4081
Real-Time Imaging during Free Breathing for Patient-Friendly V/Q Scan of the Whole Lung in One Minute at 3T1Institute of Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 2Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), German Center for Lung Research (DZL), Hannover, Germany, 3Magnetic Resonance, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
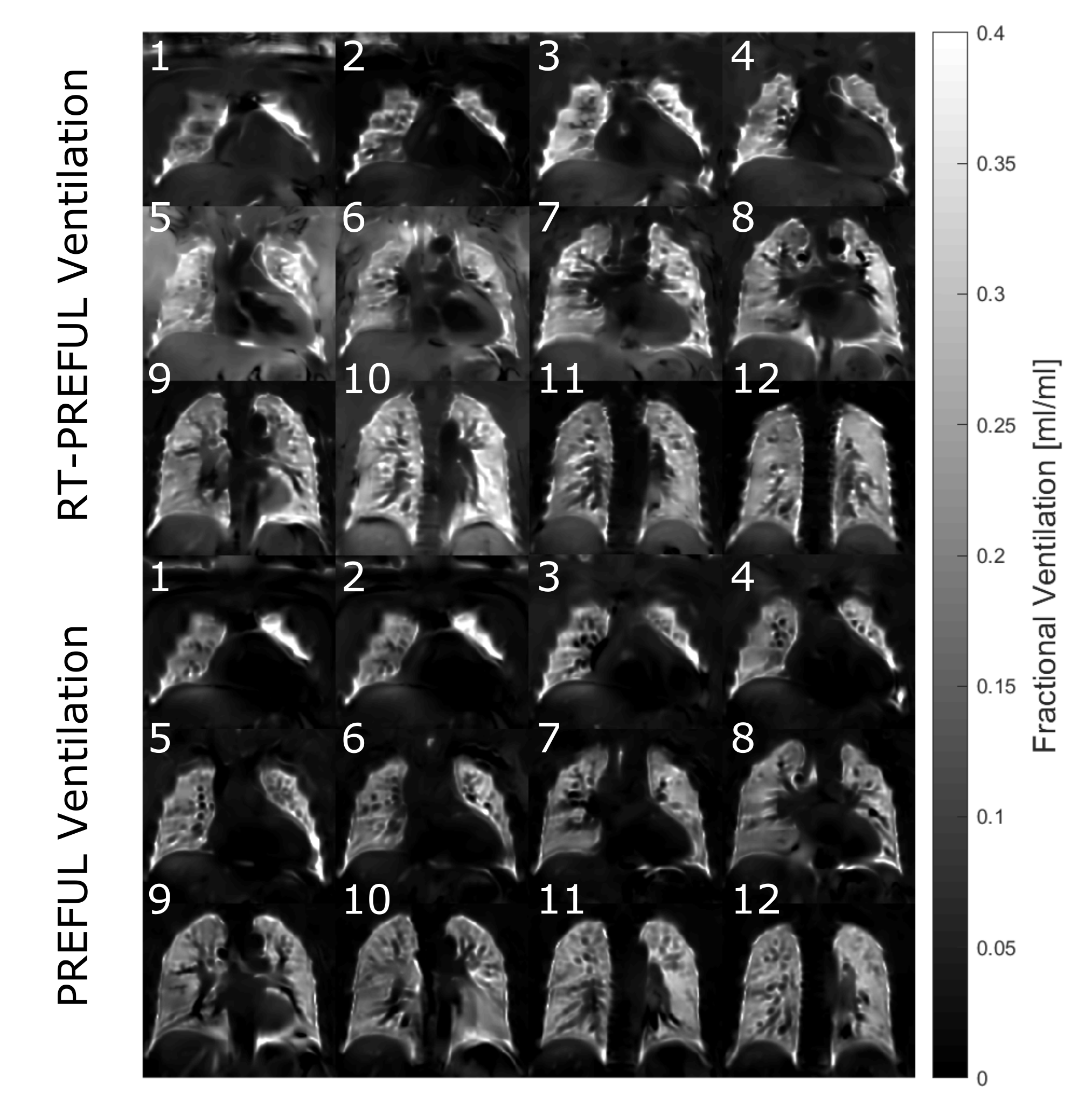
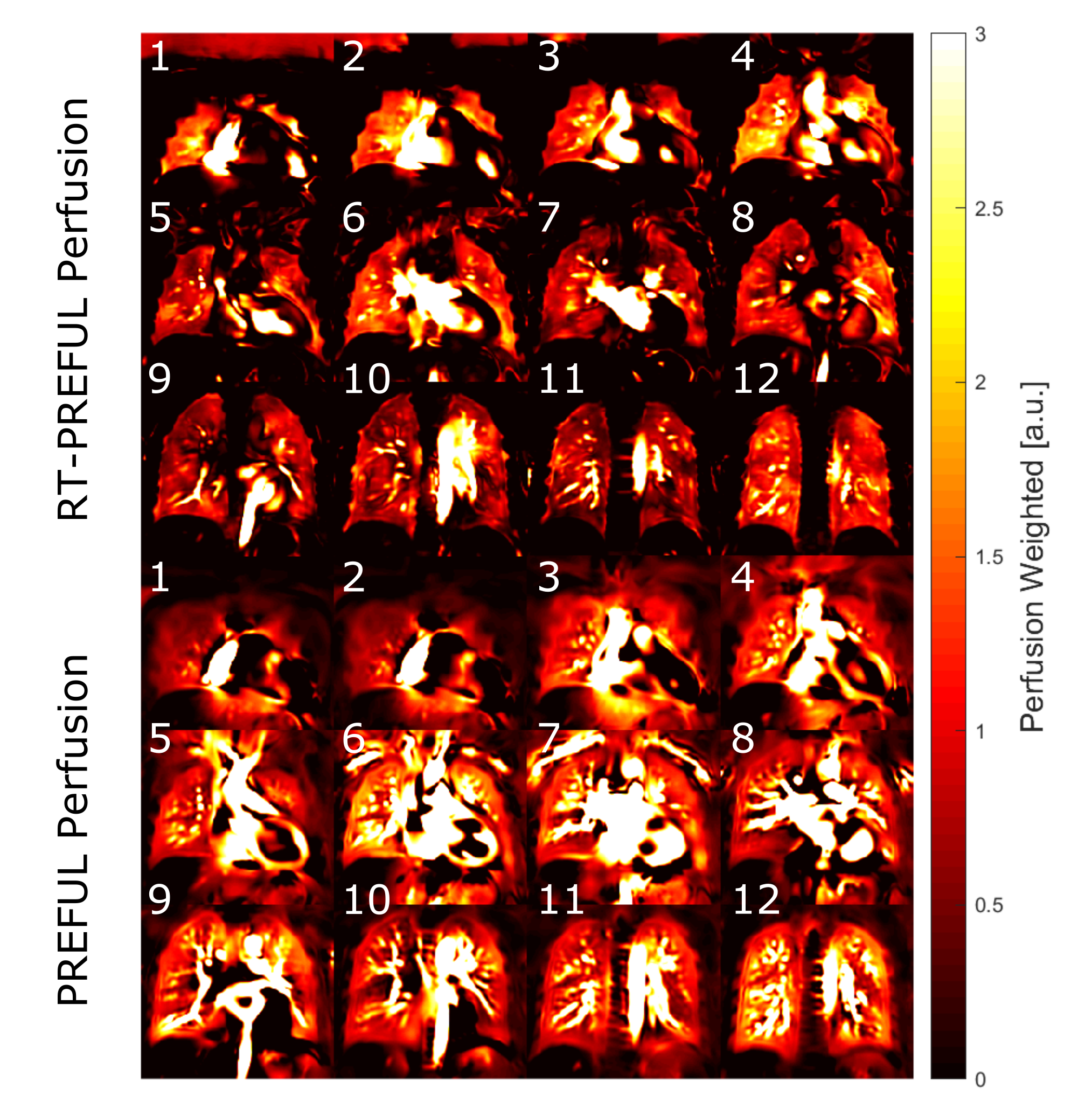
MRI techniques like phase-resolved functional lung imaging (PREFUL) offer the possibility for pulmonary ventilation (V) / perfusion (Q) imaging without ionizing radiation or contrast agents. One major drawback of such methods is the long acquisition time, if a whole lung coverage is required. In this study, five healthy volunteers were scanned with a highly accelerated 2D multi-slice real-time PREFUL (RT-PREFUL) acquisition with compressed sensing and parallel imaging reconstruction to establish a V/Q scan of the whole lung in one minute. The comparison with conventional PREFUL technique showed very similar ventilation results and comparable perfusion results with 9-fold acceleration.
