4108
Diagnostic value of intravoxel incoherent motion (IVIM) in benign and malignant breast lesions1The Second Hospital of Dalian Medical University, Dalian, China, 2GE Healthcare, Beijing, China
Synopsis
In recent years, incoherent motion in voxel has been initially applied to the diagnosis and differential diagnosis of breast lesions. Traditional single-index model DWI can not completely reflect the biological characteristics of tissue diffusion. IVIM bi-exponential model and stretched-exponential model can separate the pseudo-diffusion produced by blood flow in microvessels from the real water molecular diffusion, and accurately evaluate the benign and malignant tumor. This study intends to reflect the characteristics and changes of microstructure in breast tissues at molecular level by quantitative parameters of combined lVIM bi-exponential model and stretched-exponential model, which provides an effective basis for early detection and accurate diagnosis of breast cancer
Purpose
With the change of lifestyle, the incidence of breast cancer is on the rise. Early detection and treatment are of great significance to reduce the mortality of breast cancer.Intravoxel incoherent motion (IVIM) model may reflect both the internal structure of tissues, obtaining the information of tissue diffusion and microcirculation perfusion[1] , and stretch model (SEM) may reflect the heterogeneity of tissue structure, and they have becoming a hot spot in breast cancer MRI research. The purpose of this study was to compare the value of the parameters related to IVIM bi-exponential model, stretched-exponential model and the traditional diffusion-weighted imaging (DWI) single-exponential model in the differential diagnosis of breast benign and malignant lesions.Material and Methods
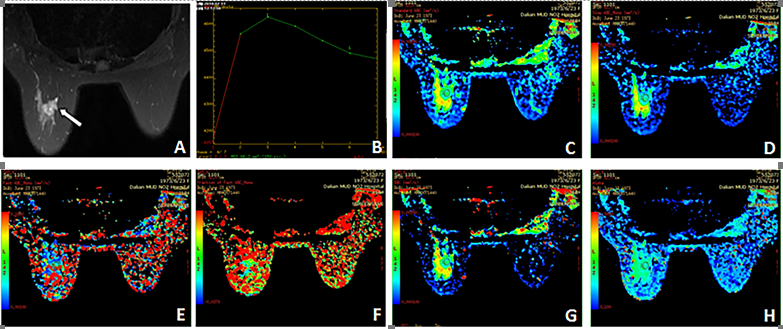
Sixty cases (62 lesions) of breast with routine MRI examination, DWI (b=0,800s/mm2) and IVIM(b=0, 10,30,50,80,100,200,400,600,800,1000s/mm2 ), before operation from October 2016 to September 2017 were enrolled. Ethical approval was obtained and constent forms were waived. All cases were confirmed by pathology, including 30 cases of malignant lesions. There were 3 cases of ductal carcinoma in situ, 26 cases of invasive ductal carcinoma, 1 case of basal cell-like carcinoma; 32 cases of benign lesions, including 25 cases of fibroadenoma, 1 case of granulomatous mastitis, 4 cases of intraductal papilloma and 2 cases of cyst. All the subjects underwent MR examinations on a 3T MR scanner (Discovery MR750W, GE Healthcare, USA). Images analyses were performed on GE AW4.6 Workstation. Area of cystic degeneration, necrosis and bleeding, and irregular ROI were used in measuring the quantitative parameters, including slow ADC mono (D), fast ADC mono (D*), Ffast mono(f) of IVIM bi-exponential model, and Diffusion index (DDC) and diffusion heterogeneity index (α) of stretched-exponential model. 1-sample K-S test and independent sample T-test were applied to investigate the statistical signicance of the results. The area under the operating characteristic curve (ROC curve) was calculated to evaluate the diagnostic effect of each parameter on benign and malignant breast lesions. The optimal threshold of each parameter and the corresponding youden index, sensitivity and specificity were calculated. Logistic regression analysis was used for the combined diagnosis of benign and malignant lesions in IVIM bi-exponential model and stretched-exponential model.
