4093
Assessment of scan parameter effects on time resolved bSSFP acquisition for Fourier Decomposition Pulmonary MR1Computer Assisted Clinical Medicine, Heidelberg University, Mannheim, Germany
Synopsis
Pulmonary functions play an important role in diagnosis of pulmonary diseases. One method for functional lung MRI is Fourier Decomposition technique, which obtains ventilation and perfusion weighted images from dynamic free-breathing acquisitions. Although this method is validated against well-established methods, its robustness depends on scan parameters and temporal resolution. In this work, we have investigated the effects of common scan parameters on image quality. In vivo results are presented to demonstrate the performance differences in protocols.
Introduction
Assessment of pulmonary functions plays an important role in the diagnosis and follow-up of lung diseases. Although methods using radioactive nuclides remain the gold standard for functional lung imaging, MRI based methods are highly desirable. One of the non-invasive methods introduced for functional lung MRI method is Fourier Decomposition technique1. The Fourier Decomposition technique relies on fast time-resolved acquisitions of chest images to obtain ventilation and perfusion weighted images. It works without contrast enhancement and is applied during free-breathing. The acquired time series data are registered to compensate for motion, and are followed by an analysis using Fourier transform to estimate respiratory and cardiac signal modulations. Although this approach is validated against well-established methods, its robustness depends on temporal and spatial resolution2. For patients with high heart rates or pediatric patients3,4,5 and patients with arrhythmia6, the temporal resolution poses another challenge due to the increased cardiac frequencies and beat-to-beat variations. In this work, we have utilized four different protocols to investigate the effects of common scan parameters on image quality of Fourier Decomposition method.Methods
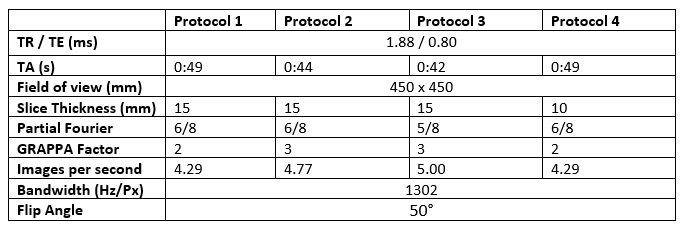
In vivo acquisitions of a healthy volunteer (female, 29 years old) during free-breathing were acquired with a 1.5 T scanner (Magnetom Avanto, Siemens Healthineers, Erlangen, Germany) using a 2D balanced steady-state free precession sequence with the scan parameters listed in Table 1. A total of 