Introduction
The recent developments and studies demonstrate the potential of V/Q lung imaging without ionizing radiation or contrast agents in free breathing using MRI techniques like Fourier Decomposition1 (FD), SENCEFUL2 or phase-resolved functional lung (PREFUL)3 imaging. Long acquisition times of the whole lung (~12 minutes) are a relevant drawback considering the limited scan slots in clinical routine. Also a real-time acquisition is desirable to avoid the use of simplified assumptions. Bauman et al. demonstrated the feasibility of a high temporal resolution single-slice FD acquisition using a radial balanced steady-state free precession (bSSFP) sequence at 1.5T4. The purpose of this study was to demonstrate the feasibility of an accelerated pseudo-random 2D Cartesian real-time PREFUL (RT-PREFUL) multi-slice acquisition with reduced total acquisition time and increased temporal resolution using compressed sensing and parallel imaging at 3T.Methods
Acquisition: Five healthy volunteers (age 26-43 years) underwent 3T MRI (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) using a standard spine coil in combination with a 18-channel body coil. PREFUL and RT-PREFUL were used for a multi-slice 2D acquisition of the whole lung during free-breathing. For PREFUL, a spoiled gradient echo sequence with the following parameters was used to acquire 500 images for each slice: TE 0.83 ms, TR 1.93 ms, FA 4°, matrix 128 x 128, field of view 50 x 50 cm2, slice thickness 10 mm, bandwidth 1500 Hz / pixel, GRAPPA with acceleration factor 2, a temporal resolution of 123 ms and a total acquisition time of 62 s / slice. For RT-PREFUL, an ECG-gated pseudo-random Cartesian spoiled gradient echo prototype sequence (as described by Liu et al.5) with TR 2.3 ms, TE 