4084
A Comprehensive Pipeline for non-contrast enhanced Pulmonary Vascular 1H MRI1Robarts Research Institute, London, ON, Canada, 2Medical Biophysics, Western University, London, ON, Canada, 3Radiation Oncology, Stanford University, Stanford, CA, United States, 4Medical Biophysics, University of Toronto, Toronto, ON, Canada, 5Medicine, Division of Respirology, Western University, London, ON, Canada
Synopsis
Structure-function relationships are central to our understanding of pulmonary disease and play an important role in evaluating novel therapies. Many chronic lung diseases, such as asthma and chronic obstructive pulmonary disease (COPD), have vascular abnormalities that are not accounted for in current image analysis platforms. Recent MRI developments provide complementary pulmonary vascular structural and functional information and include ultra-short echo time and Fourier-decomposition MRI. To facilitate clinical translation, we developed a comprehensive structure-function pipeline to visualize and measure pulmonary vascular vessel trees and perfusion for patients with severe asthma, a demanding clinical target.
PURPOSE:
Chronic lung disease is regionally heterogeneous, progressive and debilitating. A deep understanding of the structure-function relationships that drive lung disease pathogenesis has been elusive, mainly because clinical measurement tools are relatively insensitive to the pathologies that initiate and drive disease progression. Pulmonary vascular pruning was previously observed in patients with chronic obstructive pulmonary disease (COPD)1 and asthma.2 While these vascular findings have been illuminating, previously developed MRI and x-ray computed tomography (CT) structure/function biomarker pipelines have focused on airways and ventilation instead of pulmonary vessels and perfusion.3 Although contrast-enhanced and non-contrast CT vessel trees are currently used clinically to diagnose patients with suspected pulmonary embolism, MRI methods such as ultra-short echo time (UTE) MRI4 and Fourier-decomposition MRI (FDMRI)5 also hold promise for these investigations. Short echo-times make UTE MRI less influenced by magnetic susceptibility artifacts,4 making it suitable for chest examinations, while the dynamic nature of FDMRI is well-suited to perfusion imaging. Therefore, our objective was to generate a comprehensive structure-function algorithm pipeline that provides MRI biomarkers of vascular tree structure and function which may be integrated into existing clinical workflows.METHODS:
Participants and Image Acquisition:
Participants with severe asthma provided written informed-consent to an approved protocol (NCT02351141). FDMRI was performed using a whole-body 3.0T Discovery MR750 system (General Electric Healthcare, USA) with a 32-channel chest coil. Patients were placed supine and 500 centre-slice coronal images were acquired during free-breathing using a balanced steady-state free precession (bSSFP) sequence (image acquisition time = 125s; repetition time/echo time/flip-angle = 1.9ms/0.6ms/15o; field-of-view = 40x40cm2; matrix = 256x256; slice thickness=15mm). UTE MRI was performed using a 3D cones-based UTE sequence.6 Patients were placed supine and coached to achieve breath-hold volumes of full inspiration, full expiration, functional residual capacity, and functional residual capacity plus 1L by inhalation of a 1L bag of N2. Coronal whole lung images were acquired using a UTE GEHC sequence (image acquisition time = 15s; repetition time/echo time/flip-angle = 3.5ms/0.03ms/58o; field-of-view = 40x40cm2; matrix = 200x200; slice thickness=10mm). B1 field mapping was performed using a dual angle 3D Look-Locker pulse sequence (acquisition time = 40s; repetition time/echo time = 1200ms/0.3ms; α/2α = 5o/10o; field-of-view=48x48cm2; matrix = 32x32; slice thickness = 15mm) using the 3T GE phantom model 2360049 (GEHC).
