4116
Adaptation of a Computer Vision Blur Metric to Objectively Compare High Resolution DWI Strategies in in vivo Breast Imaging1Biomedical Engineering, University of Minnesota, Minneapolis, MN, United States, 2Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 3Radiology, University of Minnesota, Minneapolis, MN, United States
Synopsis
DWI has shown promise for detecting and characterizing breast cancers but is limited by the low spatial resolution of standard spin-echo EPI techniques. Several strategies have been proposed to generate high resolution DWI, including reduced field-of view, steady-state imaging, readout-segmented EPI, and simultaneous multi-slice imaging (SMS). In this work we adopt the Crété-Roffet blur metric to objectively compare resolution of three DWI strategies, including standard SE-EPI, and RO-segmented EPI and SMS-EPI high resolution approaches. In this comparison, both high-resolution DWI methods showed an improvement in in-plane resolution over the standard technique. The Crété-Roffet blur metric appears to be a robust and objective means of comparing effective resolution.
Introduction
While diffusion weighted imaging (DWI) has shown promise for breast cancer treatment[1] the low spatial resolution of the standard technique (spin-echo (SE)-EPI) limits lesion detection and biases apparent diffusion coefficients (ADCs) due to partial volume effects. Several strategies have been proposed to generate high resolution DWI, including reduced field-of-view[2], steady-state imaging[3], readout-segmented EPI[4], and simultaneous multi-slice imaging (SMS)[5,6]. It is important to objectively compare techniques throughout development to guide protocol optimization. However, comparing resolution can be difficult for several reasons: nominal resolution does not reliably reflect the true image resolution due to blurring effects from off-resonance and T2*-decay, especially in EPI; subjective assessment is laborious and prone to bias[7]; and phantom assessments cannot fully replicate all in vivo sources of blurring. This work adapts an objective measurement from the computer vision field, the Crété-Roffet metric[8], to assess the resolution of several DWI strategies. The Crété-Roffet metric quantitatively measures blurring from 0 (sharp) to 1 (blurry) and has previously been validated against subjective blur assessment.
