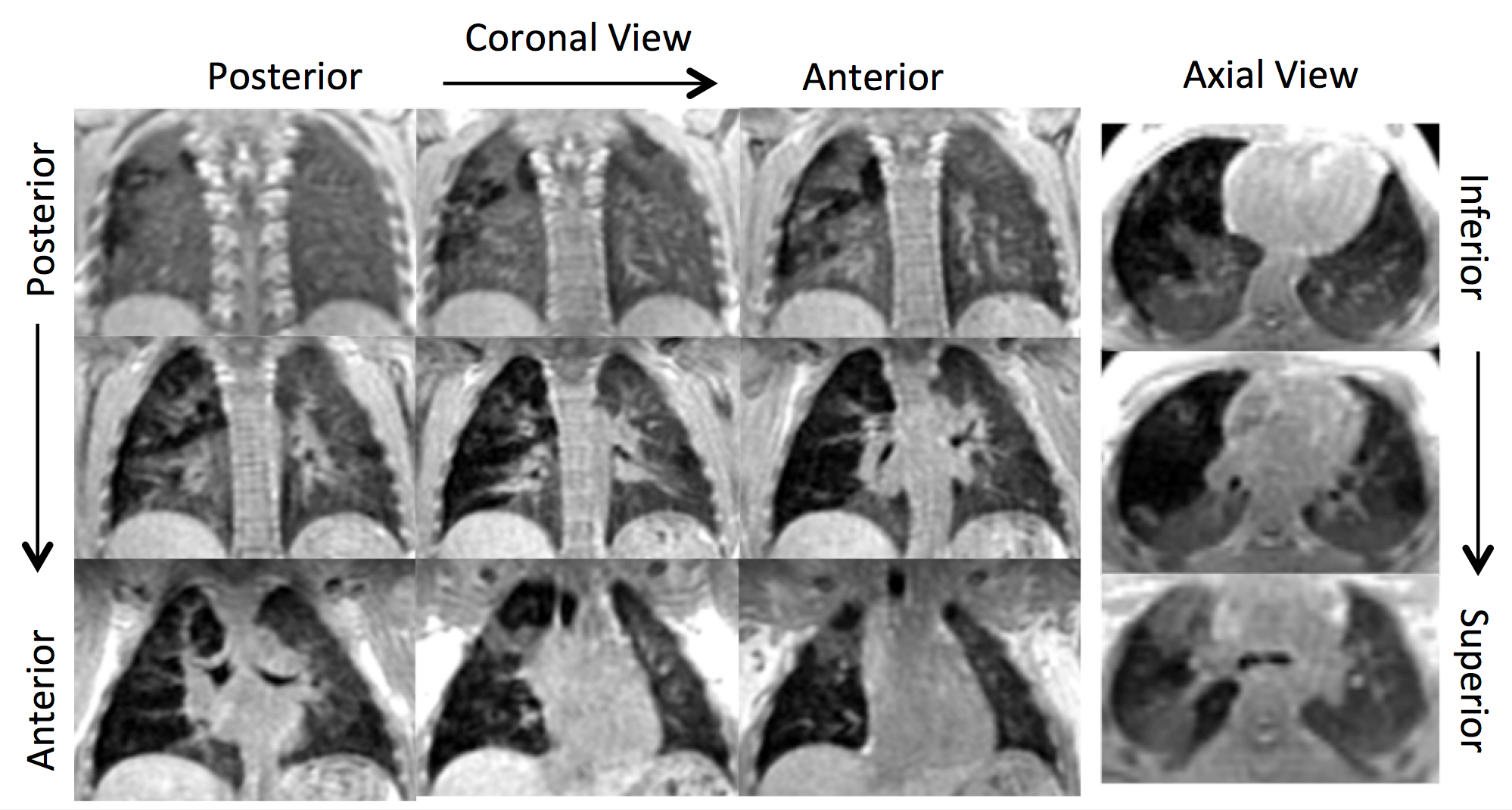
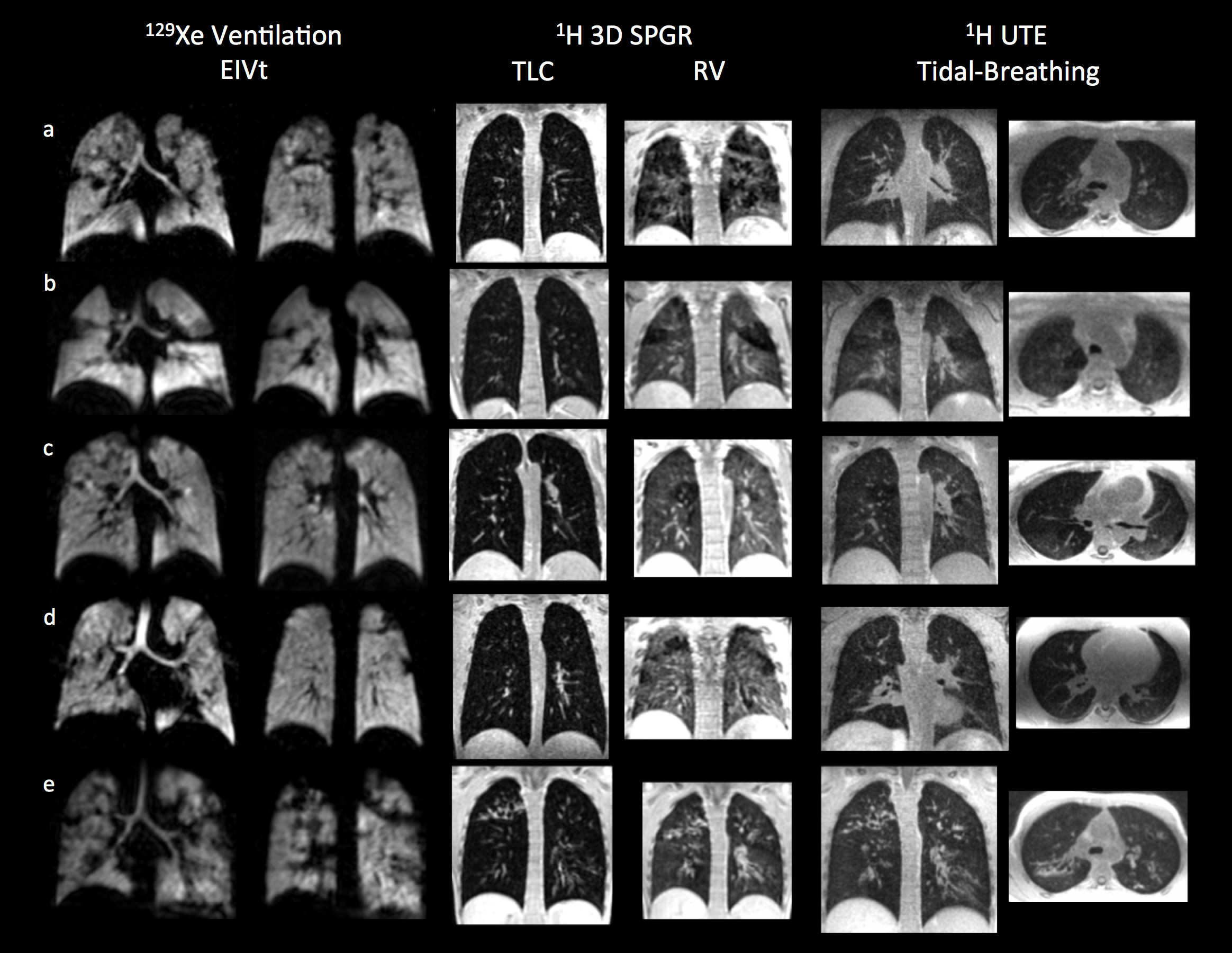
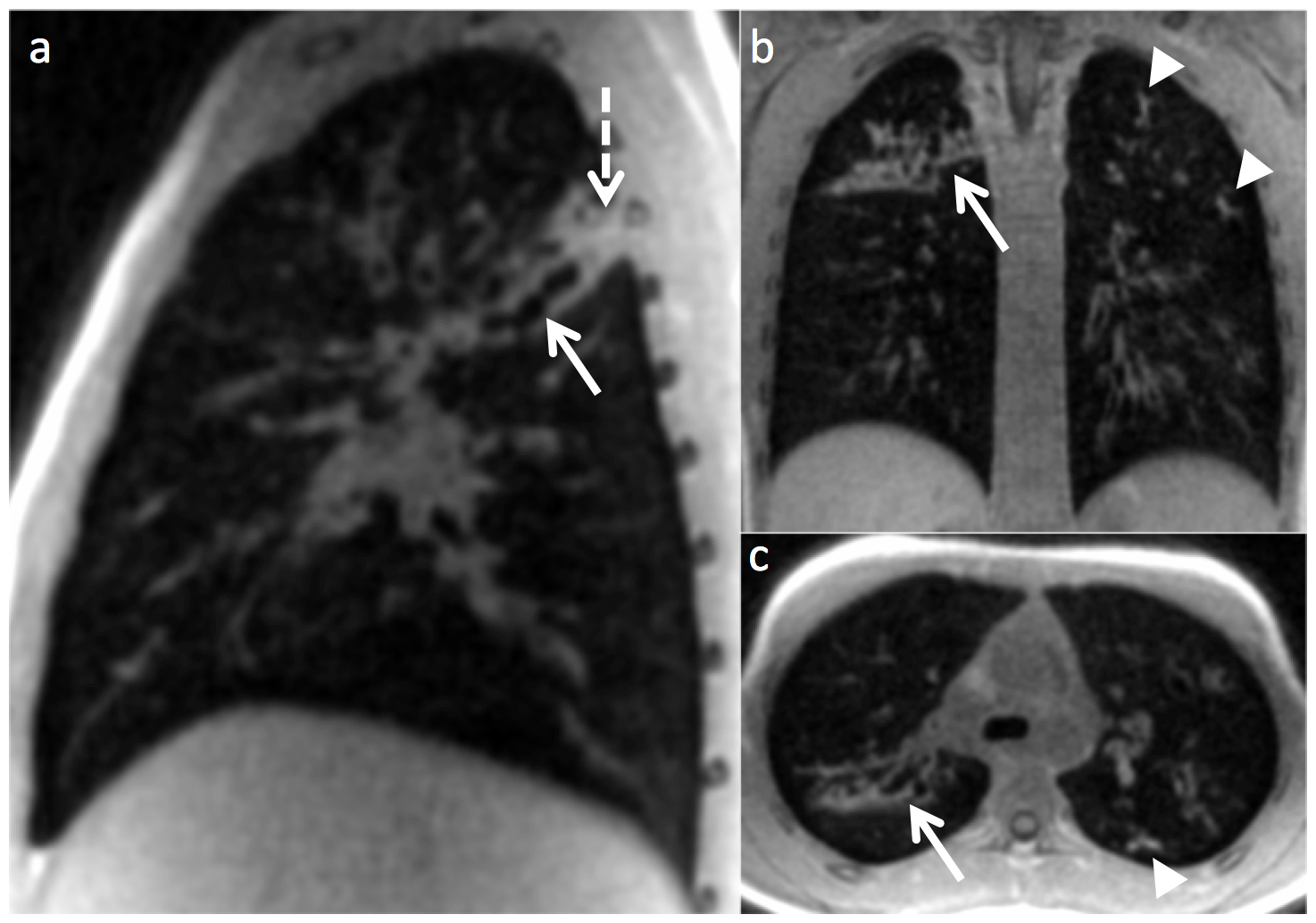
Subject demographics, lung function and MRI metrics are documented in Table 1. All subjects had an FEV1 within the normal range. All control subjects had normal LCI, and visibly normal 129Xe and 1H MR images (Figure 1). In contrast, 6/14 (43%) CF subjects had an abnormal (>7.4) LCI. All CF subjects had visible ventilation defects evident on 129Xe MRI, and VDP was significantly higher when compared to controls (p<0.001). 3D SPGR 1H MRI at RV demonstrated gas trapping in 10/14 (71%) patients (Figures 2 and 3). UTE 1H MRI analysis demonstrated; bronchial wall abnormalities in 3/14 (21%) patients, mucus plugging in 6/14 (43%), sacculations or abscesses in 0/14 and collapse or consolidation in 7/14 (50%). Figure 4 highlights UTE 1H MRI findings from one patient with bronchiectasis, mucus plugging and consolidation evident.Discussion