210 images were acquired for each protocol with a 0.1 s pause after each measurement. Asymmetric echo was allowed to increase signal from lung parenchyma1. The acquisitions were registered before further analyzes using a stand-alone non-rigid registration software7.
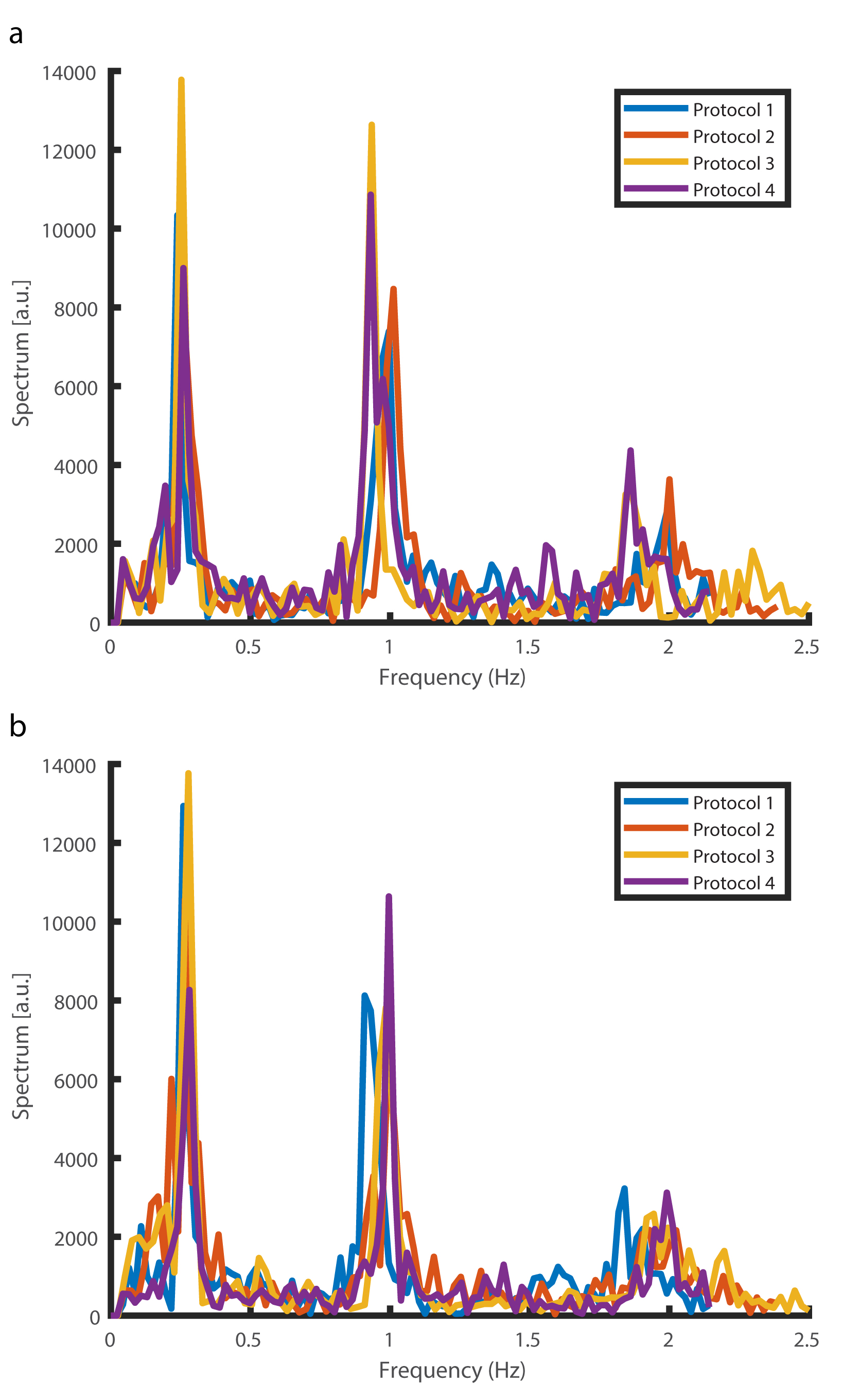
The registered datasets were analyzed voxel-wise using MATLAB (MathWorks, Natick, Massachusetts, USA). For all acquisitions, first nine images were removed to ensure steady state has been reached2. To obtain signal variations corresponding to respiratory and cardiac signal modulations, the power spectrums were estimated from the Fourier transform of the time courses. Frequencies lower and higher than 0.8 Hz were associated with respiratory and cardiac signal respectively.
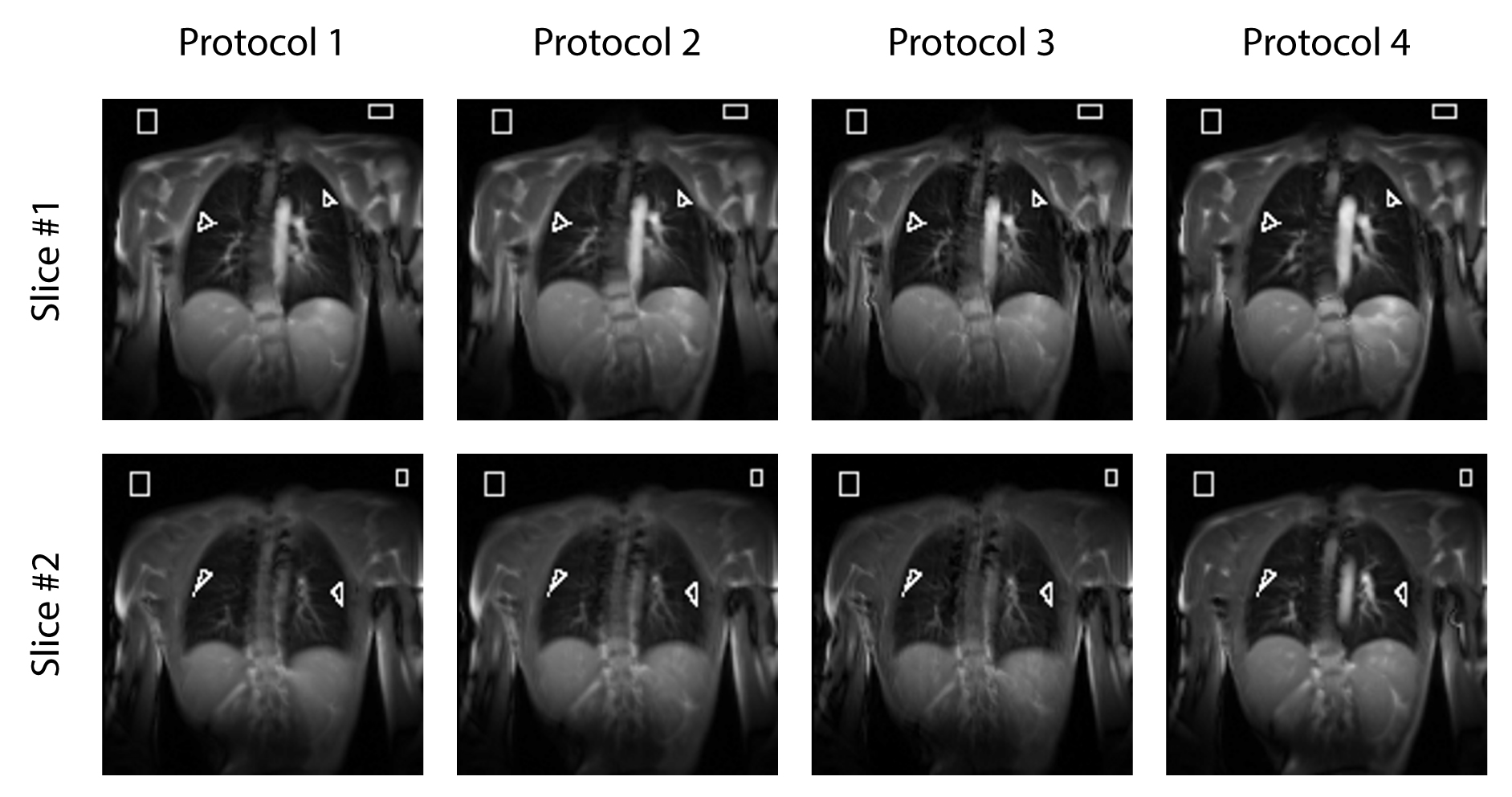
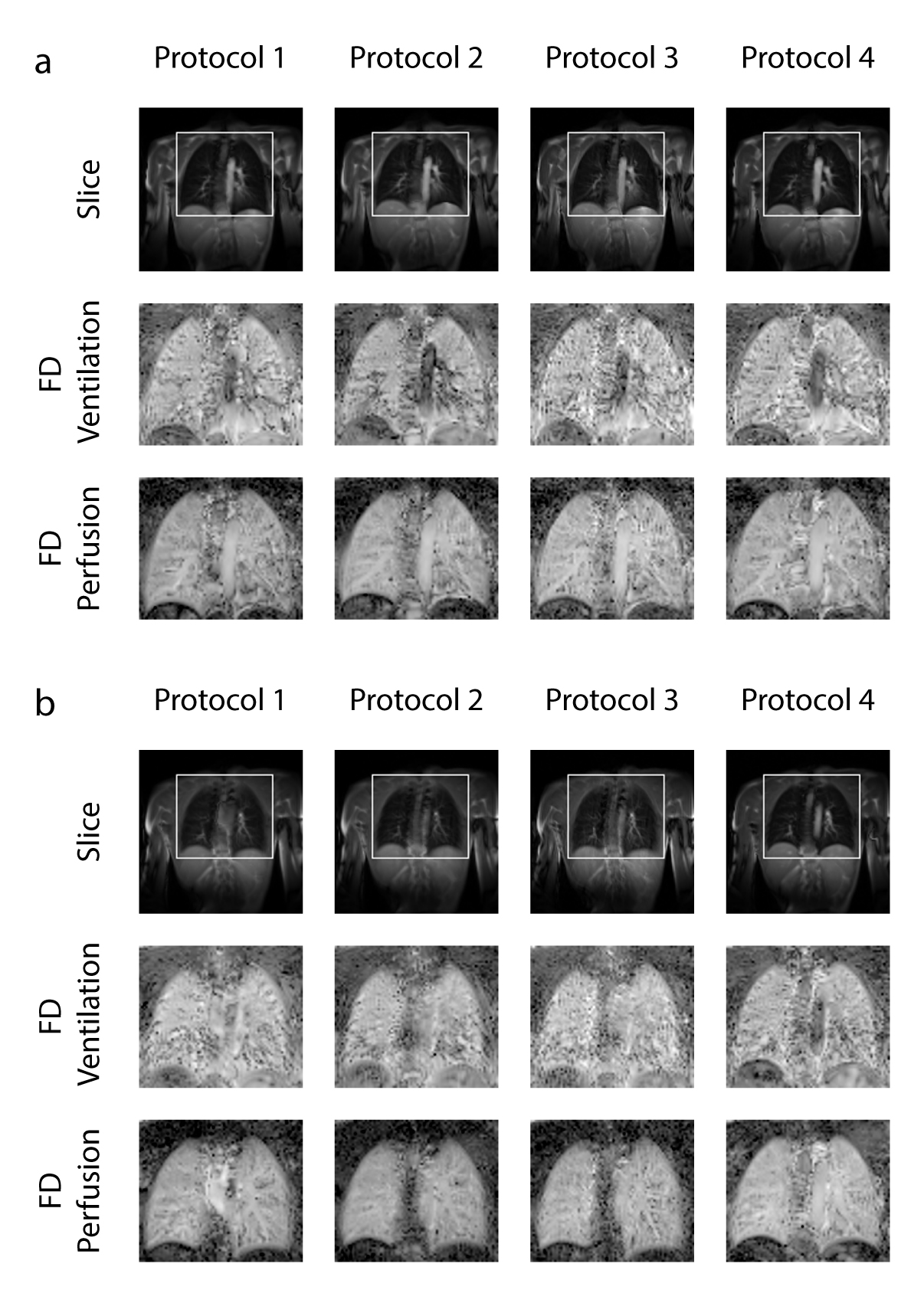
To compare the protocols, signal-to-noise ratio (SNR) values were obtained for two slices from manually drawn regions-of-interests (ROI)8 and the ROIs were extended to 201 images. For better visualization, ventilation and perfusion weighted images were generated from a reduced field of view corresponding to lung parenchyma.