Purpose: To compare the resolution of three different breast DWI protocols using the Crété-Roffet method.
Methods
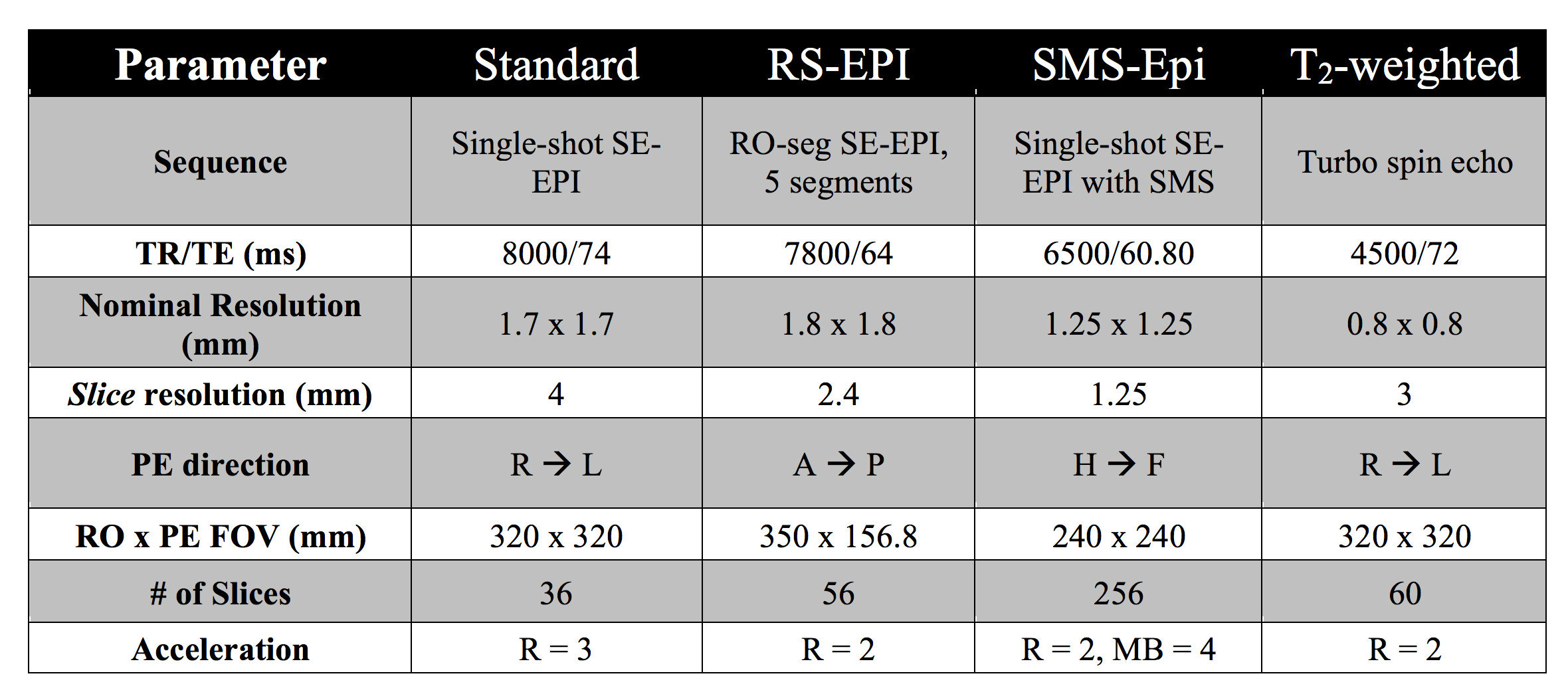
Fifteen breast cancer patients were scanned under an IRB-approved protocol on a Siemens 3T PrismaFit using a 16-channel Sentinelle breast coil. DWI was acquired with 3 protocols, each constrained to a 5-minute acquisition: standard single-shot SE-EPI (Std) following the ACRIN 6698 protocol[9], readout-segmented EPI (RS-EPI) with 5 segments based on Wisner et al.’s protocol[2], and a simultaneous multi-slice (SMS) acquisition acquired sagittally and reformatted axially[6]. A standard anatomical T2-weighted image (T2w) was included for comparison. All protocols were repeated on a quantitative breast phantom[10] that includes a resolution grid and tissue mimics. Table 1 provides sequence details.
Image processing was performed in Matlab using DICOM (magnitude) images. Because each protocol was acquired with different nominal resolutions, all images were resampled onto a common 0.5 mm isotropic grid (smaller than any nominal resolution). The blur metric was calculated independently for each Cartesian direction.
