4104
Quantitative assessment of changes in breast background parenchymal enhancement following tamoxifen treatment1Radiology, The University of Chicago, Chicago, IL, United States, 2Radiology, Shiga University of Medical Science, Otsu, Japan
Synopsis
Our study introduces a standardizing model of background parenchymal enhancement (BPE) in DCEMRI sequences that can be used to quantitatively and objectively describe changes in BPE rates following preventative tamoxifen treatment. This is in contrast with the current practice of using 4 subjective categories to describe BPE. Decreased BPE rates post-treatment agree with earlier results showing that BPE, like breast density, correlates with breast cancer risk. Standardization for imaging parameters and contrast agent relaxivity increases the observed effect size, giving evidence of increased sensitivity to treatment-induced changes and the potential as a tool for individual breast cancer risk management.
Purpose
To introduce a method to standardize quantification of breast background parenchymal enhancement (BPE) on DCEMRI using a linear approximation to the early signal change and a correction for differences in acquisition parameters and contrast agent relaxivity.
Introduction
Earlier literature established a correlation between BPE and breast cancer risk, similar to the correlation between breast density and breast cancer risk. (1-3) Other studies showed that BPE is reduced after tamoxifen or aromatase inhibitor therapy and could therefore serve as a marker of preventative treatment response. (4-6) However, earlier studies categorized BPE into 4 categorical groups by visual observation, limiting sensitivity to changes. We demonstrate a quantitative analysis of BPE prior to and following tamoxifen treatment with increased sensitivity to small changes.Methods
On a retrospective database search, 21 patients (ages 27-63, median 46 years) were identified who have undergone two MRI exams, prior to and following tamoxifen treatment, with at least one uninvolved breast. Seven patients were excluded for technical reasons. Dynamic contrast-enhanced MRI (DCEMRI) was performed for all exams, with time resolution of 55-78 s and following the contrast uptake and washout for 4-11 minutes (TR = 4.4-7.9 ms, TE = 2.1-4.2 ms, flip angle = 10-30°).
A mask of breast tissue was created from the first DCEMRI acquisition, and then eroded in two orientations to exclude the skin. Pre-contrast images, multiplied by the eroded mask, were projected in the axial and sagittal planes. The central breast region of interest was drawn manually in two projections, excluding skin and nipple tissue, chest wall muscle, and axillae. Breast where lesions were present were excluded. In the remaining central breast tissue, supervised fuzzy C-means algorithm was used to segment breast parenchyma.
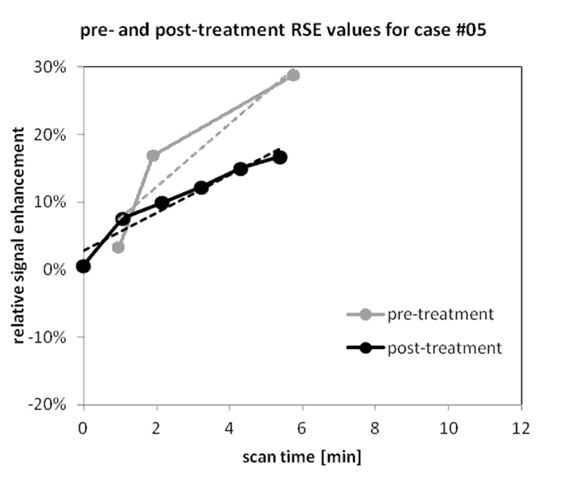
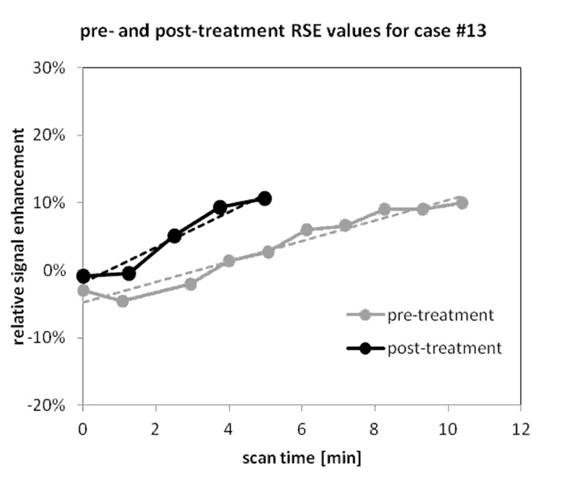
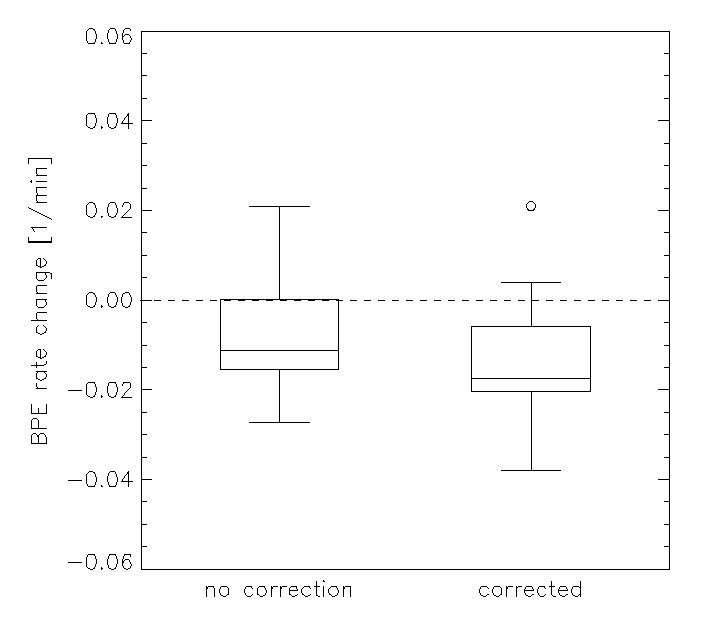
