4090
Free breathing lung T1 mapping in idiopathic pulmonary fibrosis1Academic Radiology, University of Sheffield, Sheffield, United Kingdom
Synopsis
A method for free breathing Look-Locker T1 mapping using image registration is presented. This method uses a fitted model inversion recovery signal modulated with respiratory motion to create a set of synthetic images, to which all acquired free-breathing Look-Locker images are registered. The method was implemented in 9 patients with idiopathic pulmonary fibrosis (IPF) and 9 healthy volunteers and the results compared to T1 maps acquired with the same Look-Locker sequence acquired in an inspiratory breathold state for patients with IPF, and inspiratory and expiratory breath hold states for healthy volunteers. Patients with IPF were found to have a lower T1 during free breathing and a higher standard deviation of regional T1 values in the lung when compared to volunteers.
Background
IPF is a chronic lung condition where lung scarring (fibrosis) occurs in regions of the lung resulting in worsened oxygen exchange, decreased lung volume. Changes in both regional and global lung T1 have been visualised using MRI, and may offer a radiation-free method of assessing lung scarring [1][2]. However, it is often difficult for patients with IPF to maintain breath holds during imaging.Purpose
To develop methods for free breathing Look-Locker T1 mapping in the lung in healthy volunteers and patients with IPF using post-processing image registration, and compare to T1 mapping acquired at breath hold.Methods
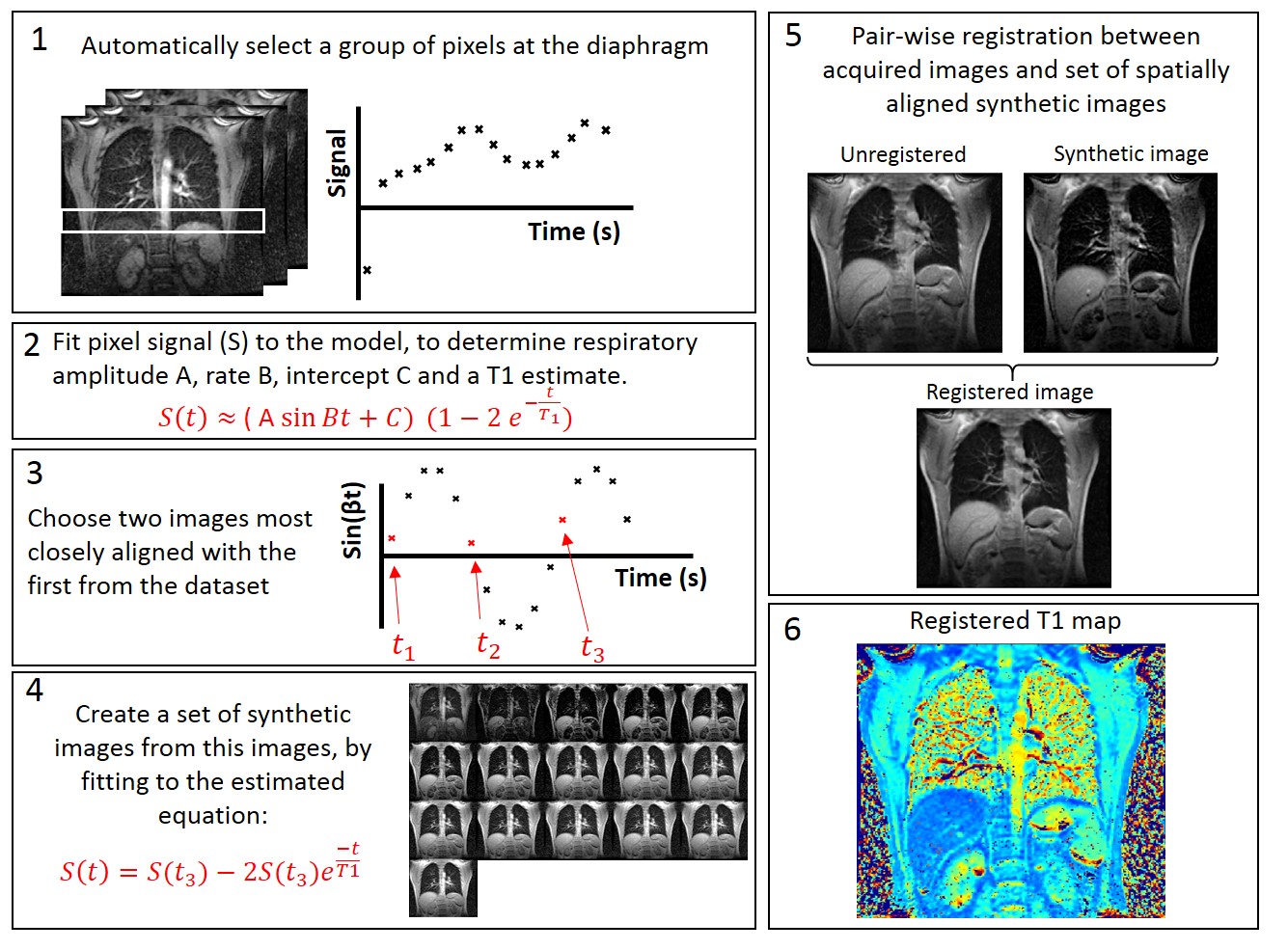
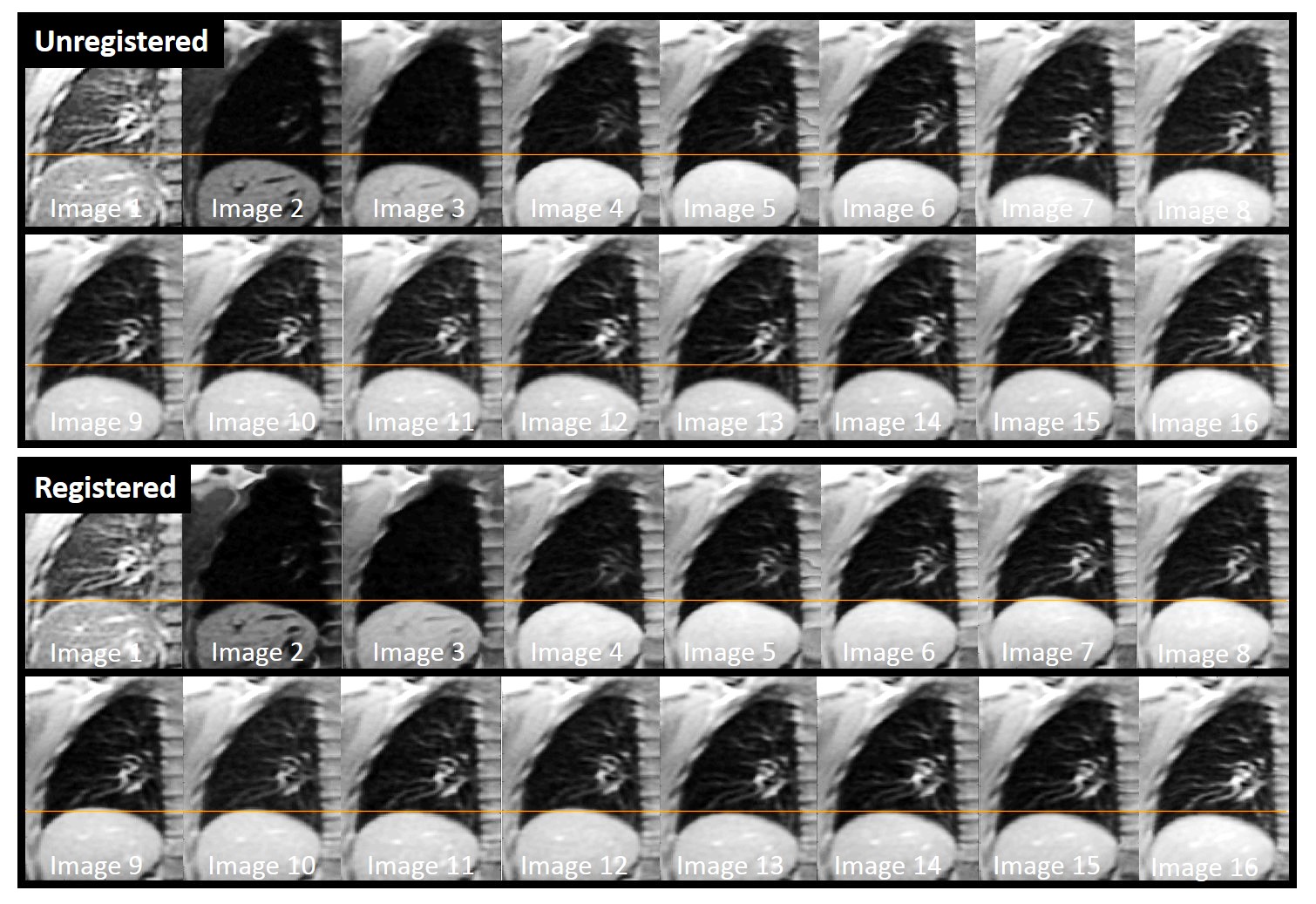
Free breathing images were registered to a set of spatially aligned synthetic images with similar contrast to the acquired images. Synthetic images are created using a combined inversion recovery and respiratory model. The model using information from the acquired images to determine respiratory rate and choose images from the same respiratory state from which