Results
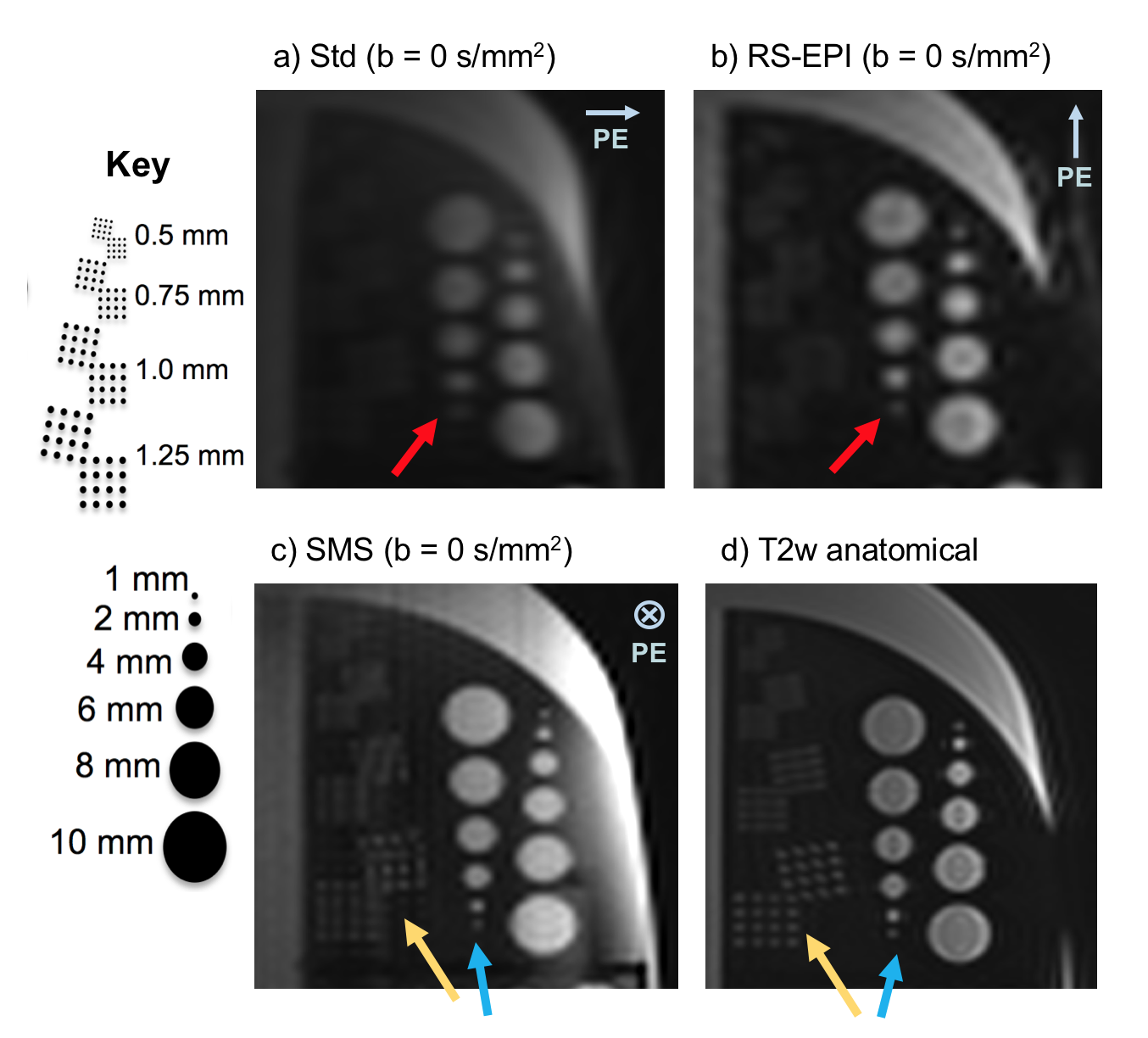
Figure 1 shows axial b=0 s/mm2 DWI and T2w images of the breast phantom resolution grids. The 2 mm feature (red) is barely detectible in the Std approach and readily visible with RS-EPI. While SMS-DWI can detect the smallest 1 mm feature (blue) and 1.25 mm grid (yellow), they are sharpest in the anatomical T2w image.
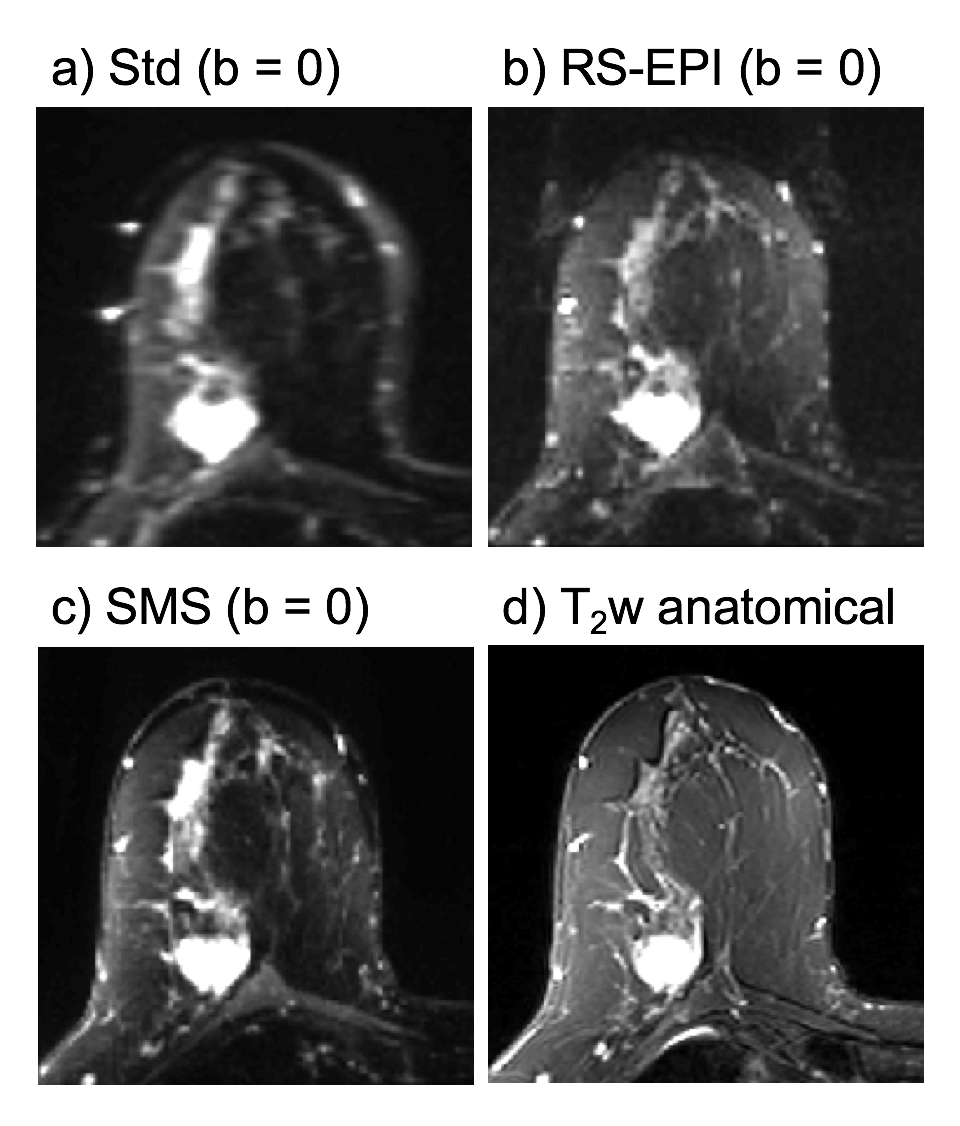
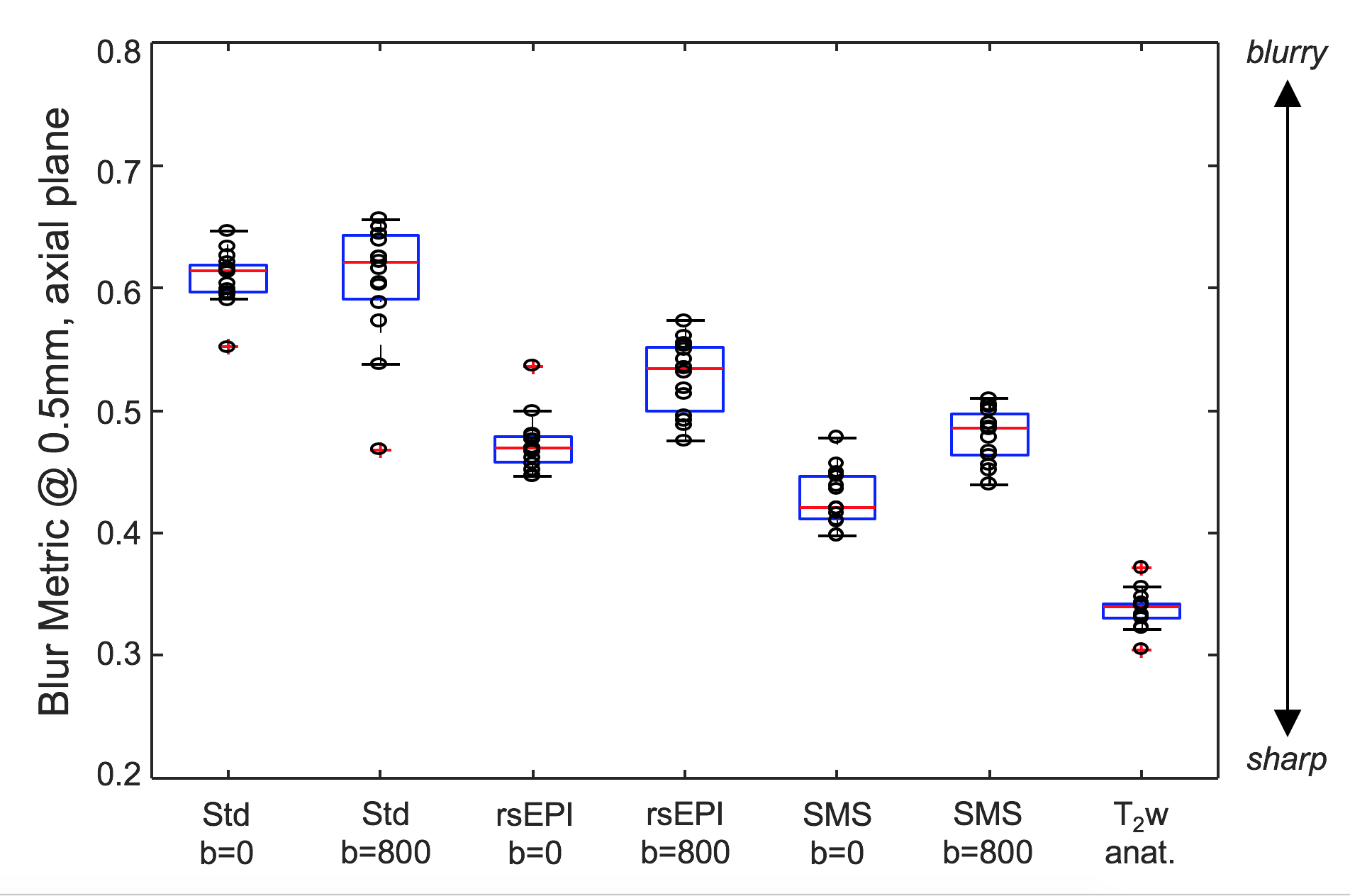
Figure 2 shows the three DWI methods and the T2w anatomical image from an example in vivo case after resampling to a 0.5 mm common grid. The increase in effective resolution from (a) to (d) can be readily observed. Figure 2 shows the blur metric measured in the axial plane (average of right-left and anterior-posterior) for the three DWI methods at both b=0 and 800 s/mm2, and also for the T2w image. Consistent with Figures 1 and 2, T2w shows the least blurring, followed by SMS-EPI, RS-EPI, and finally the standard SE-EPI technique. Note that the b=800 image is more blurry than b=0 for all DWI methods due to increased relative fat signal, eddy currents, and averaging over respiratory cycles.
