4079
Validation of Fourier Decomposition Lung MR Perfusion using Breath-hold Correction1Medical Radiation Physics & Nuclear Medicine, Karolinska University Hospital, Stockholm, Sweden
Synopsis
Co-registration of free breathing coronal lung images in Fourier decomposition (FD) lung MRI is a crucial part of the processing pipeline for this technique. It is vital that the registration works on the correct parts of the image and does not interfere with the data in an unfavourable way. This work aims to evaluate the extent to which registration affects the perfusion, and by association the ventilation results of this technique, using a breath-hold acquisition as a gold standard. Results encourage the generation of confidence maps to aid interpretation of FD lung MR results, particularly in regions affected by registration.
Introduction: Fourier decomposition (FD) lung magnetic resonance (MR) imaging is a non-invasive method with potential for evaluating perfusion/ventilation mismatch in lung pathologies such as chronic obstructive pulmonary disease (COPD) and Cystic Fibrosis (CF) [1,2]. It is a relatively new and unused method which, although potentially very useful, still requires thorough clinical validation. One of the major advantages of the technique is its non-invasive nature, involving a non-ionizing, free breathing, short duration MRI scan. In brief, the method involves evaluating the signal over time and subsequent frequency response of lung parenchyma throughout free breathing. This is done by acquiring a large dynamic dataset of the lung and deformably registering each frame to a mid-breath state. A Fourier Transform (FT) is then applied to the time-series data on a voxel-by-voxel basis followed by gaussian fitting and integration of peaks thought to be responsible for: 1) The compression of the parenchyma which can be linearly related to ventilation, and 2) the pulsation of blood throughout the parenchyma which is equated to bulk perfusion of the lung. This generates magnitude maps of ventilation and perfusion, comparable to those of nuclear medicine V/Q scans. The accuracy of the deformable registration applied to the data inevitably affects the final results which may be used in clinical diagnosis. This is of particular importance in patients where early stage pathology starts in the basal regions of the lung. This work aims to evaluate the extent of these inaccuracies, by comparing the perfusion portion to a breath-hold acquisition, in order to establish and validate this technique for future clinical trials.
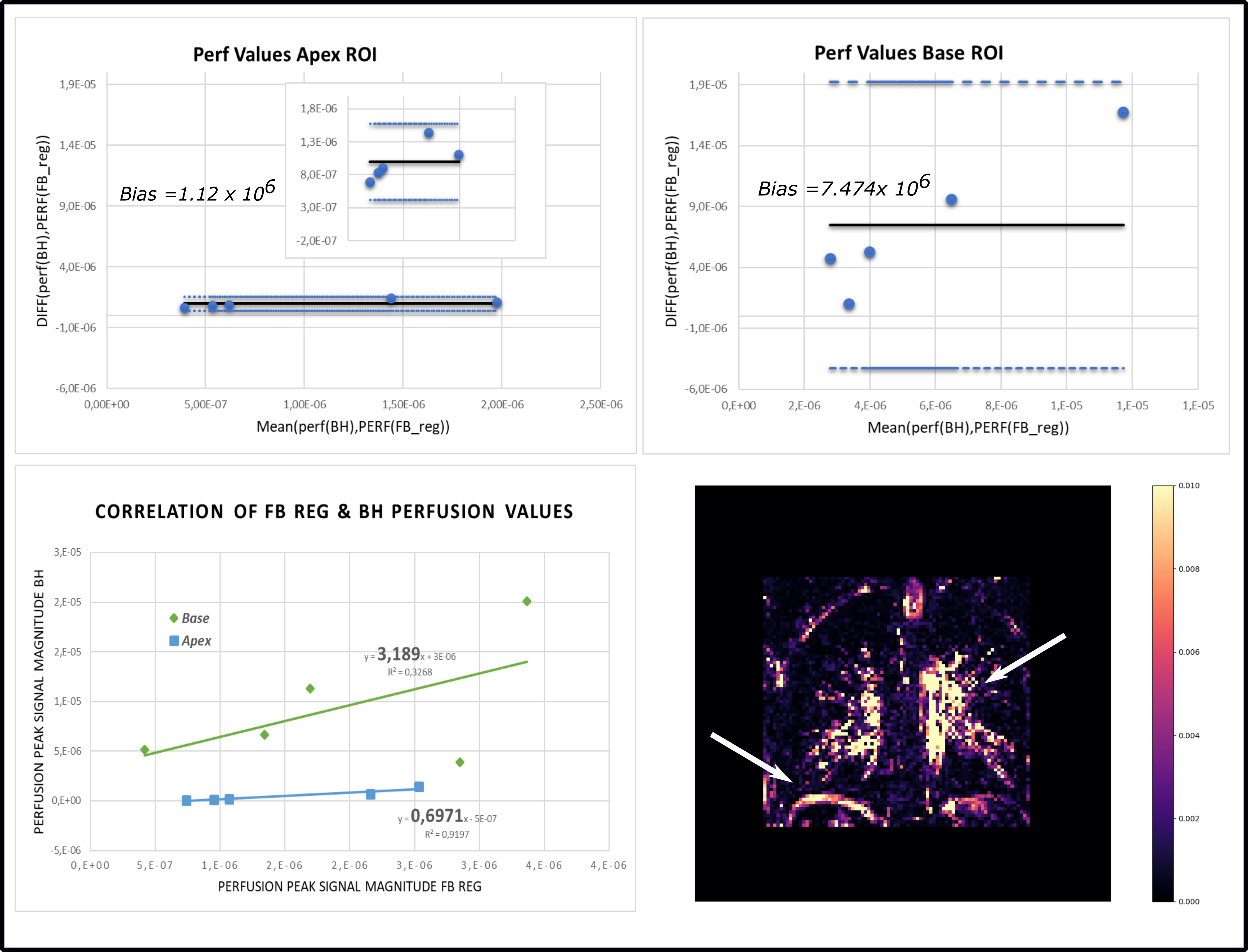