Results
Figure 1 shows the power spectrums of respective protocols for both slices. As observed, all protocols successfully distinguished the peak frequencies corresponding to respiratory and cardiac frequencies. Note the higher achievable frequency for Protocols 2 and 3 compared to Protocols 1 and 4, which might be required for pediatric imaging or patients with arrhythmia3,4,6. In Figure 2, representative slices from the protocols are shown. The ROIs used for the calculation of SNR are also shown with white lines overlaid on the images. In Figure 3, the representative slices from all protocols are shown with the field of view used for the visualization, followed by ventilation and perfusion weighted images. Compared to Protocol 1 and Protocol 2, Protocol 3 and Protocol 3 generates less smooth ventilation and perfusion maps, as expected from decrease in SNR.
In Table 2, the mean SNR values corresponding to both slices are listed. As expected, with shorter acquisition time or slice thickness, the SNR decreases. Overall, our results indicate that the SNR loss between Protocol 1 and Protocol 2 is negligible and can be traded for the increased frame rate to improve the robustness of Fourier Decomposition method, especially in patients with high heart rate or younger patients3.4,5. However, shortening the acquisition time further or assigning thinner slices was observed to decrease the SNR values more than 10%.
Discussion and Conclusion
In this work, we have investigated the effects of common protocol parameters to demonstrate their effects on Fourier Decomposition based functional lung imaging. Our results indicate that the SNR penalty associated with parallel imaging factor is negligible; however, increasing the partial Fourier factor or decreasing slice thickness warrants a more careful consideration.Acknowledgements
This work was supported by Deutsche Forschungsgemeinschaft (grant number: DFG 397806429).References
1. Bauman, G. , Puderbach, M. , Deimling, M. et al. Non‐contrast‐enhanced perfusion and ventilation assessment of the human lung by means of Fourier decomposition in proton MRI. Magn. Reson. Med. 2009;62:656-664.
2. Kjørstad A, Corteville DM, Henzler T, et al. Quantitative lung ventilation using Fourier decomposition MRI: comparison and initial study. MAGMA 2014;27(6):467–476.
3. Weidner M, Zöllner FG, Hagelstein C,, et al. High temporal versus high spatial resolution in MR quantitative pulmonary perfusion imaging of 2-year old children after congenital diaphragmatic hernia repair. Eur Radiol. 2014;24(10):2427
4. Weis M, Zoellner FG, Hagelstein C, et al. Lung Perfusion MRI After Congenital Diaphragmatic Hernia Repair in 2-Year-Old Children With and Without Extracorporeal Membrane Oxygenation Therapy. American Journal of Roentgenology. 2016;206(6):1315-1320
5. Fleming S, Thompson M, Stevens R et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet. 2011; 377:1011–1018.
6. Chava R, Assis F, Herzka D, et al. Segmented radial cardiac MRI during arrhythmia using retrospective electrocardiogram and respiratory gating. Magn Reson Med. 2018;00:1–13
7. Chefd’hotel C, Hermosillo G, Faugeras O. Flows of diffeomorphisms for multimodal image registration. Proceedings IEEE International Symposium on Biomedical Imaging. 2002;753–756.
8. Corteville DMR, Kjørstad Å, Henzler T, et al. Fourier decomposition pulmonary MRI using a variable flip angle balanced steady‐state free precession technique. Magn Reson Med. 2015;73:1999–2004.
Figures