4105
Sparse Radial VIBRANT: High Spatiotemporal Resolution Dynamic Contrast Enhanced MRI with Compressed Sensing in Breast1Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2GE Healthcare, Waukesha, WI, United States
Synopsis
High temporal resolution dynamic contrast enhanced (DCE) MRI is a promising technique for breast cancer detection and diagnosis. We present here Sparse Radial VIBRANT, a high spatial and temporal resolution DCE-MRI method for breast imaging using golden angle radial sampling and temporal compressed sensing, and compare with a view sharing method in breast cancer patients.
Introduction
Dynamic contrast enhanced (DCE) MRI is the backbone of clinical MRI protocols for breast cancer. High temporal resolution DCE-MRI is promising for early cancer detection and diagnosis1–4. Multiple methods of achieving high temporal resolution in DCE-MRI have been reported including view sharing and compressed sensing5–7. A drawback of view sharing techniques is that higher frequency components of k-space are undersampled and shared between timepoints, which could lead to temporal blurring and reduce quality of quantitative analysis. The purpose of this study is to present a high spatial and temporal resolution DCE-MRI method for breast imaging using golden angle radial sampling and temporal compressed sensing, which we call Sparse Radial Volume Imaging for Breast Assessment (VIBRANT), and compare with a view sharing method in breast cancer patients.Methods
Sparse Radial VIBRANT Imaging:
Five patients with newly diagnosed, invasive breast cancer were scanned at 3T (Discovery 750, GE Healthcare, Waukesha, WI) with a fat-saturated, 3D, spoiled gradient echo sequence (400 spokes, 212 frequency encode steps/spoke, FOV=30-34cm2, TR/TE=4.2/2.1ms, slice thickness=1.6mm, scan time=2minutes). Continuous data acquisition began 1 minute before contrast injection and continued for 1 minute after injection (Gadavist, Bayer Healthcare Pharmaceuticals, Whippany, NJ; 0.1mmol/kg at 2 ml/s). Data was binned into 24, undersampled timepoints (16-17 spokes/frame, 5 seconds/frame). Reconstruction was performed using temporal compressed sensing with a total variation (TV) sparsifying transform8.
DISCO Imaging:
Patients receiving the prototype Sparse Radial VIBRANT technique were matched with newly-diagnosed, breast cancer patients who received our standard view sharing technique for high-temporal resolution DCE-MRI (frequency and phase encode steps = 212x212, TR/TE = 3.8/1.7 ms, FOV = 30-38 cm, slice thickness = 1.6 mm, scan time = ~70 seconds) between February and October 2017 (6). DISCO acquisition consists of a pre-contrast mask phase and 10 or 15 time frames acquired over 60 seconds beginning simultaneously with contrast injection. Patients were matched on the criteria: receive coil, in plane resolution, time/image frame within 1.1 second, patient weight within 12 kg, and tumor stage. 184 breast cancer patients were identified during this time period, 12 met these criteria and 5 were randomly selected.
Qualitative Image Assessment:
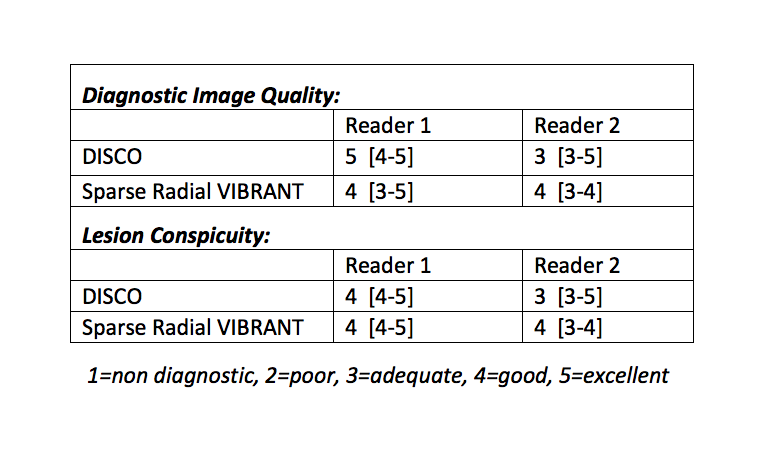
Pooled patient images were randomized and evaluated by 2, blinded radiologists (7 and 13 years experience in breast MRI) for image quality. Only images acquired during and post-contrast injection were assessed (60 seconds). Ratings were performed on a scale of 1 to 5 for lesion conspicuity and diagnostic image quality. Differences in ratings between the two image types were assessed using a paired t test.