Results
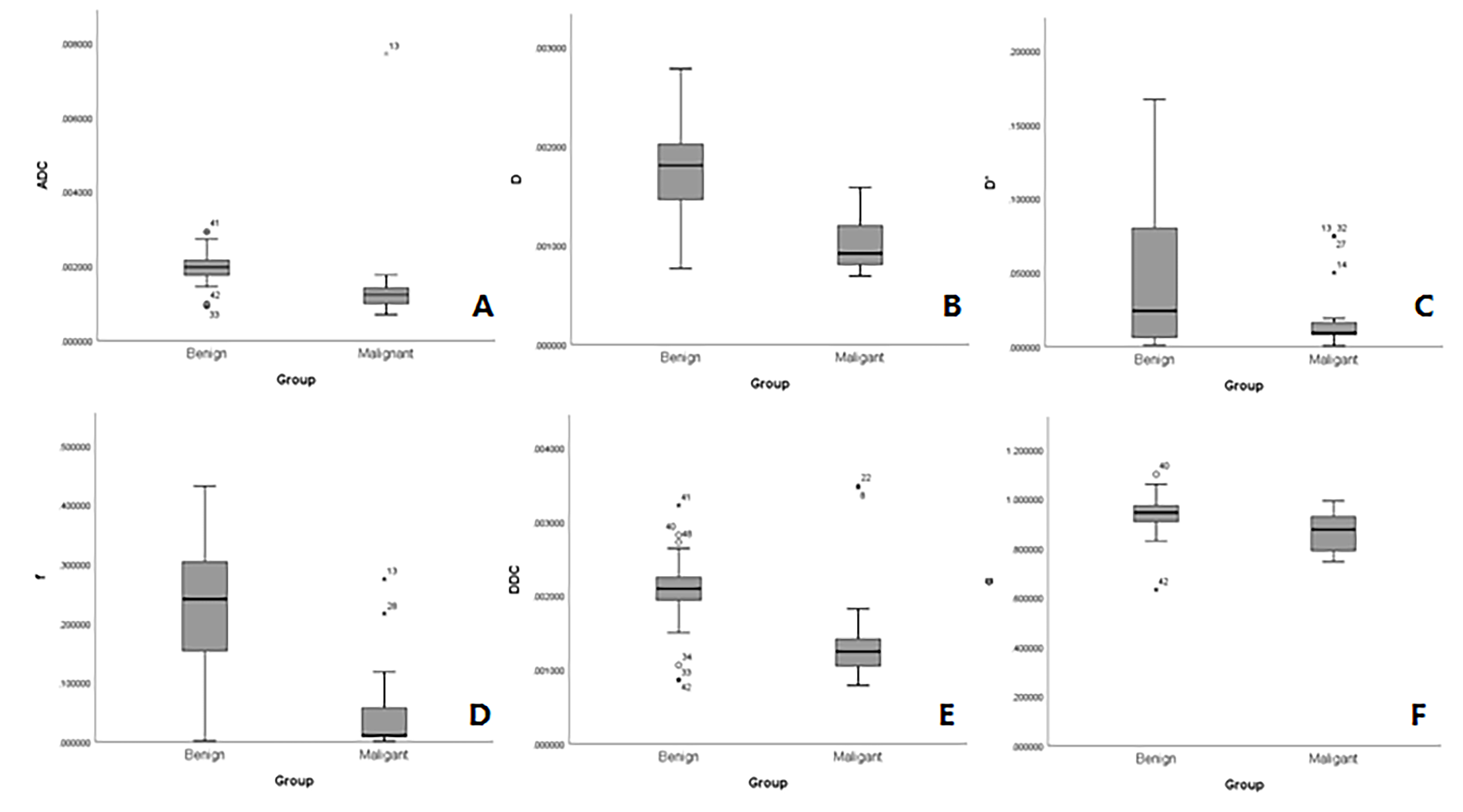
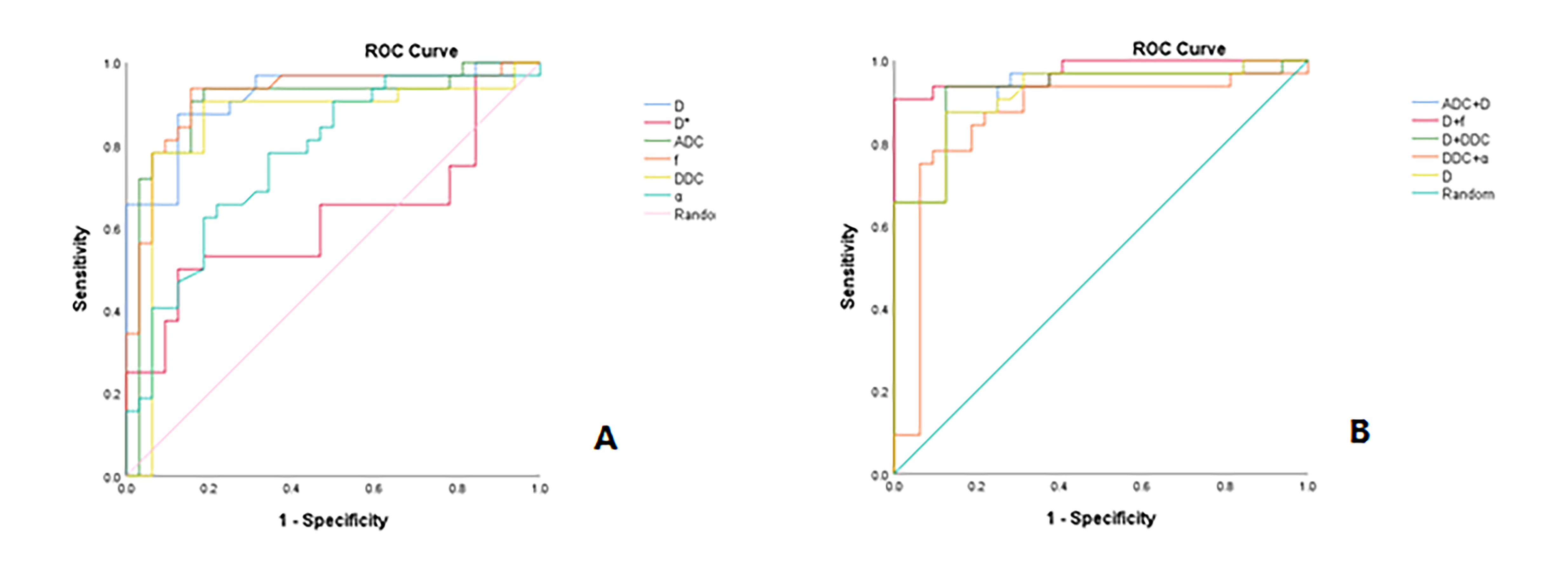
Figure 1 shows a representative case with illustration of the ROI placement. Figure 2 shows there were significant differences in ADC values from DWI and D, f, DDC, α values from IVIM between benign and malignant breast lesions. Among them, the value of ADC, D, D*, f , DDC and α was statistically significant in benign and malignant lesion. The areas under curve(AUC) of ADC,D,D*, f, DDC, and α were0.898, 0.919, 0.621, 0.918, 0.849 and 0.772 respectively, ROC curves showed that D shows the highest AUC, The ADC shows the highest sensitivity(0.938) and D shows the highest specificity (0.875) . as shown in Figure 3. In the joint diagnosis of the IVIM, the area under the ROC curve (AUC) of ADC and D, D and f, D and DDC, DDC and α was 0.922, 0.973, 0.924 and 0.861, the values of combined D and f shows the highest sensitivity and specificity (0.906 and 1).Discussion
MRI has been widely used in the diagnosis of breast diseases because. In particular, IVIM bi-exponential model, which can more accurately reflect the diffusion of water molecules and microcirculation perfusion, and stretched-exponential model, which can reflect the heterogeneity of voxels, have been investigated for differentiating benign from malignant breast tumors[2] . The results of this study show that IVIM model parameters have statistical significance between and benign and malignant breast lesions, D of IVIM bi-exponential model has the highest diagnostic ability and specificity among all these parameters, and is significantly higher than ADC value, and the specificity of combined D and f has the