Relative signal enhancement (RSE, relative to the unenhanced signal) averaged over the parenchymal volume was calculated for pre- and post-treatment DCEMRI scans, on a time scale relative to the first post-contrast acquisition. The MR signal was scaled using the gradient echo signal equation to correct for differing TR and/or flip angle values in order to allow direct comparison. For this purpose, baseline values of parenchymal T1 = 1250 ms (1.5T) and 1450 ms (3T) were used. The post-contrast RSE uptake curves were modeled as a linear function whose slope indicated the RSE rate, with higher slopes indicating faster BPE. The RSE rates were then compared between pre- and post-treatment scans, and the characteristics of the group with decreased vs that showing increased BPE rate were compared. The effect size for post-treatment change in BPE rates was calculated for DCEMRI data without and with correction for imaging parameters and contrast agent relaxivity and compared.
Results
The range of tamoxifen treatment duration was 8 to 36 months. A larger proportion of subjects showed decreased BPE (n=11) than increased BPE (n=3) (p < 0.03, one-sided Wilcoxon signed rank test). The average values in the group with decreased vs the group with increased BPE rate were (two-sided Mann–Whitney U test): treatment duration 29.1 ± 15 vs 20 ± 7 months (p > 0.05); pre-treatment BPE rate 0.53 ± 0.025 1/min vs 0.025 ± 0.020 1/min (p < 0.05); post-treatment BPE rate 0.034 ± 0.022 1/min vs 0.034 ± 0.016 1/min (p > 0.05). The change in BPE rate pre- and post-treatment (0.047 ± 0.026 1/min vs 0.034 ± 0.020 1/min, p < 0.03, one-sided Wilcoxon signed rank test) was not significantly correlated with treatment duration (Pearson correlation coefficient). The effect sizes for post-treatment BPE rate changes were 0.62 in non-corrected vs 0.86 in corrected data.Discussion and Conclusion
Our study introduces a standardizing model of BPE in DCEMRI sequence that can be used to quantitatively describe changes in BPE rates following preventative tamoxifen treatment. The demonstrated decreased BPE rates post-treatment agree with earlier results showing that BPE, like breast density, correlates with breast cancer risk. The improvement in the effect size following standardization of the DCEMRI signal supports the utility of the proposed model in quantifying BPE rates. The quantitative, as opposed to subjective categorical, characterization of BPE may potentially provide a sensitive and objective measure of preventative therapy response and could become a practical tool for personalized risk management. In addition, increased sensitivity could help increase the power of large cohort studies.Acknowledgements
No acknowledgement found.References
1. King V, Brooks JD, Bernstein JL, Reiner AS, Pike MC, Morris EA. Background parenchymal enhancement at breast MR imaging and breast cancer risk. Radiology. 2011;260(1):50-60.
2. Bennani-Baiti B, Dietzel M, Baltzer PA. MRI Background Parenchymal Enhancement Is Not Associated with Breast Cancer. PloS one. 2016;11(7):e0158573.
3. Telegrafo M, Rella L, Stabile Ianora AA, Angelelli G, Moschetta M. Breast MRI background parenchymal enhancement (BPE) correlates with the risk of breast cancer. Magnetic resonance imaging. 2016;34(2):173-176.
4. Pike MC, Pearce CL. Mammographic density, MRI background parenchymal enhancement and breast cancer risk. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. 2013;24 Suppl 8:viii37-viii41.
5. King V, Kaplan J, Pike MC, et al. Impact of tamoxifen on amount of fibroglandular tissue, background parenchymal enhancement, and cysts on breast magnetic resonance imaging. The breast journal. 2012;18(6):527-534.
6. King V, Goldfarb SB, Brooks JD, et al. Effect of aromatase inhibitors on background parenchymal enhancement and amount of fibroglandular tissue at breast MR imaging. Radiology. 2012;264(3):670-678.
Figures