Methods: Five healthy volunteers were scanned at 1.5T using a Philips Ingenia MRI scanner. Subjects were asked to free-breathe for approximately 1.5 minutes, throughout which 500 images were acquired at a temporal resolution of 0.146 s. Sequence parameters: Coronal SSFP, TE=0.579 ms, slice thickness=10mm, 3.1x3.1 mm in-plane spatial resolution. This was followed by a separate acquisition throughout an instructed breath-hold (18 s) in a mid-tidal state (in order to minimise registration errors). Free-breathing images were registered using a demons deformable registration algorithm (SimpleITK, Inside Software Consortium) with 128 iterations and a reference image chosen based on a minimisation algorithm matching the breath-hold acquisition. In-house software written in Python 3.6 was used to analyse the data and compute ventilation/perfusion maps. Using the Perfusion map (Q-BH) generated from the breath-hold FD-MR acquisition as the gold standard, data from regions of interest, ROIs, in the apical and basal regions of the lung from Q-BH and Q-FB (free-breathing registered data perfusion map) were compared in order to evaluate the potential error caused by the registration. Fractional Weighting (FW) maps, the result of an absolute voxel by voxel subtraction of Q-BH and Q-FB were generated for all subjects and aim to aid and caution radiologists with the interpretation of the FD-MRI data.
Results and Discussion: Parenchymal perfusion was found to slow down as a consequence of the subject holding their breath and manifests as a slight shift in the perfusion peak in the Fourier spectrum, indicated in (Fig1b,d). There is a complete lack of ventilation peaks present in the breath-hold acquisition and some evidence of aliased signal in the registered free-breathing dataset. Results show a significant difference in Q-BH and Q-FB in regions affected by bulk motion and thus registration (Fig2d). ROI analysis in the apical regions of the lung show a high correlation between the two methods (Q-BH and Q-FB) and a low bias, in contrast to the basal regions affected by registration (Fig2a-c). Elevated values in the FW maps for the five subjects show areas that are due to a combination of unavoidable registration errors as well as bronchial tree mismatch between the two acquisitions. These results highlight the need for caution when interpreting ventilation/perfusion mismatch in regions heavily affected by registration. Skewing of the data is inevitable when performing a non-rigid registration and the effects of this must be taken into account. Future work aims to extend this study to quantify the error in the ventilation maps caused by the registration in FD lung MR. The authors also aim to extend the study to free-breathing datasets that have been segmented prior to registration.
Conclusions: Results from linear regression of ROI data show a high correlation between Q-BH and Q-FB in apical regions of the lung in contrast to basal regions where the bias is high and correlation poor. This emphasizes the need for further investigation as early signs of many lung pathologies start in the basal regions of the lung.