highest among all parameters in individual and combined diagnoses between and benign and malignant breast lesions, and is much better than that of ADC. The ADC values obtained by traditional DWI model are not only affected by the diffusion of water molecules, but also by microcirculation perfusion[3]. The IVIM model solves this problem well by separating the diffusion of water molecules and the perfusion of microcirculation in the ADC value. It can analyze the tissue diffusion imaging data more comprehensively, reveal the pathological and physiological changes of benign and malignant breast lesions more truly, and improve the efficiency of differential diagnosis.
Conclusion
IVIM derived parameters showed diagnostic advantages than DWI in differential diagnosis of breast cancer; combining D and f derived from the bi-exponential mode can provide a higher diagnostic accuracy.Acknowledgements
No acknowledgement found.References
[1] Cho GY, Moy L,et al. Evaluation of breast cancer using intravoxel incoherent motion (IVIM) histogram analysis: comparison with malignant status, histological subtype, and molecular prognostic factors .[J].European Radiology, 2016, Vol.26 (8), pp.2547-2558
[2] Chen W, Zhang J,et al. Optimization of intra-voxel incoherent motion measurement in diffusion-weighted imaging of breast cancer.[J]. J Appl Clin Med Phys. 2017 ;18(3):191-199.
[3] Zhao M, Fu K, et al. Intravoxel incoherent motion magnetic resonance imaging for breast cancer: A comparison with benign lesions and evaluation of heterogeneity in different tumor regions with prognostic factors and molecular classification. Oncol Lett. .[J]. 2018 ;16(4):5100-5112.
Figures