1.05 ms, acceleration factor 9.1, temporal resolution 32 ms and otherwise identical parameters as PREFUL with online compressed sensing reconstruction was used. Each slice was acquired during one heartbeat with an average number of 30 cardiac phases depending on the heart rate. To capture different respiratory phases and ensure sufficient SNR, the measurement was repeated six times resulting in a total acquisition time of ~ 1 minute.
Post-Processing: For motion correction, non-rigid registration was performed using advanced normalization tools (ANTs)6,7. The PREFUL acquisitions were sorted to create one respiration and perfusion cycle as previously described3 to generate fractional ventilation (FV) and perfusion-weighted (Qw) phase-resolved maps. For RT-PREFUL, no additional perfusion sorting was necessary due to cardiac gating. The respiratory cycle was sorted according to diaphragm position. Since the steady state was not reached during the short acquisition, additional filtering using a lag-3 difference (order 1) operator was applied prior to Qw calculation. To avoid perfusion and transient-state effects, the FV calculation was only performed for measurements with equal cardiac phases.
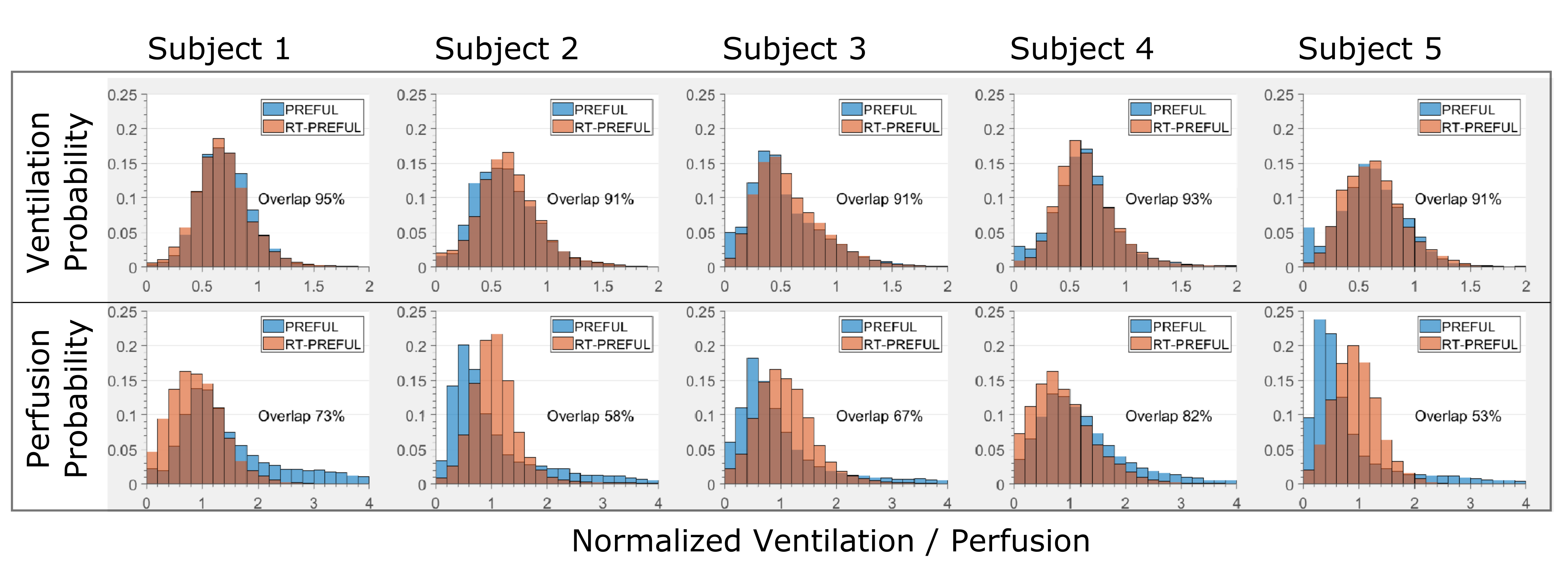
Quantitative analysis: The lung parenchyma
was segmented as region of interest (ROI) by manual segmentation. For histogram
analysis, the lung parenchyma perfusion / ventilation values of all slices were
concatenated into one sample for each subject and normalized using the
respective 90% percentile. To compare the distribution similarity, the overlap
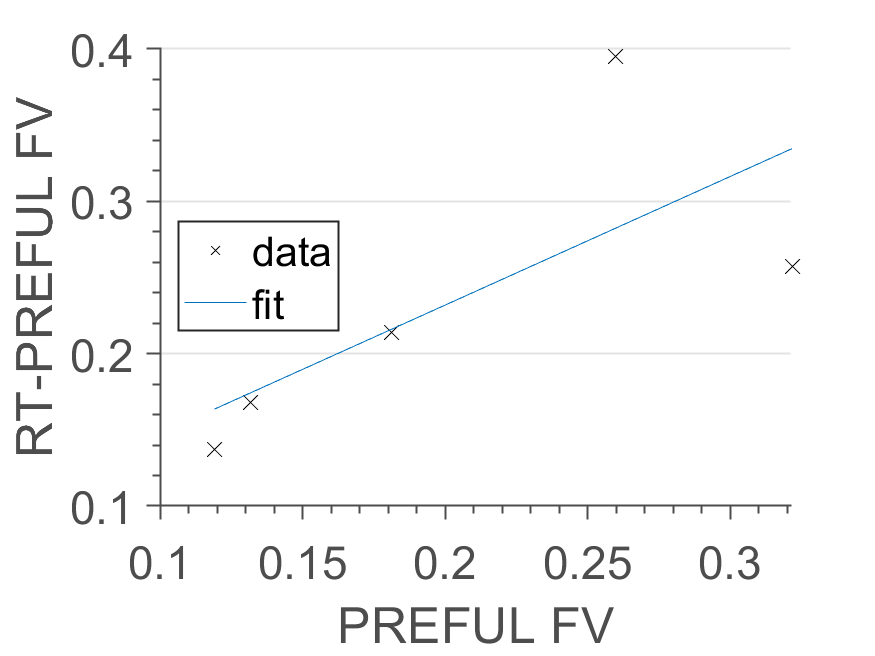
of the histograms was evaluated. Whole-lung median PREFUL and RT-PREFUL FV were
analyzed with Pearson correlation coefficient.
