4085
Flow-Compensated Ventilation and Perfusion Fourier-decomposition Pulmonary MRI1Robarts Research Institute, London, ON, Canada, 2Medical Biophysics, Western University, London, ON, Canada, 3Radiation Oncology, Stanford University, Stanford, CA, Canada, 4Medical Biophysics, University of Toronto, Toronto, ON, Canada, 5Medicine, Division of Respirology, Western University, London, ON, Canada
Synopsis
Fourier-decomposition pulmonary MRI ventilation and perfusion maps are subject to substantial flow artifacts stemming from cardiac frequencies which makes lung perfusion measurements complex and in some regions of interest, impossible to acquire. We eliminated flow artifacts by shimming only on cardiac regions, instead of the entire field-of-view. Flow compensation improved vessel resolution and segmentation around the heart but also increased the incidence of off-resonance banding artifacts around the diaphragm. MRI ventilation defect percent was greater in flow-compensated versus uncompensated images as well as hyperpolarized gas MRI, demonstrating that ventilation images are highly sensitive to changes in field inhomogeneities.
PURPOSE:
Fourier-decomposition of free-breathing MRI (FDMRI) provides a way to simultaneously generate ventilation and perfusion functional maps by analyzing image intensity oscillations over time.1 Short TR sequences, such as balanced steady-state free-precession (bSSFP), are required to sample beyond the cardiac Nyquist frequency. Due to off-resonance excitation, these maps are highly susceptible to out-of-slice pulsatile flow artifacts.2 This is especially true for higher field (such as 3T) systems, where strong flow artifacts in the frequency encode direction detract from signal-to-noise ratio improvements. When sampling the data just beyond the cardiac Nyquist frequency, cardiac harmonics may be aliased into the respiratory region of the power spectrum, raising the possibility that flow artifacts could negatively impact ventilation images. A proposed solution is targeted shimming to high flow regions, however the impact of cardiac shimming in the lung, a region of strongly varying susceptibility, remains unclear. The objective of this proof-of-concept investigation was to investigate ways to reduce out-of-slice flow artifacts in bSSFP acquisitions using cardiac shimming, and to measure the relationship of the resultant “shimmed” FDMRI ventilation and perfusion maps with hyperpolarized 129Xe MRI and thoracic CT.METHODS:
Subjects and Image Acquisition:
In this proof-of-concept demonstration, two participants provided written informed consent to an ethics-board-approved protocol (NCT02351141). FDMRI was performed using a whole-body 3.0T Discovery MR750 system (General Electric Healthcare, USA) with a 32-channel chest coil. Patients were supine and instructed to freely-breathe for the duration of the scan. Coronal thoracic cavity images were acquired over 500 phases using a balanced steady-state free precession (bSSFP) sequence (image acquisition time = 125s; repetition time/echo time/flip-angle = 1.9ms/0.6ms/15o; field-of-view = 40x40cm2; matrix = 256x256; slice thickness=15mm). Images were acquired twice: once using an automated shim over the entire field-of-view, and subsequently using a manual cardiac shim closely cropped to the heart. 3D Thoracic CT images were axially acquired on a 64‐slice Lightspeed VCT scanner (General Electric Healthcare, Milwaukee, WI) following inhalation and breath-hold of a 1.0L N2 bag from functional residual capacity (FRC). Hyperpolarized gas MRI was also acquired as previously described.3
Image Analysis:
FDMRI maps were generated using an in-house post-processing pipeline running on MATLAB software (MATLAB R2018a; Mathworks, USA).4 Free-breathing images were non-rigidly deformed to correct for motion during the image sequence according to a reference image approximately halfway between FRC and forced vital capacity (FVC). The deformed image was pixel-wise Fourier transformed to generate a series of power spectrum images. The reference image was segmented using a semi-automated continuous max-flow algorithm to generate a lung mask and was applied to the power spectrum image to create a perfusion map. Hierarchical k-means clustering identified functional defect volumes used to calculate perfusion defect percent (QDP) and ventilation defect percent (VDP). Vessel-maps were generated from CT images using Pulmonary Workstation 2.0 (VIDA Diagnostics, USA).