Quantitative Image Assessment:
Tumors were volumetrically segmented on the maximum intensity projection (MIP) across timepoints for Sparse Radial VIBRANT and DISCO images. Noise within the tumor region of interest (ROI) was calculated based on repeated measures method as
$$\sigma = \frac{1}{\sqrt{2}} stddev_{r\in ROI}\left(S(r,1) - S(r,2)\right)$$
where S(r,1) is signal intensity of pixel r at timepoint 1 and S(r,2) is signal intensity of pixel r at timepoint 2, and assumed ergodic. Signal to noise ratio (SNR) and contrast to noise ratio (CNR) was calculated as
$$SNR(t) = \frac{S_{ROI}(t)}{\sigma}, \,\,\, CNR(t) = \frac{\left|S_{ROI}(t) - S_{peri}(t)\right|}{\sigma}$$
where SROI(t) is the mean signal at timepoint t within the ROI and Speri(t) is the mean signal in the surrounding pixels at timepoint t, calculated by dilating the ROI by 3 pixels.
Results
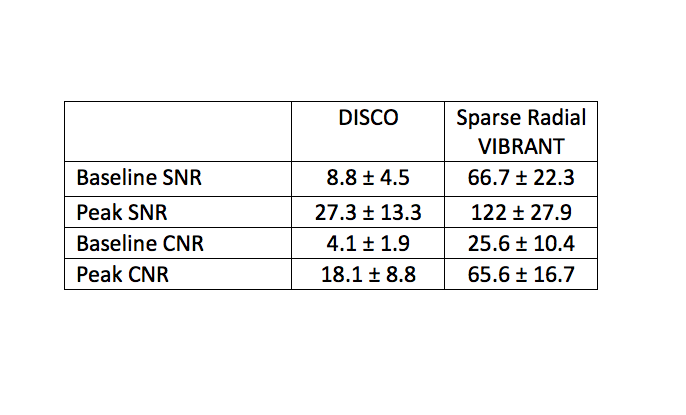
Qualitative image quality and lesion conspicuity scores were not significantly different between Sparse Radial VIBRANT and DISCO images (table 1). Both SNR(0) and peak SNR (defined here as the highest SNR across timepoints), as well as CNR(0) and peak CNR, were higher for Sparse Radial VIBRANT than for DISCO (table 2). These differences were statistically significant with p<0.05 although power is limited given sample size.Discussion
Diagnostic image quality of Sparse Radial VIBRANT is comparable to that of DISCO. SNR and CNR, however, are much higher for Sparse Radial VIBRANT than DISCO. This is likely from temporal blurring of high frequency components in DISCO images and the sparsity-promoting regularization term used for Sparse Radial VIBRANT reconstruction. The nonlinear, Sparse Radial VIBRANT reconstruction may also bias the measured noise values.
Quantitative and semi-quantitative parameters derived from DCE-MRI with DISCO have been shown to differentiate malignant from benign breast lesions1. These parameters, such as bolus arrival time, are limited by precision of view-sharing techniques. Sparse Radial VIBRANT preserves temporal fidelity for quantitative analysis and may improve their diagnostic performance. Furthermore, the radial trajectory used in VIBRANT Star is less sensitive to motion. This is advantageous for avoiding artifacts due to patient motion and increasing diagnostic capability in the axilla where cardiac motion artifacts can obscure morphology.
Acknowledgements
No acknowledgement found.References
1. Pineda FD, Medved M, Wang S, et al.: Ultrafast Bilateral DCE-MRI of the Breast with Conventional Fourier Sampling: Preliminary Evaluation of Semi-quantitative Analysis. Acad Radiol 2016; 23:1137–1144.
2. Abe H, Mori N, Tsuchiya K, et al.: Kinetic Analysis of Benign and Malignant Breast Lesions With Ultrafast Dynamic Contrast-Enhanced MRI: Comparison With Standard Kinetic Assessment. AJR Am J Roentgenol 2016; 207:1159–1166.
3. Mus RD, Borelli C, Bult P, et al.: Time to enhancement derived from ultrafast breast MRI as a novel parameter to discriminate benign from malignant breast lesions. Eur J Radiol 2017; 89:90–96.
4. Platel B, Mus R, Welte T, Karssemeijer N, Mann R: Automated characterization of breast lesions imaged with an ultrafast DCE-MR protocol. IEEE Trans Med Imaging 2014; 33:225–232.
5. Mann, Mus, Geppert, Barentsz, Huisman: Ultrafast dynamic imaging of the breast at diagnostic spatial resolution using TWIST. .
6. Saranathan M, Rettmann DW, Hargreaves BA, Lipson JA, Daniel BL: Variable spatiotemporal resolution three-dimensional Dixon sequence for rapid dynamic contrast-enhanced breast MRI. J Magn Reson Imaging 2014; 40:1392–1399.
7. Heacock L, Gao Y, Heller SL, et al.: Comparison of conventional DCE-MRI and a novel golden-angle radial multicoil compressed sensing method for the evaluation of breast lesion conspicuity. J Magn Reson Imaging 2017; 45:1746–1752.
8. Feng L, Grimm R, Block KT, et al.: Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014; 72:707–717.
Figures