4121
A comparative study of multi-shot diffusion-weighted imaging (DWI) using multiplexed sensitivity encoding (MUSE) and conventional single-shot echo-planar imaging (EPI) DWI in breast cancer1Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 2Global Research Organisation, GE Healthcare, Buckinghamshire, United Kingdom, 3Department of Radiology, Addenbrooke's Hospital, Cambridge, United Kingdom
Synopsis
MUSE (multiplexed sensitivity encoding) is a multi-shot echo-planar imaging (EPI) technique used in diffusion-weighted imaging (DWI) that reduces distortion and blurring compared to single-shot EPI. Experiments using a breast phantom aimed to investigate the effect of varying parallel acceleration and number of shots on geometric distortion and quantification of the apparent diffusion coefficient (ADC). A refined protocol was applied to a small cohort of patients to comparatively assess improvements in image quality.
Introduction
Diffusion-weighted imaging (DWI) is increasingly used in the detection and characterisation of breast cancer and it is typically performed using single-shot echo-planar imaging (ss-EPI), however spatial resolution is limited by distortion and blurring due to T2* decay during readout. MUSE (multiplexed sensitivity encoding) (1) is a segmented-EPI technique that acquires k-space in a number of ‘shots’, reducing the echo train length and therefore the degree of blurring and distortion. MUSE acquires segments of k-space with an interleaved trajectory and uses existing sensitivity encoding techniques (SENSE) (2) to reconstruct the full field-of-view (FOV) image. To date, this technique has not been investigated in the breast, though a number of studies have investigated the improvement in image quality and diagnostic performance of RESOLVE, a readout-segmented EPI technique (3,4).
Studies using a breast phantom aimed to investigate MUSE, used in conjunction with parallel acceleration, to quantify the apparent diffusion coefficient (ADC) and assess geometric distortion. We evaluated the reduction in distortion using the Mattes mutual information (MI) metric (5). We used this method to determine an optimised parallel acceleration factor and number of shots for MUSE-DWI. The optimised protocol was then applied to a small number of patients to assess improvements in image quality compared to standard ss-EPI.
