4083
Imaging functional and microstructural changes in the lungs of children born prematurely1POLARIS, Academic Radiology, IICD, The University of Sheffield, Sheffield, United Kingdom, 2Department of Child Health, School of Medicine, Cardiff University, Cardiff, United Kingdom
Synopsis
Preterm-births account for 10% of worldwide births, and those born at 32 weeks gestation or less have deterioration in their lung function in childhood and beyond. Here we assessed pulmonary micro-structural and functional changes using hyperpolarized 129Xe gas ventilation and diffusion-weighted MRI in three groups of children: (1) those born preterm with FEV1<=85%, (2) born preterm with normal lung function and (3) those born full term with normal lung function. Significant differences in ventilation heterogeneity and the kurtosis of the distribution of mean alveolar dimension were observed between groups.
Introduction
Preterm-births account for 10% of worldwide births, and those born at 32 weeks gestation or less have deterioration in their lung function in childhood and beyond. A combination of birth at an early stage of lung development and postnatal interventions such as mechanical ventilation and supplemental oxygen therapy can lead to the development of bronchopulmonary dysplasia, BPD, for example. Previously, 3He apparent diffusion coefficient (ADC) has been shown to be elevated in children born preterm with BPD compared to term born controls1, and 1H structural MRI scores have been shown to correlate with BDP severity and clinical outcomes in neonates2. The purpose of this study was to assess functional and microstructural changes in the lungs of children born prematurely alongside healthy controls born at full term using hyperpolarized 129Xe ventilation and diffusion weighted MRI and multiple breath washout (MBW).Methods