There is increasing evidence for the utility of both functional and structural MRI in the routine assessment of patients with CF. In this analysis we highlight that in patients with normal spirometry and even with normal LCI, that abnormalities can be evident in ventilation as seen on 129Xe MRI, but also in structural MRI. The degree of signal heterogeneity evident at RV on 3D SPGR 1H MRI in 71% of patients highlights the ability to detect gas trapping as a key feature of early lung disease during a short breath-hold sequence. In this cohort, we were able to detect one or more other structural abnormalities in 57% of patients, with the most frequent abnormality detected being collapse or consolidation in 50% of patients. Due to the retrospective nature of this analysis we were unable to assess CT in parallel to determine the true sensitivity of these 1H images to detect abnormality.Conclusion
In patients with CF and normal FEV1, functional and anatomical abnormalities can be assessed and detected at the same visit in approximately 30-45mins using both free-breathing and breath-hold MRI sequences. This highlights the future potential of MRI in the routine imaging of CF lung disease.Acknowledgements
The authors would like to acknowledge all members of the POLARIS research group at the University of Sheffield for the support. In particular we would like to thank Mrs Leanne Armstrong for administrative support. We would also like to thank the Cystic Fibrosis clinical teams at Sheffield Children’s Hospital, Sheffield Teaching Hospital and Manchester CF Centre for their support. Finally we would like to thank all of the participants for their time in taking part in this researchReferences
1. Marshall H, Horsley A, Taylor CJ, et al. Detection of early subclinical lung disease in children with cystic fibrosis by lung ventilation imaging with hyperpolarised gas MRI. Thorax 2017;72(8):760-62. doi: 10.1136/thoraxjnl-2016-208948
2. Thomen RP, Walkup LL, Roach DJ, et al. Hyperpolarized (129)Xe for investigation of mild cystic fibrosis lung disease in pediatric patients. J Cyst Fibros 2017;16(2):275-82. doi: 10.1016/j.jcf.2016.07.008
3. Roach DJ, Cremillieux Y, Fleck RJ, et al. Ultrashort Echo-Time Magnetic Resonance Imaging Is a Sensitive Method for the Evaluation of Early Cystic Fibrosis Lung Disease. Annals of the American Thoracic Society 2016;13(11):1923-31. doi: 10.1513/AnnalsATS.201603-203OC
4. Johnson KM, Fain SB, Schiebler ML, et al. Optimized 3D ultrashort echo time pulmonary MRI. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 2013;70(5):1241-50. doi: 10.1002/mrm.24570
5. Horsley AR, Gustafsson PM, Macleod KA, et al. Lung clearance index is a sensitive, repeatable and practical measure of airways disease in adults with cystic fibrosis. Thorax 2008;63(2):135-40. doi: 10.1136/thx.2007.082628
6. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. The European respiratory journal 2012;40(6):1324-43. doi: 10.1183/09031936.00080312
7. Hughes PJC, Horn FC, Collier GJ, et al. Spatial fuzzy c-means thresholding for semiautomated calculation of percentage lung ventilated volume from hyperpolarized gas and (1) H MRI. J Magn Reson Imaging 2018;47(3):640-46. doi: 10.1002/jmri.25804
Figures