Methods
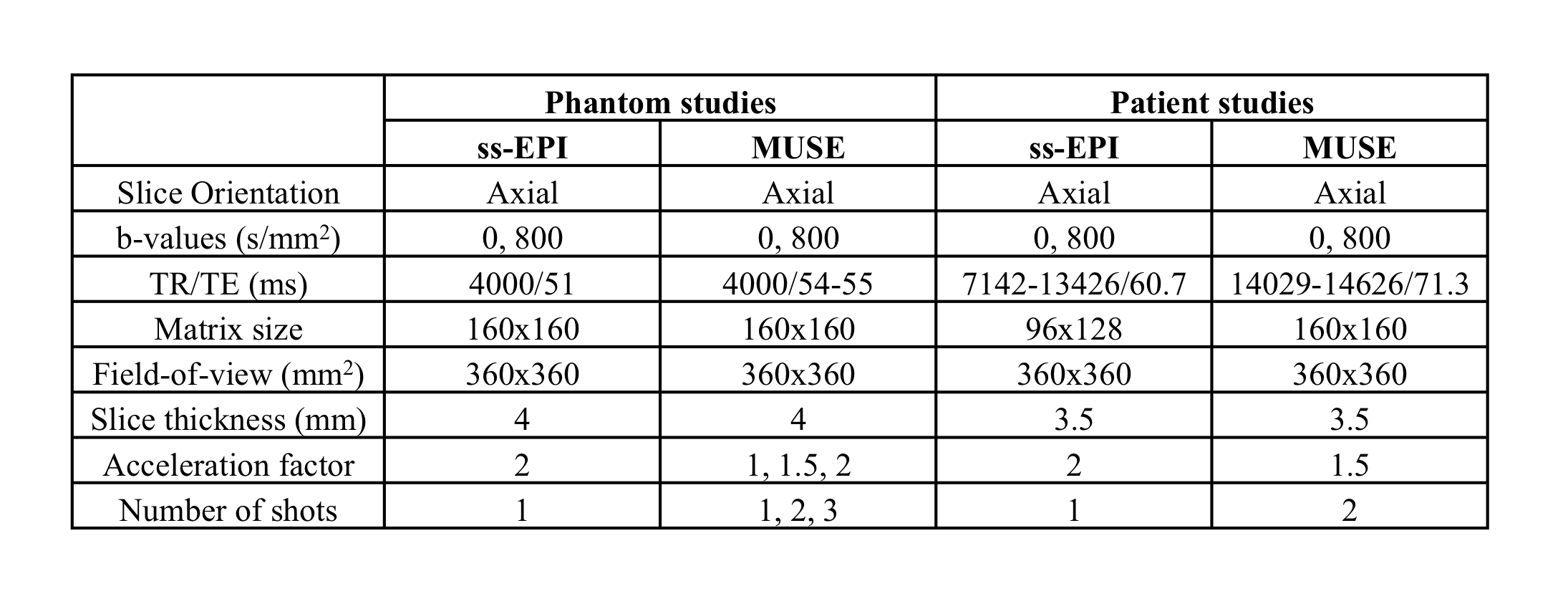
Phantom Study: Imaging of a breast phantom (High Precision Devices, Inc., Boulder, CO ) was performed on a 3T system (MR 750, GE Healthcare, Waukesha, WI) using an 8-channel breast coil. The phantom contained 16 vials of varying concentrations of polyvinylpyrrolidone (PVP) to mimic the diffusion properties of malignant and benign breast tumours. DWI was performed using ss-EPI and 6 permutations of MUSE-DWI with varying parallel acceleration factors and numbers of shots (see Table 1). A proton density weighted image (TR/TE = 2500/7.75ms, matrix = 512x512, slice thickness = 3.5mm) was acquired using a fast spin echo sequence as a geometrical reference.
Patient Study: To date, n=3 patients with pathologically confirmed breast cancer have been scanned using MUSE as part of a prospective study approved by our local review and ethics boards. Imaging was performed on a 1.5T system (MR 450W, GE Healthcare, Waukesha, WI) using an 8-channel breast coil. ss-EPI DWI and MUSE-DWI were performed (see Table 1). The MRI protocol also included T2-weighted, T1-weighted fast spin echo (FSE) and a DCE sequence.
Data analysis: Generation of ADC maps and diffusion analyses were carried out using in-house software developed in MATLAB (version R2018b). Regions of interest (ROIs) were drawn around each vial in Osirix (version 8.0.1, www.osirix-viewer.com). The mean ADC of each vial was calculated for each acquisition and the coefficient of variation calculated between all acquisitions. A measurement of distortion was obtained by calculating the MI metric between the b = 800 s/mm2 and proton density weighted images. For patient studies, both ss-EPI and MUSE images were scored based on three criteria: lesion conspicuity (1-5), contrast between lesion and tissue (1-5) and diagnostic confidence (1-3). Lesions were also given a BI-RADS score (6). Regions of interest were drawn in Osirix by a breast radiologist with reference to DCE images and mean ADC values calculated for the whole tumour volume.