38 children with mean age 11.5 years were studied. The children were split into three groups based on their term of birth and lung function in childhood: (1) those born preterm with FEV1<=85%, (2) born preterm with normal lung function and (3) born full term with normal lung function. Hyperpolarized 129Xe MRI was performed at 1.5 T (GE HDx) using a flexible transmit/receive quadrature vest coil and a 129Xe polarizer for gas generation3. For all 129Xe exams the subjects inhaled a gas mixture of 129Xe and N2 from FRC and held their breath for 10-16 seconds. Gas mixture volume and 129Xe doses were adjusted according to the subjects’ heights to account for differences in lung volume and 129Xe concentration.
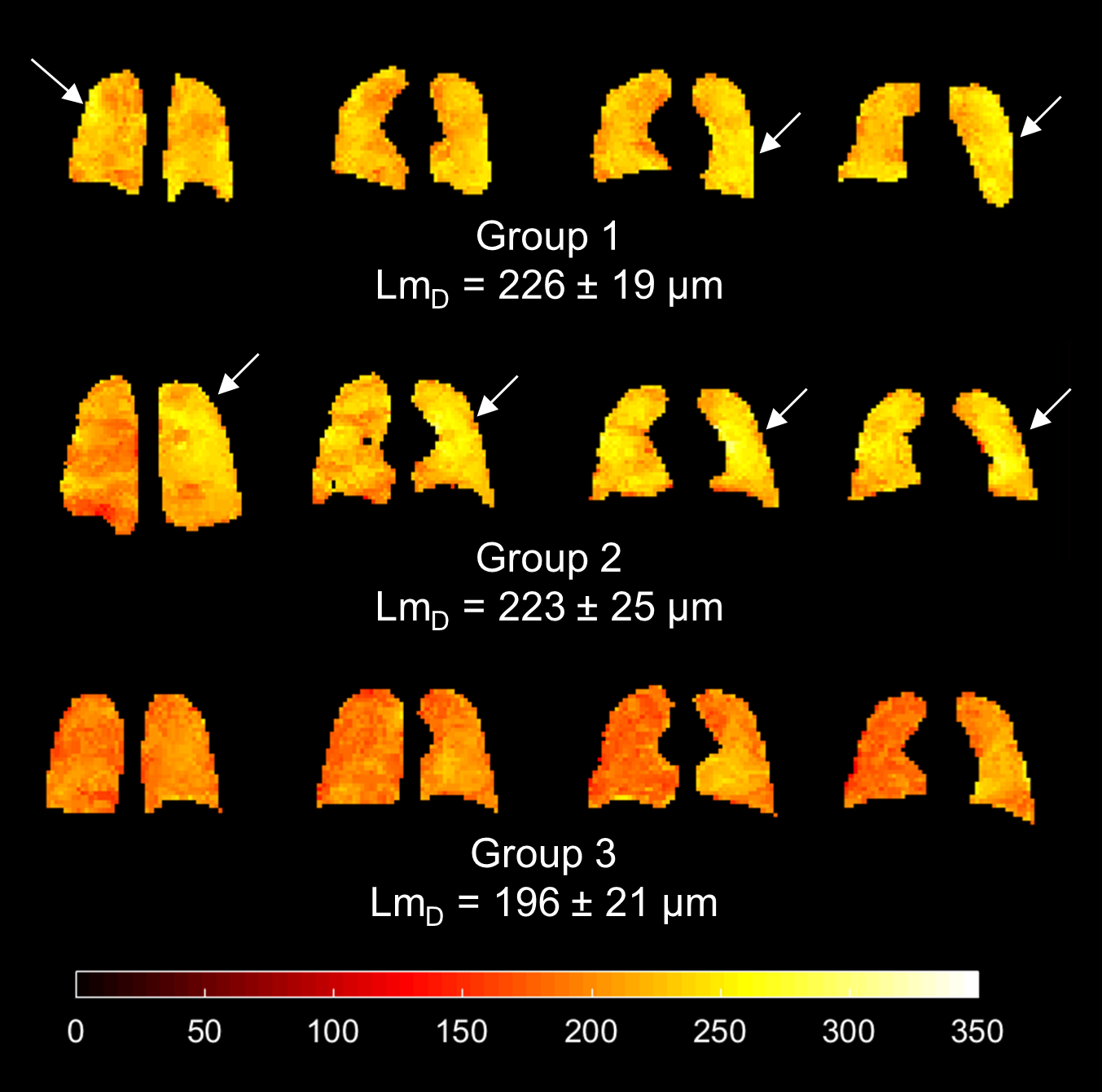
129Xe diffusion-weighted MRI was acquired with a 3D multiple b-value SPGR sequence with compressed sensing4 using the following parameters: Δ=8.5 ms, b-values=[0, 12, 20, 30] s/cm2, TE/TR=14.1/17.4 ms, BW =±6.94 kHz, voxel=6.25x6.25x15 mm3, FA=3.1°, FOV=40x32x24 cm3. ADC maps were computed from the first two b-value images. In addition, all four b-value images were used to derive estimates of mean alveolar dimension (LmD) from the stretched exponential model4. Histograms of ADC and LmD values across the entire lung were analyzed for full width at half maximum (FWHM), skew and kurtosis. 3D 129Xe ventilation imaging was performed with a 3D SSFP sequence5 and the ventilation defect percentage (VDP) and coefficient of variation of image intensity (CV%), both indicators of ventilation heterogeneity, were computed6,7.
MBW was performed with a modified open-circuit Innocor (0.2% SF6) in order to calculate the lung clearance index (LCI).
Kruskal-Wallis tests were performed (GraphPad Prism 7.04) to assess differences across groups.