Acknowledgements
No acknowledgement found.References
References: [1] Bauman et al, Eur J Radiol. 2013. Vol83(23):2371-7, [2] Till F Kaireit et al, J.Magn.Reson.Imaging,2018;47:1534-1541Figures
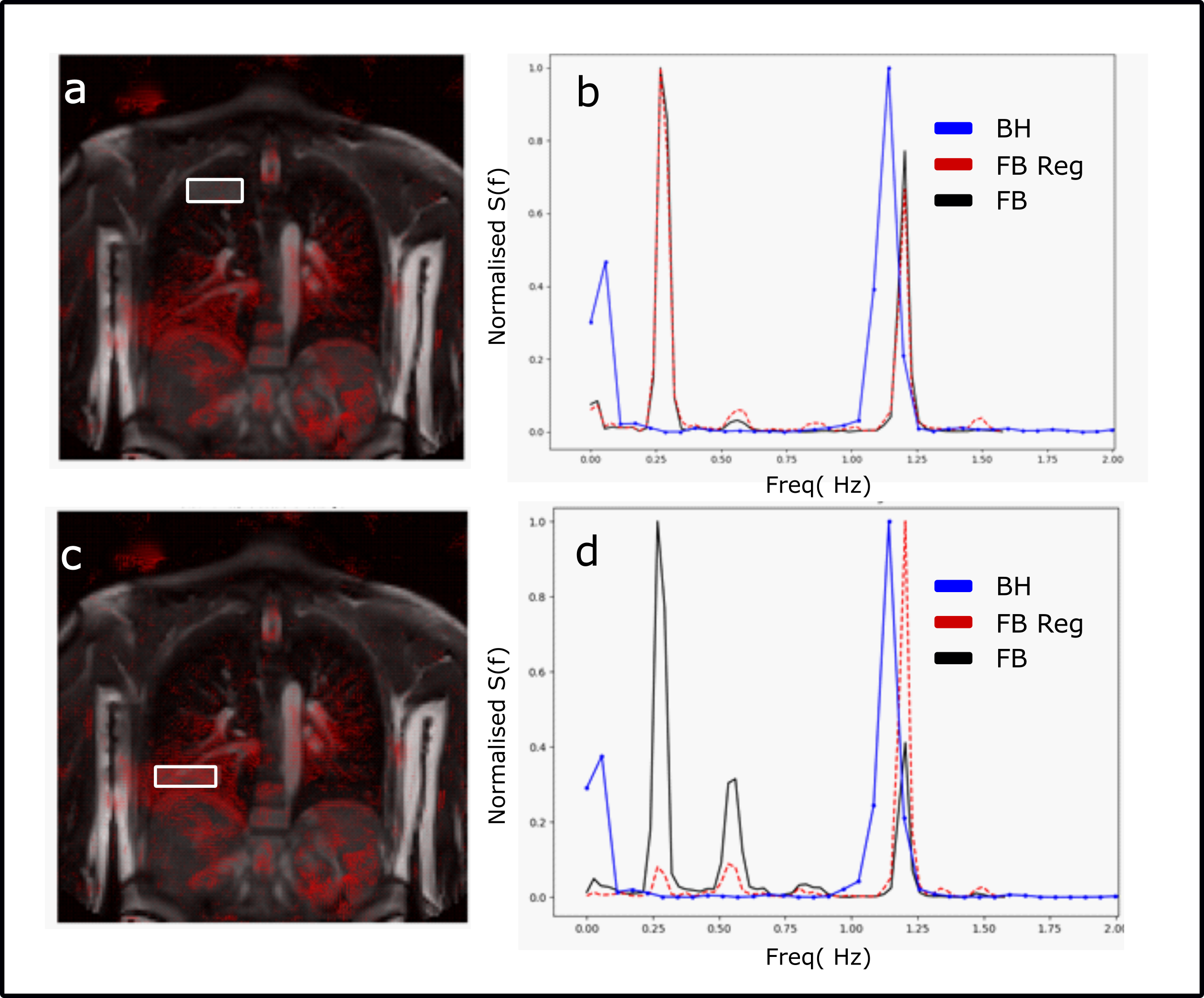
Fig 1 a) Deformation quiver map outlining ROI in b) Fourier spectra for breath-hold and free-breathing registered data of ROI in a). c) ROI in basal regions of the same subject and d) corresponding Fourier spectra. Clipped peak near 0 Hz in BH spectrum is due to steady state effects.