4102
UTE-SENCEFUL with a coil clustering algorithm for automatic DC gating1Department of Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany
Synopsis
In this work UTE-SENCEFUL is combined with a technique for automatic DC gating to produce ventilation weighted maps of the lung in 3D and in high-resolution.
Introduction
Self-gated Non-Contrast-enhanced Functional Lung MRI (SENCEFUL1) has been recently combined with a UTE technique to determine 3D high-resolution ventilation maps of the lung (UTE-SENCEFUL2). This technique exploits the DC signal variations in the k-space center as a navigator, to assess functional information in free-breathing and without employment of contrast agent. In the original implementation, a single coil element of which the DC-signal shows high correlation with breathing motion must be selected manually. Such approach, however, is time consuming and restricts UTE-SENCEFUL’s application in clinical routine. Aiming to improve its robustness and usability, this work implements an automatic method for DC-gating3 using a coil clustering algorithm in the UTE-SENCEFUL framework.Methods
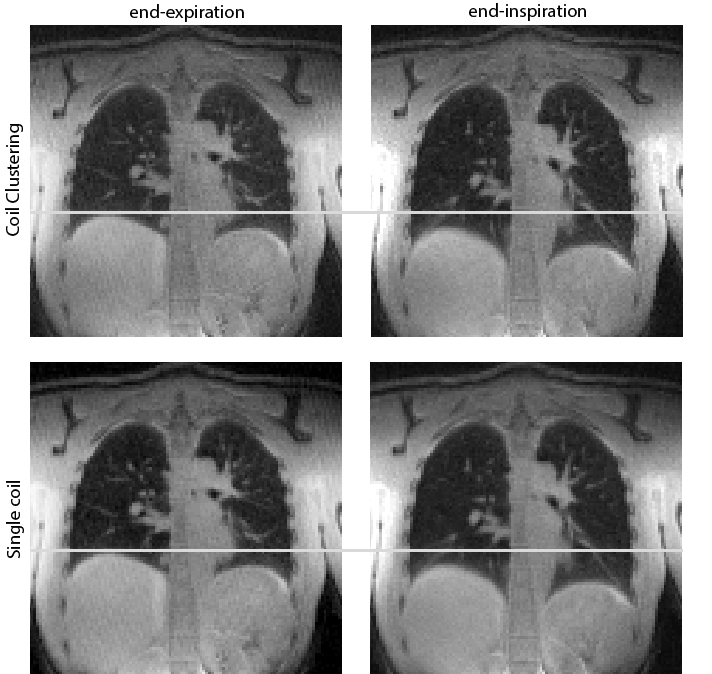
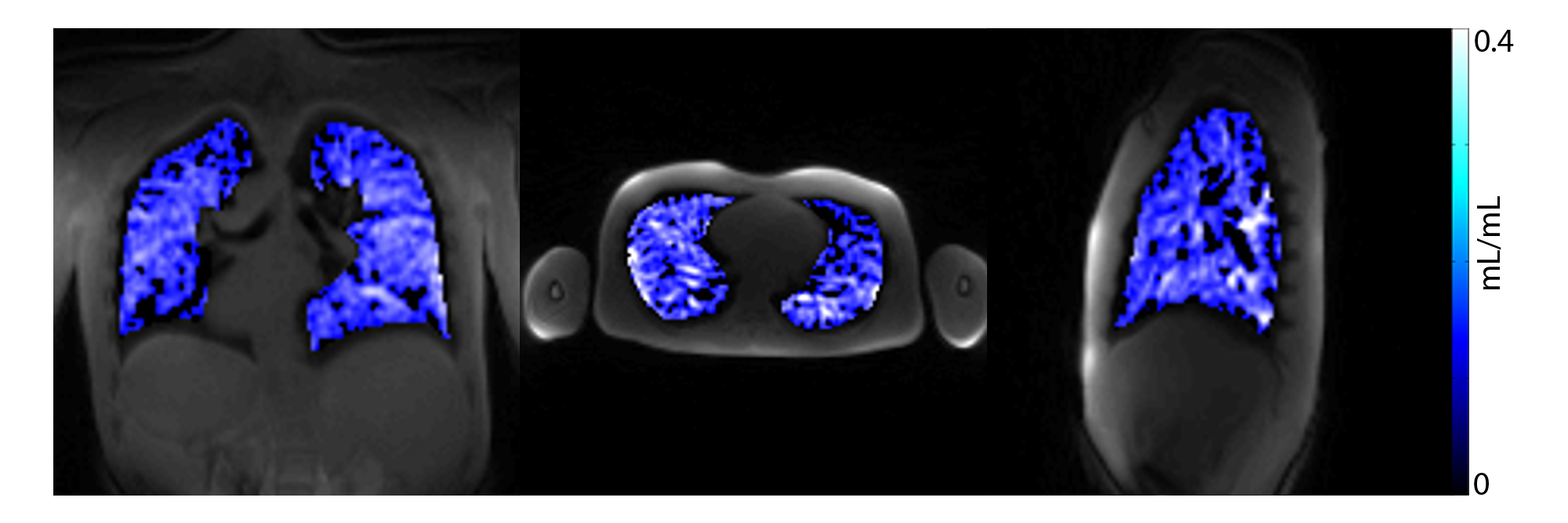
Three healthy volunteers were investigated in this study. The measurements were performed during tidal breathing and supine position on a 3T MR scanner (Magnetom Prisma, Siemens Healthineers, Erlangen) equipped with a 32-channel coil array. The following sequence parameters were used: TE = 0.03 ms; TR = 1.49ms; flip angle = 2°; FOV = 350x350mm; number of projections = 350000, resolution = 2.7mm x 2.7mm, slice thickness = 2mm. The UTE sequence consisted of a non-selective RF pulse with a radial center-out acquisition2,4. The DC signal from each coil was extracted from the first 5 measured points after the transient phase of the digital filter and before the gradient was ramped up. The