Results
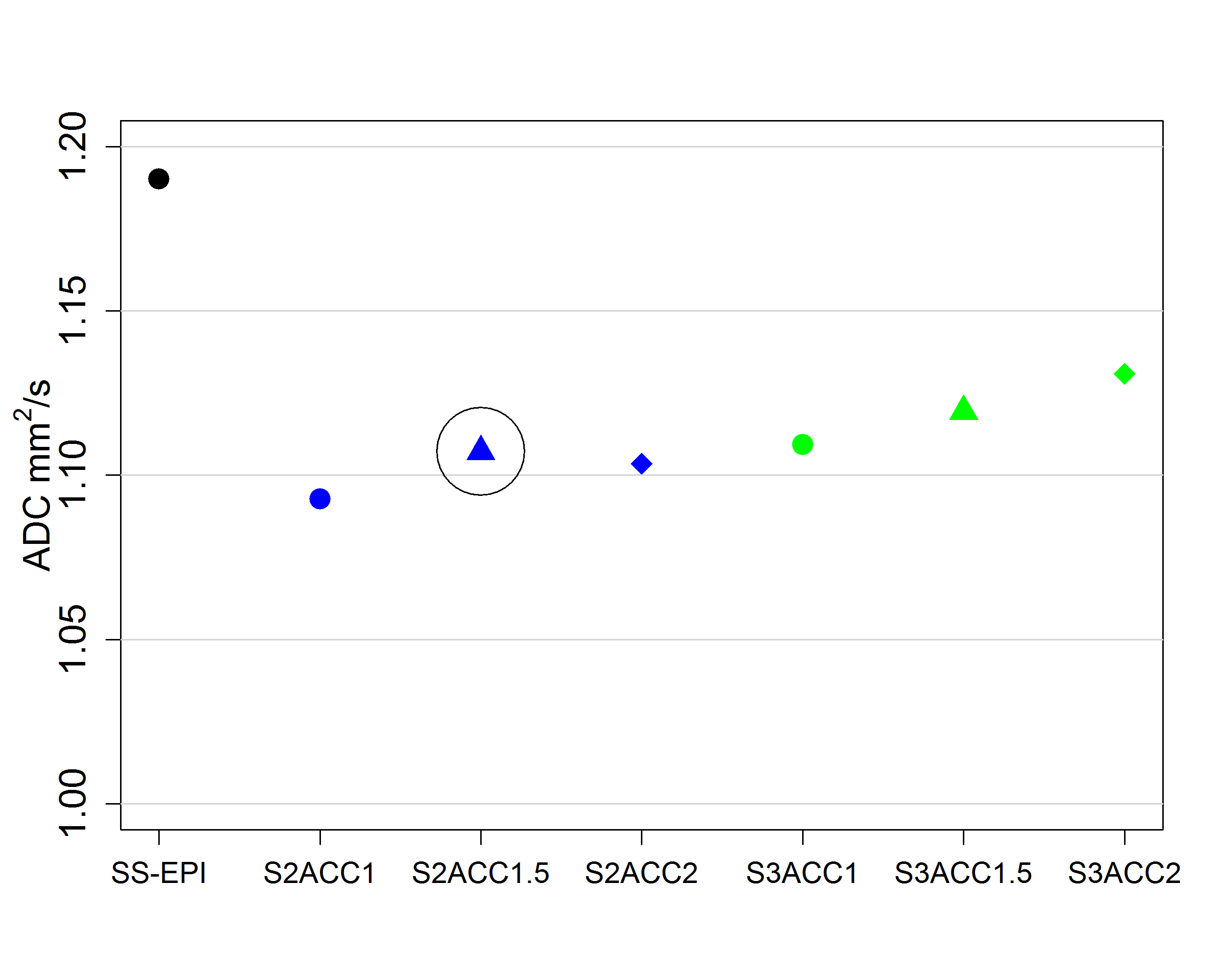
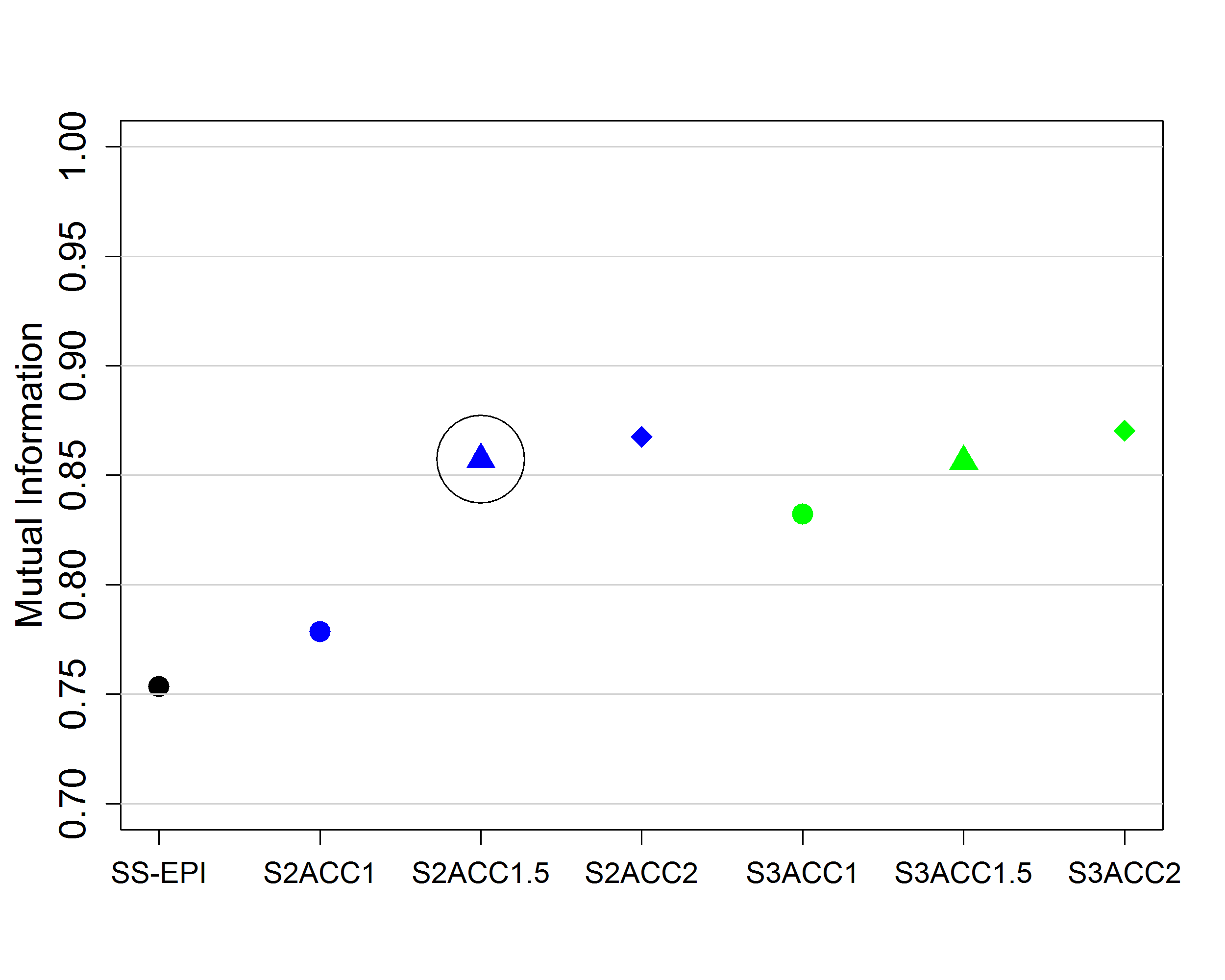
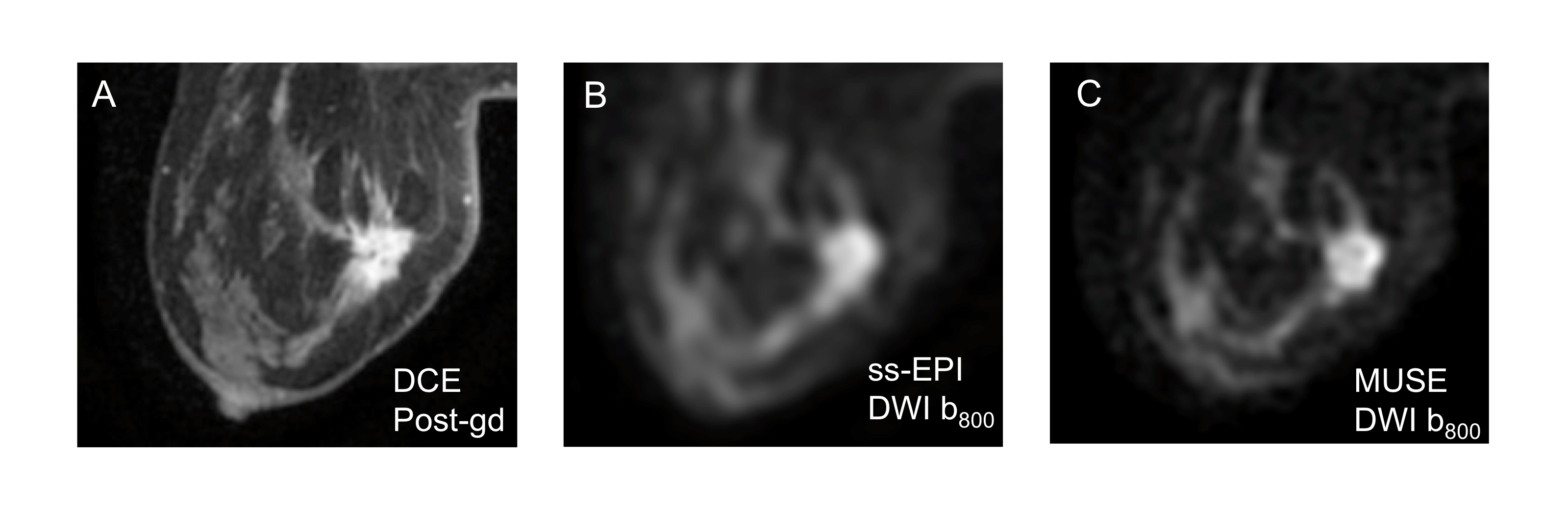
There was a low coefficient of variation (< 2%) in ADC values measured for each acquisition at all PVP concentrations (Figure 1). Acquisitions using MUSE achieved a greater MI metric than when using ss-EPI. MI increased with number of shots and parallel acceleration factor (Figure 2). 3 women (mean age 48.7 years, age range, 45-51 years) were successfully imaged. Malignant lesions included two invasive ductal carcinomas and one invasive lobular carcinoma. A comparison of image quality for an invasive ductal carcinoma is shown in Figure 3. Results of qualitative comparisons are given in Table 2. MUSE was superior to ss-EPI in all criteria for image quality.Discussion
Measurements of the ADC are similar when using ss-EPI or MUSE. While distortion was reduced using MUSE, increasing the number of shots increases