Results
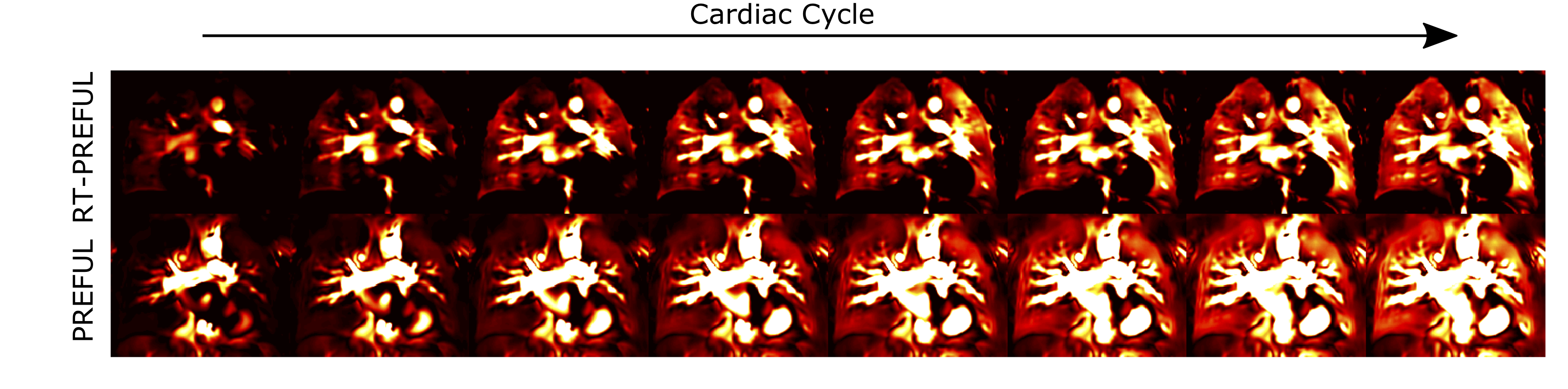
In concordance with the visual comparison (see Figure 1, 2), strong histogram overlap (see Figure 3) was obtained for ventilation (91%-95%) and moderate for perfusion (53%-82%). The comparison of whole-lung median FV showed a strong correlation (R=0.84, see Figure 4). The comparison of the cardiac cycle showed a good visual concordance for both techniques (see Figure 5).Discussion
Despite reduced total acquisition time (12 minutes vs. 1 minute) RT-PREFUL shows very similar results for ventilation and comparable perfusion imaging quality on a 3T scanner in comparison with PREFUL. Nevertheless, there were differences in background and vessels appearance, which were more pronounced on the PREFUL Qw results. A possible explanation is more effective motion freezing of RT-PREFUL due to higher temporal resolution and cardiac gating. While simplified assumptions are made to reconstruct cardiac cycles in PREFUL, the dynamic evolution of Qw images was similar to RT-PREFUL. Remaining differences can be potentially explained by extensive filtering during post-processing. In this regard, further optimization, e.g. regarding transient state and validation in patients, should be addressed in the near future. Although it is an attractive alternative approach to use a 3D acquisition8, we are unaware of a method which maintains the contrast contribution from perfusion, which is necessary for V/Q imaging.Conclusion
This study shows that recent advances in sequence design and reconstruction in combination with adapted PREFUL post-processing enable the feasibility of real-time V/Q acquisition of the whole lung in a reasonable time frame, which is of importance for clinical translation.Acknowledgements
This work was supported by Siemens Healthcare GmbH and the German Centre for Lung Research (DZL).References
1. Bauman G, Puderbach M, Deimling M, et al. Non-contrast-enhanced perfusion and ventilation assessment of the human lung by means of fourier decomposition in proton MRI. Magn Reson Med. 2009;62(3):656-664. doi:10.1002/mrm.22031
2. Fischer A, Weick S, Ritter CO, et al. SElf-gated Non-Contrast-Enhanced FUnctional Lung imaging (SENCEFUL) using a quasi-random fast low-angle shot (FLASH) sequence and proton MRI. NMR Biomed. 2014;27(8):907-917. doi:10.1002/nbm.3134
3. Voskrebenzev A, Gutberlet M, Klimeš F, et al. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018;79(4):2306-2314. doi:10.1002/mrm.26893
4. Bauman G, Eichinger M, Uecker M. High temporal resolution radial bSSFP sequence with nonlinear inverse reconstruction for the measurement of the pulmonary blood inflow time using Fourier decomposition MRI. In: Proc. Intl. Soc. Mag. Reson. Med. 20. ; 2012:1.
5. Liu J, Rapin J, Chang T, et al. Dynamic cardiac MRI reconstruction with weighted redundant Haar wavelets. In: Proc. Intl. Soc. Mag. Reson. Med. 20. ; 2012:4249.
6. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A Reproducible Evaluation of ANTs Similarity Metric Performance in Brain Image Registration. Neuroimage. 2011;54(3):2033-2044. doi:10.1016/j.neuroimage.2010.09.025
7. Voskrebenzev A, Gutberlet M, Kaireit TF, Wacker F, Vogel-Claussen J. Low-pass imaging of dynamic acquisitions (LIDA) with a group-oriented registration (GOREG) for proton MR imaging of lung ventilation. Magn Reson Med. 2017;78(4):1496-1505. doi:10.1002/mrm.26526
8. Pusterla O, Bauman G, Wielpütz MO, et al. Rapid 3D in vivo 1H human lung respiratory imaging at 1.5 T using ultra-fast balanced steady-state free precession. Magn Reson Med. 2017;78(3):1059-1069. doi:10.1002/mrm.26503
Figures