RESULTS:
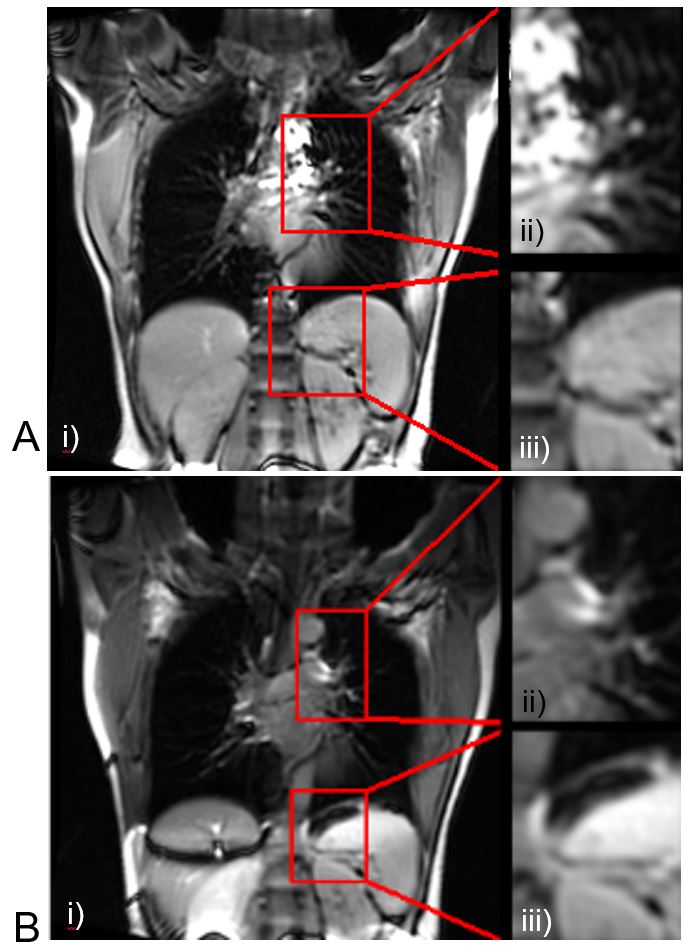
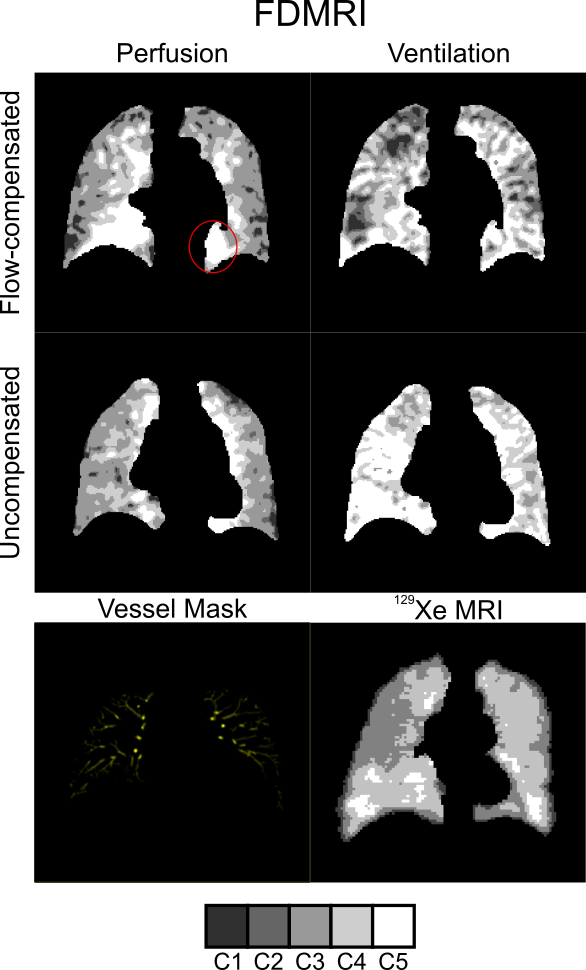
Shimming to the cardiac region eliminated flow artifacts in the compensated images and increased contrast around vessels, as shown in Figure 1, and spatially corresponded with non-contrast thoracic CT vessels. The compensated images had an increased incidence of banding artifacts, especially around the diaphragm. Figure 2 shows the resulting FDMRI ventilation and perfusion cluster maps; the ventilation map changed substantially between methods, with much larger ventilation defects that did not qualitatively match the results observed using 129Xe MRI. 129Xe VDP was 1%, whereas FDMRI VDP was 7% when compensated, and 0% when uncompensated.DISCUSSION:
This proof of concept-investigation showed the result of cardiac shimming on flow artifacts in FDMRI perfusion maps. Flow-compensation resulted in much improved contrast in the region of the heart/lung boundary in the mediastinum. When cardiac versus whole field-of-view shimming was employed, there was a substantial increase in banding artifacts, especially near the diaphragm, due to bSSFP off-resonance effects.5 This did not affect semi-automated segmentation, but may affect future fully-automated segmentation methods. Qualitative and quantitative measurements of VDP were indicative of field inhomogeneity influences on ventilation maps which suggests that independent ventilation and perfusion image acquisitions may be required for optimal results.CONCLUSIONS:
Cardiac shimming successfully removed flow artifacts in perfusion images and improved apparent vascular contrast. This was generated at the cost of field inhomogeneity effects on ventilation maps and measurements which suggests that for optimal FDMRI ventilation and perfusion imaging, independent acquisitions are required.Acknowledgements
No acknowledgement found.References
1. Bauman, G. et al. Magn Reson Med 62, 656-664 (2009).
2. Bernstein, M. A., Huston, J., 3rd & Ward, H. A. J Magn Reson Imaging 24, 735-746 (2006).
3. Svenningsen, S. et al. J Magn Reson Imaging 38, 1521-1530 (2013).
4. Guo, F. et al. in SPIE Medical Imaging 2017. (eds Andrzej Krol & Barjor Gimi).
5. Bieri, O. & Scheffler, K. J Magn Reson Imaging 38, 2-11 (2013).
Figures