to create a set of spatially aligned synthetic images, see Figure 1. All acquired images are registered to a corresponding synthetic image. Image registration efficacy was evaluated using Dice Similarity Coefficient.
9 patients with IPF (age 71±7 years, 10% female) and 9 healthy volunteers (age 30±5 years, 30% female) underwent 1.5T lung MRI using a 2D Look- Locker inversion recovery sequence during both inspiration breath hold and free breathing. 7 of the volunteers also underwent the same sequence during expiration. The Look-Locker sequences comprised a 180° inversion pulse followed by 16 gradient echo images. Look-Locker imaging parameters were as follows: Inversion time, TI: 229ms; TR=3.2ms; α=7°; phase x frequency: 128 x 128; slice thickness: 15mm. Breathing instructions for free breathing acquisition were to breath normally.
Results
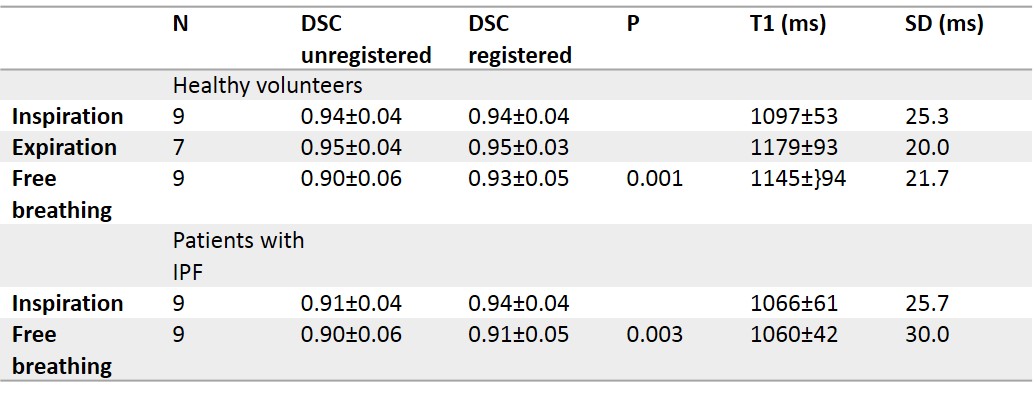
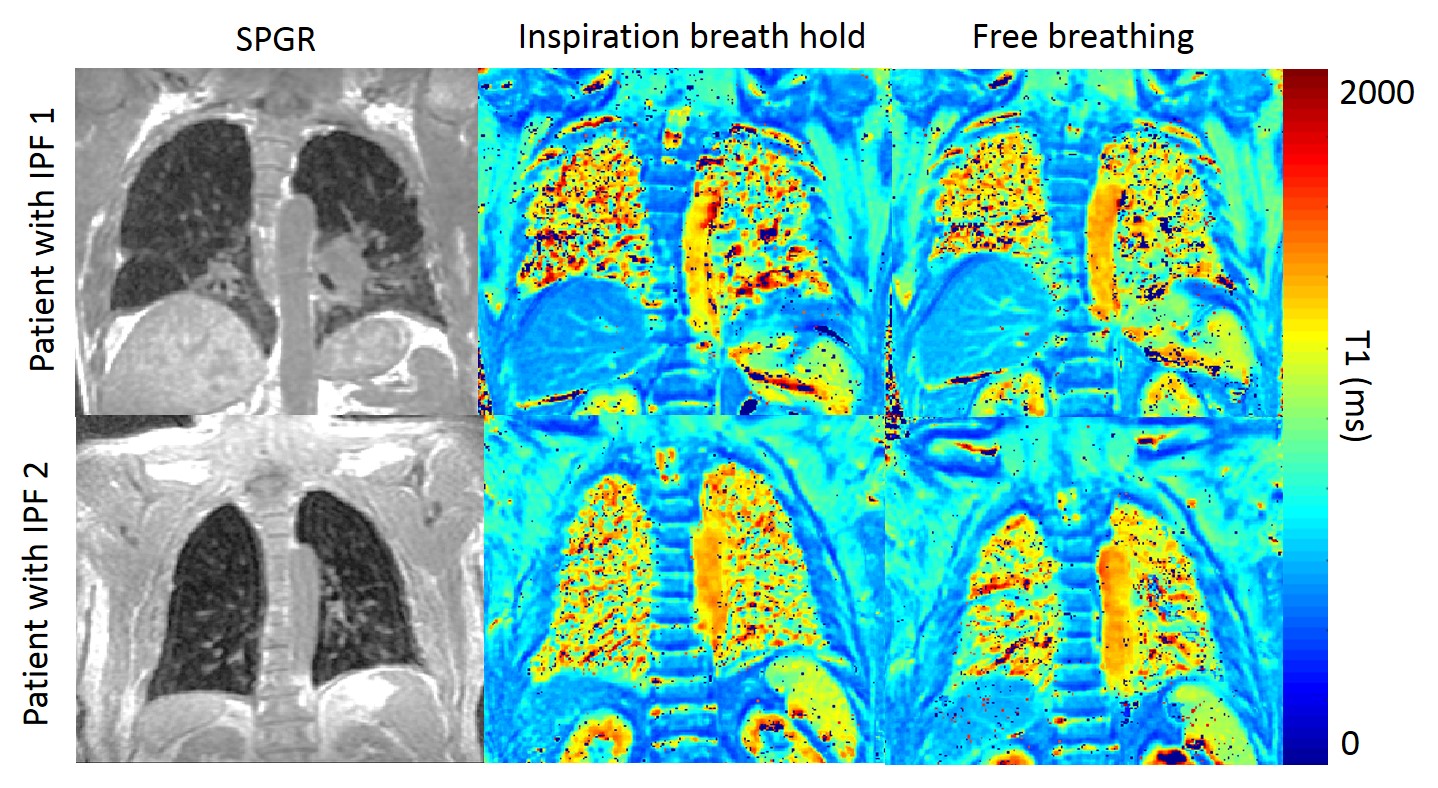
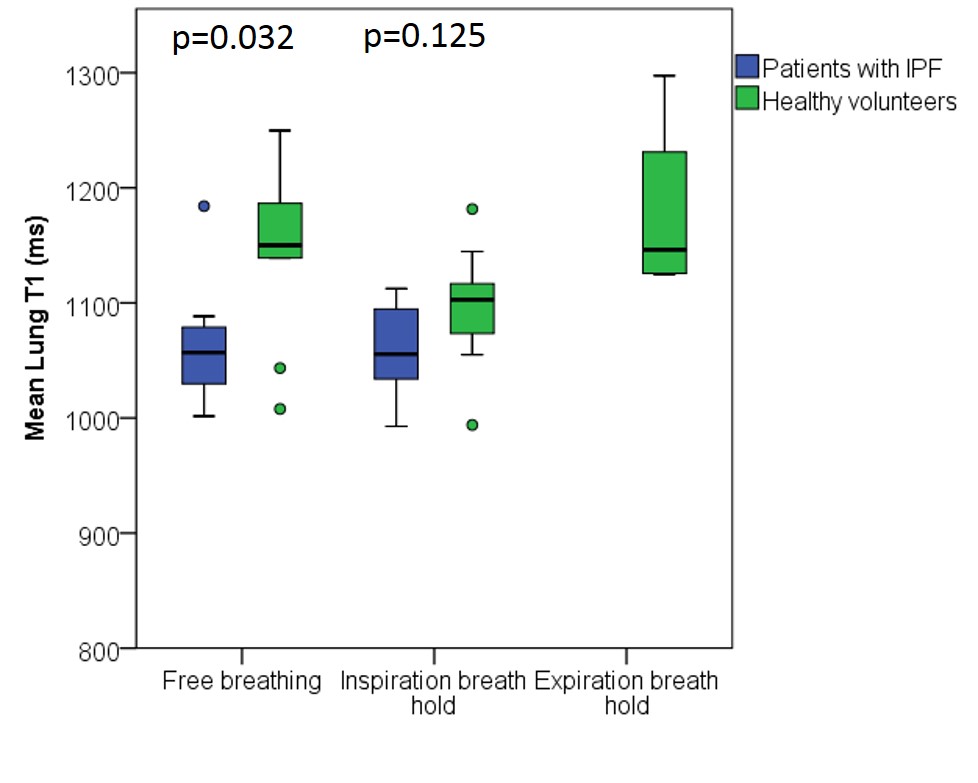