DC signal was filtered using a Savitzky-Golay function and a correlation matrix of all coils was calculated. A thresholding operation was applied to the correlation matrix, and all values above 0.95 were set to 1. Values smaller than the threshold were set to zero. As presented elsewhere 3, principal component analysis was applied to calculate the eigenvalue decomposition of this matrix. The coil cluster was selected based on the eigenvalues corresponding to eigenvectors higher than 0.1. The motion estimate was then calculated as the average DC signal within the coil cluster. This signal was used as navigator to segment the acquired data in 8 different breathing phases. Each breathing phase had a sampling density of at least 25% of the Nyquist sampling rate. Trajectory errors were corrected using the Gradient Impulse Response Function of the utilized gradient system 5. Iterative SENSE was applied to reconstruct the data set of each breathing phase6. For comparison, time resolved images were also reconstructed using the DC signal from a single coil, which was manually chosen2. The maximum of the first derivative in the lung-liver interface was used to calculate the distance in pixels, from the diaphragm in the end-inspiration and end-expiration phases. This distance was used as a quantitative parameter to compare the manual and automatic methods for DC gating and coil selection. Finally, ventilation weighted maps were generated from the time series1,2. For that purpose, breathing motion was eliminated using a 3D image registration technique7.Results
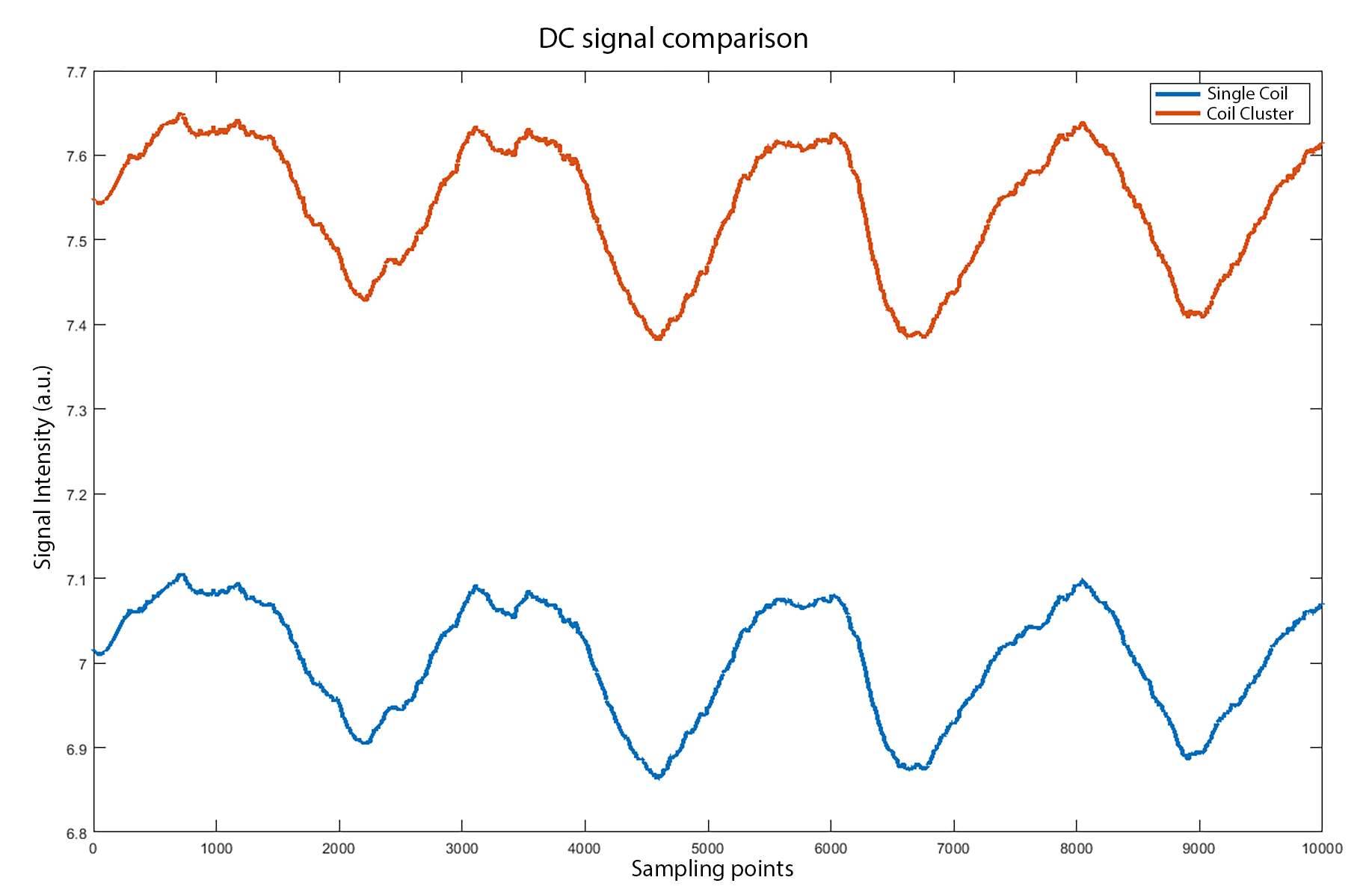
