4088
2D UTE BH lung ventilation imaging at 3T – influence of the repetition time1Department of Internal Medicine II, Ulm University Medical Center, Ulm, Germany, 2AG Experimental Cardiovascular Imaging (ExCaVI), University of Ulm, Ulm, Germany
Synopsis
In this study a two-dimensional ultra-short TE protocol was used to get breath holding (expiration and inspiration) images. It was investigated whether resulting SNR and ventilation and proton density maps can be improved by optimization the TR under given breathhold constraints for multi-slice single breathhold lung imaging. Even though the SNR in the resulting images can clearly be improved by performing an interleaved multi-slice acquisition instead of acquiring slices sub-sequentially, the impact on the resulting parameter maps was not obvious.
Purpose
The feasibility of deriving lung ventilation imaging from ultra-short TE sequences1 has been shown. To enable single breathhold acquisitions, usually as short as possible repetitions times TR are used. Considering the possibility of acquiring multiple slices per breathhold, the question rises whether a multi-slice approach enabling a longer TR may provide better signal to noise as the subsequent acquisition of the slices with minimal TR.Methods
Five healthy volunteers (two female, three male) were examined with a 3T MR scanner (Achieva, Philips Healthcare, Best, The Netherlands). A two-dimensional ultra-short TE (2D UTE) protocol (TE=0.38ms; TR=1.89ms, FA=3.5°) providing three subsequently measured slices within a 15s breathhold was used as basic acquisition scheme and compared to an interleaved multi-slice acquisition with the same (TR=5.6ms, FA=6°) and doubled (TE=10, FA=8°) breathhold duration. The signal intensity and the signal-to-noise ratio were analysed to derive the fractional ventilation2 $$$FV = \frac{SI_{EX} - SI_{IN}}{SI_{EX}}$$$ and proton fraction3 $$$f_P = \frac{SI_{lung}}{SI_{muscle}} \cdot \exp\left( \frac{TE}{T2^*} \right)$$$ of the lung parenchyma. For the calculation of the proton fraction a T2*=0.74ms was assumed.4 Statistical significance of the observed differences was analysed by applying a two-sided paired T-test with p-values below 0.05 being considered significant.
Results
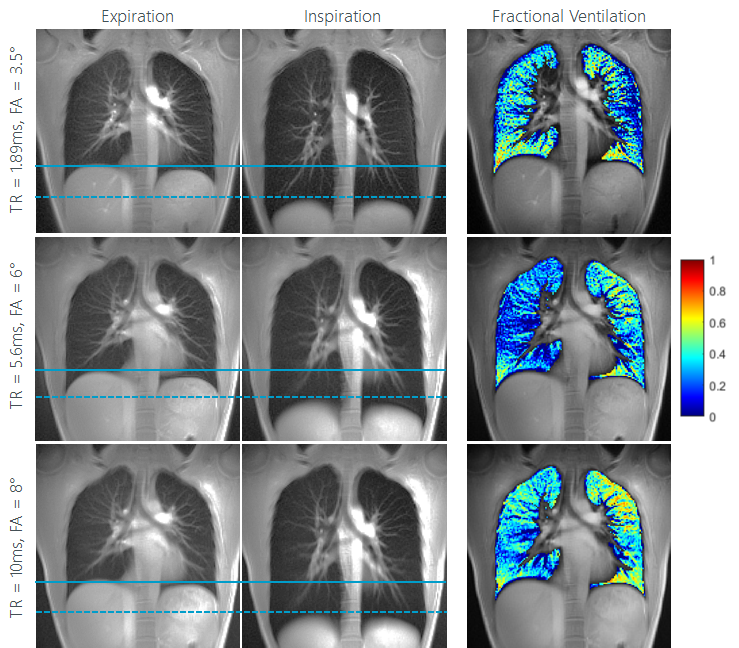
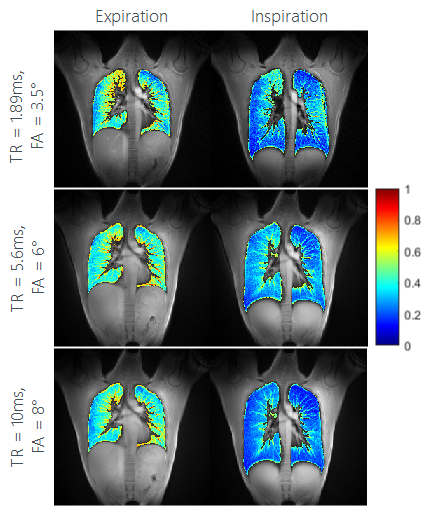
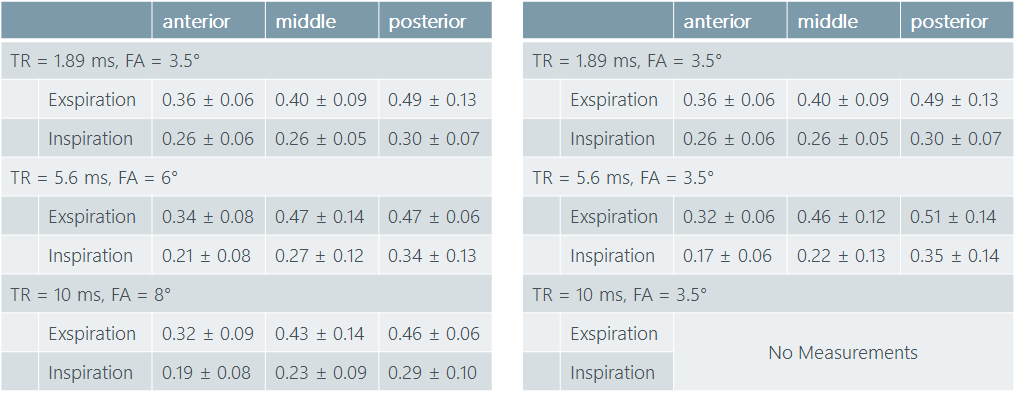
Differences in the lung parenchyma signal intensity between inspiration and expiration could be observed with either method. Ventilation maps could successfully be obtained by the analysis of the signal intensity changes between inspiration and expiration in the BH images (Figure 1) at all TR. The proton fraction (density) could be quantified and clear differences between inspiration and expiration were observed (Figure 2) for all T1. As shown in Table 1, a similar proton fraction gradient from anterior to posterior can be appreciated. No substantial differences between the investigated TRs was observed for the lung ventilation and proton fraction analyses. The SNR shows significant improvement by 45% between TR=1.89ms and TRs 5.6ms and 10ms. No significant differences were observed between TR=5.6ms and TR=10ms.Conclusion
