4120
Focal areas of NME undergoing MRI-guided VABB: outcomes and frequency of malignancy1Radiology, Stanford University, Stanford, CA, United States, 2Radiology, St Marianna university school of medicine, Kawasaki, Japan
Synopsis
We evaluated the positive predictive values (PPVs) of internal enhancement and kinetic data in focal areas of non-mass enhancement (NME) in patients undergoing MRI-guided vacuum-assisted breast biopsy (MRI-VABB). Our results show the PPVs of clumped and heterogeneous internal enhancement were similar (PPV=25% vs 21%) suggesting that heterogeneous internal is similar to clumped enhancement. The most predictive kinetic pattern of malignancy was fast initial phase without any tendency for cancer using the delayed phase.
INTRODUCTION Magnetic Resonance Imaging (MRI) of the breast has high sensitivity, and is an important modality for the detection and characterization of breast cancer1-3. Because MRI of the breast has moderate specificity4, MRI-VABB is required, and the decision to perform biopsy or not is important clinically. Of all breast lesions, NME is less likely to be detected at second-look US than mass lesions5. Therefore, we have to consider utilization of MRI-VABB of suspicious NME. The first BI-RADS Lexicon contained the term “focal area” of NME, which was dropped in the 2013 BI-RADS Edition6. The “focal area NME” was several foci assembled in a small area, unique compared to the rest of the breast. Previous studies of NME showed that a segmental distribution was most frequently associated with malignancy7-9, with focal and linear distributions of intermediate suspicion. Prior studies on NME did not mention if the NME was in a focal area or the results of MRI- VABB10-13. Of other morphologies, clustered ring and clumped NME are suspicious7,8,14-16. However, the relative suspicion of other internal enhancement characteristics were not clear. Furthermore, the kinetic analysis is known to be of less diagnostic value for NME than for masses 15,17-21. The purpose of this study was to evaluate frequency of malignancy in focally distributed NME, to identify significant predictors of malignancy and determine results of MRI-VABB in these lesions.
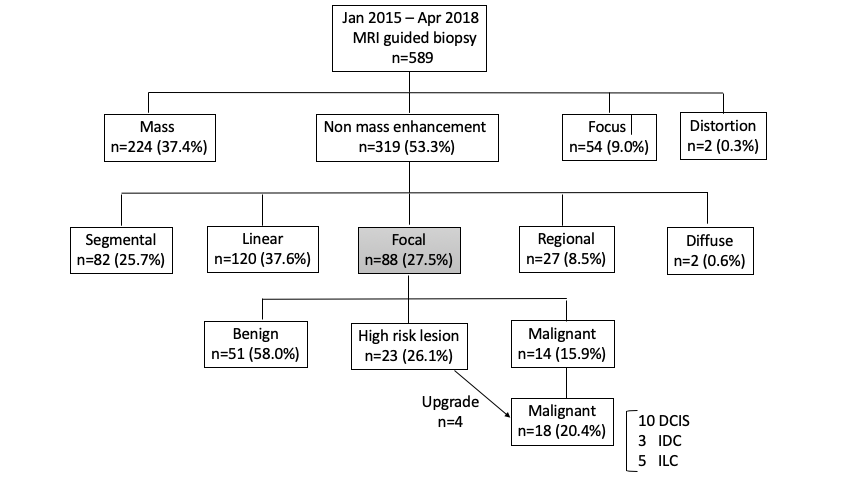
MATERIALS AND METHODS We retrospectively reviewed 589 lesions undergoing 9-gauge MRI-VABB from January 2015 to April 2018. We collected patient demographics, risk factors and indications, breast MRI BI-R ADS descriptors, histopathological diagnosis at MRI-VABB and surgical excision in case of high-risk lesions. We selected patients with NME that was focally distributed, describing if the NME had clumped, clustered ring, heterogeneous or homogeneous internal enhancement. When available the initial kinetics (slow, medium, fast), and delayed kinetics (persistent, plateau, wash out) was recorded for each lesion. The x2 test and Fisher exact tests were performed for univariate analysis.
RESULTS Of the total 589 lesions, there were 319 (53.3%) NME lesions. Among the 319 lesions, 88 (27.5%) showed NME in a focal distribution. The 88 focal NME ranged between 0.4 to 4.2cm with median dimension of 1.25cm. Of these, 40 (45.5%) showed clumped, 38 (43.2%) showed heterogenous, 9 (10.2%) showed homogeneous and 1 (1.1%) showed clustered ring enhancement. Among the 88 focal distribution NME lesions, 51 (58.0%) were benign, 23 (26.1%) were high-risk lesions and 14 (15.9%) were malignancies. 15/23 (65.2%) high risk lesions were excised. 4/15 (26.7%) were upgraded to malignancy (2 atypical ductal hyperplasia (ADH), 2 atypical lobular hyperplasia (ALH)). There were 18 malignancies, 10 were DCIS, 3 were invasive ductal carcinoma, 5 were invasive lobular carcinoma. The cancer yield of focal distribution was 20.4% (18/88). The PPV of clumped and heterogenous internal enhancement was 25% and 21% retrospectively. There were no malignancies with clustered ring and homogeneous internal enhancement. With kinetic curve data, 22/88 (25%) in initial phase and 14 (15.9%) in delayed phase had unknown data. 12/18 (66.7%) lesions with biopsy proven malignancy demonstrated rapid initial phase. There was no tendency with delayed phase.
DISCUSSION In previous studies, clustered ring and clumped internal enhancement is suspicious for malignancy, with clustered ring enhancement as the strongest predictive descriptor for malignancy7,8,14-16. In our study, there was only 1 clustered ring enhancement in focally distributed NME. Clumped and heterogeneous internal enhancement was suspicious for malignancy (PPV=25% vs 21%). In previous studies, PPVs of clumped and heterogeneous ranged from 20 to 32.8% and 5.1 to 25% 14, 22-23. On the other hand, homogeneous internal enhancement is less suspicious for malignancy.