Image Analysis:
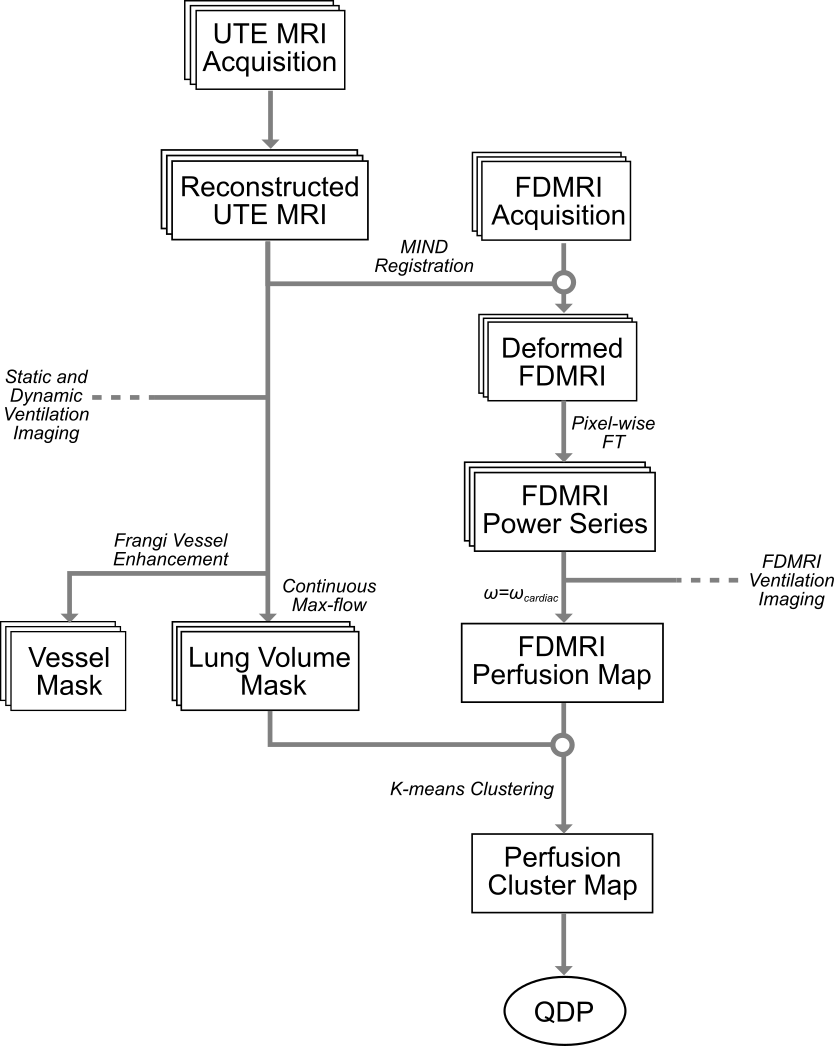
Figure 1 outlines the pipeline components. Images were analyzed using an in-house post-processing pipeline utilizing MATLAB utilities (MATLAB R2018a; Mathworks, USA). The centre UTE slice was used as a reference to non-rigidly deform the FDMRI sequence using a deformable registration algorithm as previously described.7 From the UTE image, the lungs were segmented using a continuous max-flow algorithm7 to generate a lung mask. Vessels were enhanced by applying a Frangi vesselness filter8 followed by thresholding. The deformed FDMRI series was pixel-wise Fourier transformed to produce a power-spectrum image sequence of functional performance. The cardiac frequency was determined from the highest intensity peak above 0.3Hz in the power series. The UTE lung mask was applied to perfusion images, followed by application of a hierarchical k-means clustering algorithm, and finally calculation of perfusion defect percent (QDP) from the lowest cluster volume.
RESULTS:
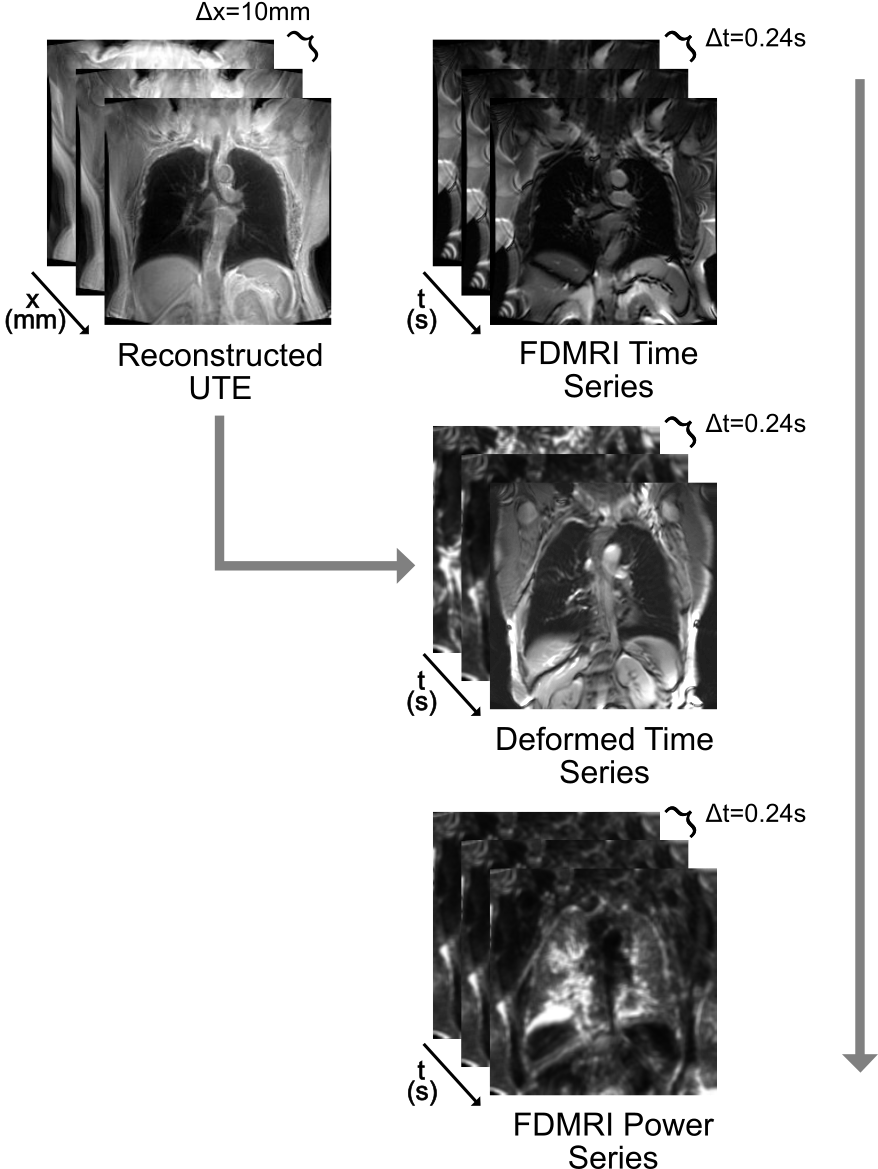
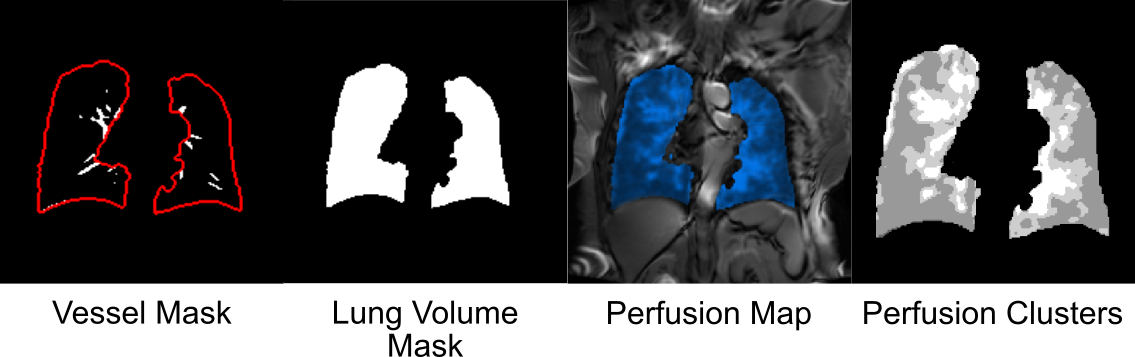
The ionization-free acquisition process was performed in under five minutes. 11 asthmatics were evaluated using the proposed semi-automated7 algorithm pipeline and required approximately 15 minutes on a desktop with an Intel® i7-3770 CPU and a GeForce GTX 680 GPU. Figure 2 shows the input image sequences and the resulting intermediary image sequences, while Figure 3 shows output images of the pipeline. The pipeline provided structural information from UTE structural anatomy (including thoracic cavity and major vessels) as well as lung and vessel masks that were used to generate perfusion maps.DISCUSSION:
The combination of UTE and FDMRI provides a new option for chest imaging investigations that is time- and cost-efficient, patient-friendly and compatible with existing respiratory biomarker pipelines. A unified pipeline allows for the strengths of UTE MRI to be applied to functional FDMRI results; the diminished slice thickness and reduced motion artifacts of UTE augments segmentation precision and accuracy, especially around the heart, and associated vessel trees provide complementary information to FDMRI perfusion maps. This MRI-only pipeline was advantageous for registration because of similar signal intensities and vesselness filters isolated major vessels. Still, spatial resolution (UTE) remains a notable limitation requiring technical developments.CONCLUSIONS:
Non-contrast pulmonary 1H MRI in combination with efficient algorithm pipelines may be exploited together to rapidly and safely generate pulmonary vascular structural and functional information in patients.Acknowledgements
No acknowledgement found.References
1. Estepar, R. S. et al. Am J Respir Crit Care Med 188, 231-239 (2013).
2. Ash, S. Y. et al. Am J Respird Crit Care Med 198, 39-50 (2018).
3. Guo, F. et al. J Med Imaging (Bellingham) 5, 026002 (2018).
4. Johnson, K. M. et al. Magn Reson Med 70, 1241-1250 (2013).
5. Bauman, G. et al. Magn Reson Med 62, 656-664 (2009).
6. Sheikh, K. et al. J Magn Reson Imaging 45, 1204-1215 (2017).
7. Guo, F. et al. in SPIE Medical Imaging 2017. (eds Andrzej Krol & Barjor Gimi).
8. Frangi, A. F. et al. in MICCAI 1998. Vol. 1496 (eds A Colchester & SL Delp) 130-137 (Berlin, Germany, 1998).
Figures