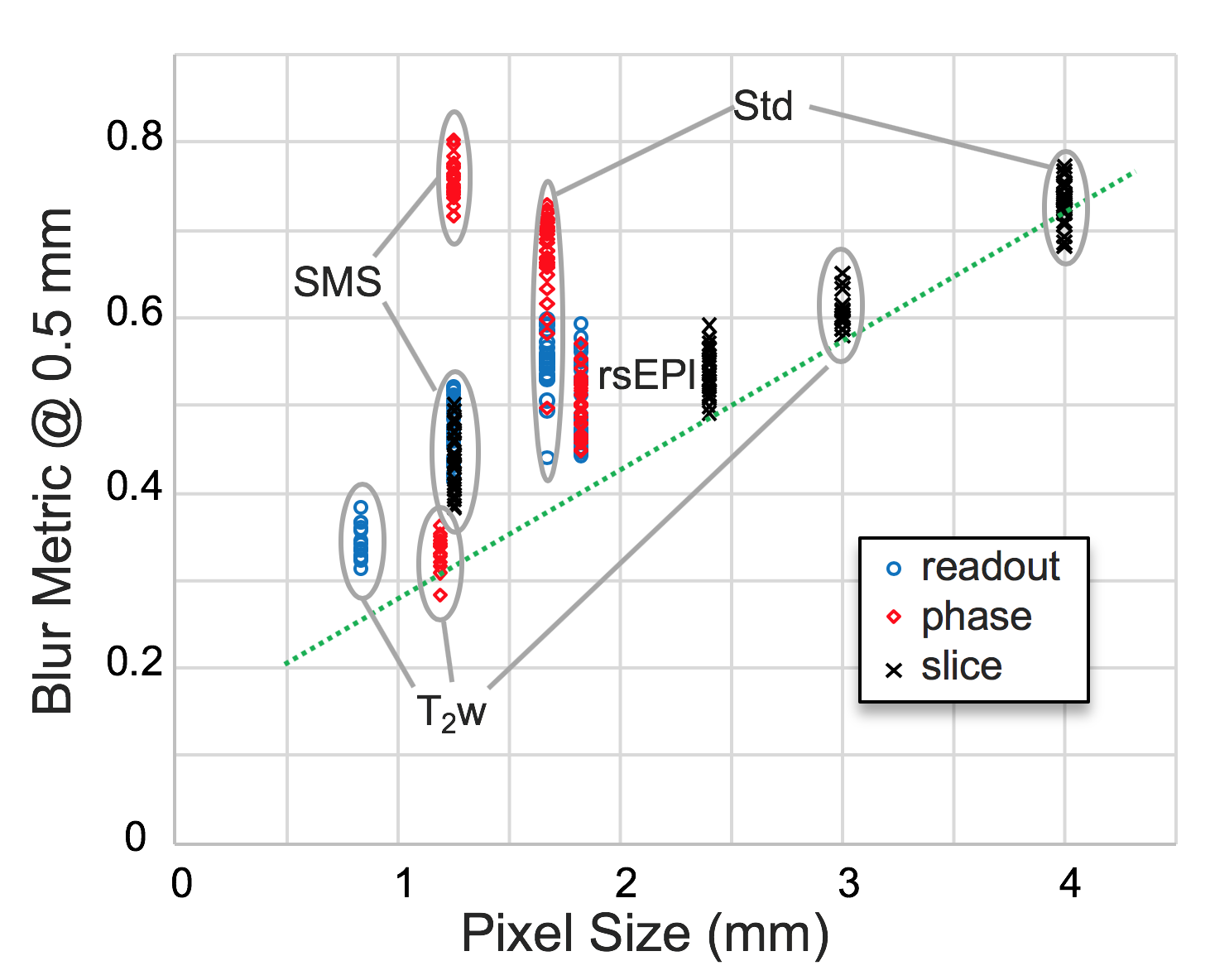
In Figure 3 the standard method shows more in-plane blurring than the readout-segmented method even though its nominal pixel size is smaller. Figure 4 explores this further by plotting the blur metric as a function of nominal pixel size in all 3 directions. There is a general trend for greater sharpness with smaller pixel sizes (green line), but this does not hold for PE in single-shot EPI.
Discussion
This technique can be used to objectively assess in vivo performance and guide sequence optimization. However, because the metric is sensitive to noise and image contrast, further work is needed to fully calibrate the blur metric as a general tool to measure true resolution. We propose that the green line in Figure 3 roughly estimates the relationship between the blur metric and the effective resolution. For example, the in-plane blurring observed in the standard DWI (1.7x1.7 mm) is comparable with a non-EPI encoded image with resolution of ~3x3 mm, which is consistent with Figure 1a where the 2 mm feature is blurry and the 1.25 mm grid is undetectable. Similarly, the T2w anatomical image comes closest to reaching the nominal in-plane resolution of 1.2x0.8 mm, and the 1 mm feature is most sharply detected in the T2w image (Figure 1d).Conclusions
While nominal resolution was found to be a poor predictor of image blurriness in single-shot EPI, the proposed use of the Crété-Roffet blur metric on resampled images appears to be a robust and objective means of comparing effective in vivo resolution. In this comparison, both high-resolution DWI methods showed improved in-plane resolution over the standard DWI technique but were inferior to the T2w image.Acknowledgements
NIH P41 EB015894
NIH R21 CA201834
NIH 1S10 OD017974-01
References
1) Partridge SC, et al. JMRI 2017;45:337–355. 2) Wilmes LJ, et al. Academic Radiology 2013;20:581–589. 3) Granlund KL, et al. Magn Reson Imaging 2014;32:330–341. 4) Bogner W, et al. Radiology 2012;263:64–76. 5) Taviani V, et al. Magn Reson Med 2017;77:209–220. 6) McKay JA, et al. Proc ISMRM. 25; 2017. p. 2115. 7) Schweitzer ME. J Magn Reson Imaging 2018;48:11–12. 8) Crete F, Dolmiere T, Ladret P, Nicolas M. In: SPIE Electronic Imaging Symposium Conf, Human Vision and Electronic Imaging 2007. 9) Partridge SC, et al. Radiology 2018. 10) High Precision Devices
Figures