CONCLUSION Our data show that MRI guided VABB in focally distributed NME is indicated not only for clumped internal enhancement but also for heterogenous internal enhancement. The most predictive kinetic pattern of malignancy was a rapid initial phase.
Acknowledgements
No acknowledgements foundReferences
1. Orel SG, Schnall MD. MR imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology 2001;220(1):13–30.
2. Van Goethem M, Schelfout K, Dijckmans L, Van Der Auwera JC, Weyler J, Verslegers I, Biltjes I, De Schepper A .MR mammography in the pre-operative staging of breast cancer in patients with dense breast tissue: comparison with mammography and ultrasound. Eur Radiol 2004;14:809-816.
3. Kuhl CK, Schrading S, Bieling HB, et al. MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet 2007;370:485-92.
4. Peter NH, Borel Rinkes IH, Zuithoff NP, et al. Meta-analysis of MR imaging in the diagnosis of breast lesions. Radiology 2008;246: 116-24.
5. Spick C, Baltzer, P. A. Diagnostic utility of second-look US for breast lesions identified at MR imaging: systematic review and meta-analysis. Radiology 2014;273(2):401-409.
6. Morris EA, Comstock C, Lee C, et al. ACR BI-RADS–magnetic resonance imaging 2013. In: ACR BI-RADS Atlas Breast Im -aging Reporting and Data System. 5th ed. Reston, Va: American College of Radiology, 2014;58:13–15.
7. Tozaki M, Igarashi T, Fukuda K. Breast MRI using the VIBE sequence: clustered ring enhancement in the differential diagnosis of lesions showing non-mass-like enhancement. AJR Am J Roentgenol. 2006;187:313–21.
8. Tozaki M, Fukuda K. High-spatial-resolution MRI of non-mass like breast lesions: interpretation model based on BI-RADS MRI descriptors. AJR Am J Roentgenol 2006;187:330– 337.
9. Yuen S, Uematsu T, Masako K, Uchida Y, Nishimura T. Segmental enhancement on breast MR images: differential diagnosis and diagnostic strategy. Eur Radiol. 2008;18:2067–75.
10. Orel SG, Rosen M, Mies C, Schnall MD. MR imaging-guided 9-gauge vacuum-assisted core-needle breast biopsy: initial experi -ence. Radiology 2006;238(1):54–61.
11. Spick C , Schernthaner M, Pinker K, et al. MR-guided vacuum-assisted breast biopsy of MRI-only lesions: a single center experience. Eur Radiol 2016;26(11):3908-3916.
12. Ferré R , Ianculescu V, Ciolovan L, et al. Diagnostic performance of MR-guided vacuum-assisted breast biopsy: 8 years of experience. Breast J;2016:22:83– 89.
13. Verheyden C , Pages-Bouic E, Balleyguier C, et al. Underestimation rate at MR imaging-guided vacuum-assisted breast biopsy: a multi-institutional retrospective study of 1509 breast biopsies.Radiology 2016;281(3):708-719.
14. Sakamoto N, Tozaki M, Higa K, Tsunoda Y, Ogawa T, Abe S, et al. Categorization of non-mass-like breast lesions detected by MRI. Breast Cancer. 2008;15:241–6.
15. Uematsu T, Kasami M. High-spatial-resolution 3-T breast MRI of nonmasslike enhancement lesions: an analysis of their features as significant predictors of malignancy. AJR Am J Roentgenol. 2012;198:1223–30. 16. Asada T, Yamada T, Kanemaki Y, Fujiwara K, Okamoto S, Nakajima Y. Grading system to categorize breast MRI using BI-RADS 5th edition: a statistical study of non-mass enhancement descriptors in terms of probability of malignancy. Japanese journal of radiology 2018; 36(3): 200-208.
17. D. Newell, K. Nie, J.H. Chen, et al., Selection of diagnostic features on breast MRI to differentiate between malignant and benign lesions using computer-aided diagnosis: differences in lesions presenting as mass and non-mass-like enhancement, Eur. Radiol. 2010;20 (4) 771–781.
18. M. Goto, H. Ito, K. Akazawa, et al., Diagnosis of breast tumors by contrast-enhanced MR imaging: comparison between the diagnostic performance of dynamic enhancement patterns and morphologic features, J. Magn. Reson. Imaging 2007;25 (1) 104–112.
19. Gutierrez RL, DeMartini WB, Eby PR, Kurland BF, Peacock S, Lehman CD. BI-RADS lesion characteristics predict likelihood of malignancy in breast MRI for masses but not for nonmasslike enhancement. AJR Am J Roentgenol. 2009;193:994–1000.
20. S.A. Jansen, X. Fan, G.S. Karczmar, et al., DCEMRI of breast lesions: is kinetic analysis equally effective for both mass and nonmass-like enhancement? Med. Phys. 2008;35 (7) 3102–3109.
21. C. Kuhl, The current status of breast MR imaging. Part I. Choice of technique, image interpretation, diagnostic accuracy, and transfer to clinical practice Radiology 2007;244(2):356-78.
22. Mahoney MC, Gatsonis C, Hanna L, DeMartini WB, Lehman C. Positive predictive value of BI-RADS MR imaging. Radiology. 2012;264:51–8.
23. Gity M, Ghazi Moghadam K, Jalali AH, Shakiba M. Asso -ciation of different MRI BIRADS descriptors with malignancy in non mass-like breast lesions. Iran Red Crescent Med J. 2014;16:e26040.
Figures