The study shows the feasibility of 2D UTE methods at 3T for the imaging of respiratory motion. The used breathhold length of 15s for TR=1.89ms and 5.6ms appears feasible in capable and cooperative patients5 and show similar quality of the ventilation and proton fraction map. Further prolonging the breathhold to 30s (TR=10ms) seem not to improve the quality of the maps. Regarding signal to noise, clear differences were observed between the TRs investigated. Switching from subsequent acquisition of slices to an interleaved multi-slice acquisition (TR=1.89ms to TR=5.6ms) while keeping breathhold duration constant, yielded a significant improvement in SNR but to no obvious improvement in the parametric maps. Further moderate prolongation of the breathhold duration may not cause any obvious further improvement and considering the likelihood of motion induced image artefacts cannot be recommended. However, in case of acquisition of multiple slices per breathhold, interleaved multislice acquisition should be preferred for SNR reasons.Acknowledgements
The authors thank the Ulm University Center for Translational Imaging MoMAN for its support.References
1. TIBILETTI, Marta ; KJØRSTAD, Åsmund ; BIANCHI, Andrea ; SCHAD, Lothar R. ; STILLER,Detlef ; RASCHE, Volker: Multistage self-gated lung imaging in small rodents. In: Magneticresonance in medicine 75 (2016), Nr. 6, S. 2448–2454
2. KJØRSTAD, Åsmund ; CORTEVILLE, Dominique M. ; HENZLER, Thomas ; SCHMIDBINDERT,Gerald ; HODNELAND, Erlend ; ZÖLLNER, Frank G. ; SCHAD, Lothar R.: Quantitativelung ventilation using Fourier decomposition MRI; comparison and initial study.In: Magnetic Resonance Materials in Physics, Biology and Medicine 27 (2014), Nr. 6, S.467–476
3. HATABU, Hiroto ; ALSOP, David C. ; LISTERUD, John ; BONNET, Mathieu ; GEFTER, WarrenB.: T2* and proton density measurement of normal human lung parenchyma usingsubmillisecond echo time gradient echo magnetic resonance imaging. In: Europeanjournal of radiology 29 (1999), Nr. 3, S. 245–252
4. YU, Jiangsheng ; XUE, Yiqun ; SONG, Hee K.: Comparison of lung T2* during freebreathingat 1.5 T and 3.0 T with ultrashort echo time imaging. In: Magnetic resonancein medicine 66 (2011), Nr. 1, S. 248–254
5. LEDERLIN, Mathieu ; CRÉMILLIEUX, Yannick: Three-dimensional assessment of lungtissue density using a clinical ultrashort echo time at 3 tesla: a feasibility study in healthysubjects. In: Journal of Magnetic Resonance Imaging 40 (2014), Nr. 4, S. 839–847
Figures