Results and Discussion
Of the 38 subjects, 36 had successful ventilation imaging. Results are summarized in table 1 and example images are shown in figures 1 and 3. VDP was significantly different between the groups (p=0.0133); specifically, for groups 1-3 p=0.0184, and for groups 2-3 p=0.0262. CV% was also significantly different between the groups (p=0.0311) with a significant difference between groups 1-2 (p=0.0407) only. The two ventilation-imaging based metrics were effective and complementary in discriminating the subject groups (figure 2). Preterm born subjects had significantly higher VDP than healthy controls. Within preterm born subjects, ventilation heterogeneity (CV%) was significantly lower in subjects with normal lung function. A trend towards elevated global mean 129Xe ADC and LmD values was observed in the preterm born subjects (groups 1 and 2) compared to the full term control subjects (figure 4); however, this was not significant (p=0.508 and p=0.591, respectively). LmD kurtosis (p=0.019) was the only histogram metric to show a significant difference between the groups, significantly lower in preterm born subjects (group 1 (p=0.02) and group 2 (p=0.05)) with respect to control subjects. This decrease in LmD kurtosis suggests an increase in the number of extreme/outlier values, and may reflect increased heterogeneity of alveolar dimensions. This is qualitatively supported by regions of elevated ADC and LmD observed in some preterm born subjects (figure 3). Only 3/38 subjects studied had an abnormal LCI (>7.4)8, with one subject from each group being abnormal which resulted in no significant difference for LCI between the three groupsConclusion
129Xe ventilation defect percentage was significantly higher in children born preterm than in-term born children, and for children born preterm ventilation heterogeneity measured by CV% was significantly higher in those with FEV1<=85%. The kurtosis of the distribution of mean alveolar dimension (LmD) was significantly lower in children born preterm when compared to those born at term suggesting an increased heterogeneity of alveolar dimensions. 129Xe ventilation and diffusion imaging detected functional and microstructural changes in the lungs of children born prematurely, neither of which were detected by FEV1 or multiple-breath washout.Acknowledgements
This work was funded by the Medical Research Council (MR/M008894/1) and the National Institute of Health Research (NIHR-RP-R3-12-027). The views expressed in this publication are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research or the Department of Health.References
1. Flors L, Mugler J P III, Paget-Brown A, Froh D, de Lange E E, Patrie J T, Altes T A, "Hyperpolarized helium-3 diffusion-weighted magnetic
resonance imaging detects abnormalities of lung structure in children with
bronchopulmonary dysplasia" J Thorac
Imaging 2017 32(5):323-32.
2. Higano N S, Spielberg D R, Fleck R J, Schapiro A H, Walkup L L, Hahn A D, Tkach J A, Kingma P S, Merhar S L, Fain S B, Woods J C, "Neonatal pulmonary MRI of bronchopulmonary dysplasia predicts short-tem clinical outcomes" Am J Respir Crit Care Med 2018, doi: 10.1164/rccm.201711-2287OC
3. Norquay G, Collier G J, Rao M, Stewart N J, and Wild J M, "129Xe-Rb Spin-Exchange Optical Pumping with High Photon Efficiency" Phys. Rev. Lett. 121, 153201.
4. Chan H F, Stewart N J, Norquay G, Collier G J, and Wild J M, "3D diffusion-weighted (129) Xe MRI for whole lung morphometry" Magn Reson Med, vol. 79, pp. 2986-2995, Jun 2018.
5. Stewart N J, Norquay G, Griffiths P D, and Wild J M, "Feasibility of human lung ventilation imaging using highly polarized naturally abundant xenon and optimized three-dimensional steady-state free precession" Magn Reson Med, vol. 74, pp. 346-52, Aug 2015.
6. Hughes P J C, Horn F C, Collier G J, Biancardi A, Marshall H, and Wild J M, "Spatial fuzzy c-means thresholding for semiautomated calculation of percentage lung ventilated volume from hyperpolarized gas and (1) H MRI" J Magn Reson Imaging, vol. 47, pp. 640-646, Mar 2018.
7. Biancardi A M, Acunzo L, Marshall H, Tahir B A, Hughes P J C, Smith L, Weatherley N D, Collier G J, Wild J M, "A paired approach to the segmentation of proton and hyperpolarized gas MR images of the lungs" in Proceedings of ISMRM, Paris, 2018, no 2442.
8. Horsley A R, Gustafsson P M, Macleod K A, Saunders C, Greening A P, Porteous D J, et al. "Lung clearance index is a sensitive, repeatable and practical measure of airways disease in adults with cystic fibrosis" Thorax, vol. 63, pp. 135-40, Feb 2008
Figures