Image registration significantly increased overall DSC in free breathing inversion recovery image datasets (p<0.001 for all subjects; p=0.001 volunteers only; p=0.016 patients only. Post-registration, free breathing and breath hold images did not have significantly different DSC (p=0.486 for all subjects; p=0.477 volunteers only; p=0.748 patients only), see Table 1. Registered T1 maps were produced for all subjects, see Figures 3 and 4. In volunteers, the inspiration breath hold T1 was significantly lower than the free breathing T1 (p=0.031) whereas there was no significant difference between inspiration breath hold and free breathing lung T1 values in patients with IPF (p=0.574), see Table 1 and Figure 4. The standard deviation (s.d) of T1 values within the lung was not significantly different in inspiration compared to free breathing s.d. of T1 in volunteers (p=0.189) but was significantly higher in inspiration in patients with IPF (p=0.018). Healthy volunteers had significantly higher lung T1 in free breathing, when compared to patients with IPF (p=0.032). There was not a significant difference found in inspiration breath-hold lung T1 values between patients with IPF and volunteers. The s.d. of T1 values within the lung was higher in patients when compared to healthy volunteers (inspiration: p=0.077; free breathing: p=0.092; both: p<0.001).Acknowledgements
No acknowledgement found.References
[1] Stadler, A, et al. (2005b). T1 mapping of the entire lung parenchyma: Influence of respiratory phase and correlation to lung function test results in patients with diffuse lung disease. Magnetic resonance in medicine, 59:96–101.
[2] Mirsadraee, S, et al. (2016). T1 characteristics of interstitial pulmonary fibrosis on 3t mri—a predictor of early interstitial change? Quantitative Imaging in Medicine and Surgery, 6(1):42.
[3] Stadler, A, et al. (2005a). T1 mapping of the entire lung parenchyma: Influence of the respiratory phase in healthy individuals. Journal of magnetic resonance imaging, 21:759–764.
Figures