the length of the acquisition substantially. An acceleration factor of 1.5 and 2 shots were chosen for clinical implementation as a compromise between acquisition time and image quality. Further development to reduce acquisition time and additional patient recruitment are required and subsequent work will evaluate if the improvement is statistically significant on a target sample size. Qualitatively, MUSE has shown improvement in clinical image quality compared to ss-EPI.Conclusion
MUSE is a promising technique to improve the image quality and clinical utility of DWI. Low patient numbers limit the conclusions that can be drawn from this study at present.Acknowledgements
No acknowledgement found.References
1. Chen N-K, Guidon A, Chang H-C, Song AW. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage 2013;72:41–7 doi: 10.1016/j.neuroimage.2013.01.038.
2. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn. Reson. Med. 1999;42:952–62.
3. Kim YJ, Kim SH, Kang BJ, et al. Readout-segmented echo-planar imaging in diffusion-weighted mr imaging in breast cancer: comparison with single-shot echo-planar imaging in image quality. Korean J. Radiol. 2014;15:403–10 doi: 10.3348/kjr.2014.15.4.403.
4. Wisner DJ, Rogers N, Deshpande VS, et al. High-resolution diffusion-weighted imaging for the separation of benign from malignant BI-RADS 4/5 lesions found on breast MRI at 3T. J. Magn. Reson. Imaging 2014;40:674–681 doi: 10.1002/jmri.24416.
5. Mattes D, Haynor DR, Vesselle H, Lewellen TK, Eubank W. PET-CT image registration in the chest using free-form deformations. IEEE Trans. Med. Imaging 2003;22:120–128 doi: 10.1109/TMI.2003.809072.
6. Taylor K, Britton P, O’Keeffe S, Wallis MG. Quantification of the UK 5-point breast imaging classification and mapping to BI-RADS to facilitate comparison with international literature. Br. J. Radiol. 2011;84:1005–10 doi: 10.1259/bjr/48490964.
Figures