On average, the distance between the lung-liver interface in the end-inspiration and end-expiration phases was 7% larger in images reconstructed using the coil-clustering method. Nevertheless, as presented in Fig 1, the sharpness of both gating techniques was visually similar. In Figure 2 a comparison between the DC-signal from the two methods is depicted. No major differences were apparent. An example of a functional map is presented in Figure 3. No ventilation impairment or defects were found in the ventilation weighted maps of the healthy subjects.Discussion
UTE-based SENCEFUL MRI is a robust technique for the assessment of both the morphological and functional information of the lung with short scan-times. The findings of this work have revealed that coil clustering results in similar quality compared to a manual selection of the DC signal. The integration of automatic DC gating thus helps paving the way towards UTE-SENCEFUL's use in the clinical routine.Acknowledgements
No acknowledgement found.References
1. Fischer A, Weick S, Ritter CO, et al. SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) using a quasi-random fast low-angle shot (FLASH) sequence and proton MRI. NMR Biomed. 2014.
2. Mendes Pereira, L; Wech T, Weng A. UTE‐SENCEFUL: first results for 3D high‐resolution lung ventilation imaging. Magn Reson Med. 2018.
3. Zhang T, Cheng JY, Chen Y, Nishimura DG, Pauly JM, Vasanawala SS. Robust self‐navigated body MRI using dense coil arrays. Magn Reson Med. 2016.
4. Weick S, Ehses P, Blaimer M, Breuer FA, Jakob PM. Improved Retrospective Self-Gated Human Lung Imaging using a Quasi Random Sampling Scheme. In: Proceedings of the 19th Annual Meeting ISMRM. ; 2011.
5. Stich M, Wech T, Slawig A, et al. Gradient waveform pre-emphasis based on the gradient system transfer function. Magn Reson Med. February 2018.
6. Pruessmann KP, Weiger M, Börnert P, Boesiger P. Advances in sensitivity encoding with arbitrary k-space trajectories. Magn Reson Med. 2001.
7. Kroon D-J, Slump CH. MRI modalitiy transformation in demon registration. In: 2009 IEEE International Symposium on Biomedical Imaging: From Nano to Macro. IEEE; 2009:963-966.
Figures